

We rarely discuss medico-legal issues on EM Cases because it misguides us a bit from good patient centered care – which is what emergency medicine is really all about.
Nonetheless, missed orthopedic injuries are the most common reason for an emergency doc to be sued in Canada. This is partly because missed orthopedic injuries are far more common than missed MIs for example, but it’s also because it’s easy to miss certain orthopedic injuries – especially the ones that aren’t super common. And orthopedics is difficult to learn and remember for the EM practitioner as there are so many injuries to remember.
And so, you guessed it – on this episode we’re going to run through some key not-so-common, easy to miss orthopedic injuries, some of which I, personally had to learn about the hard way, if you know what I mean.
After listening to this episode, try some cognitive forcing strategies – for every patient with a FOOSH that you see, look for and document a DRUJ injury. Wait, hold on….I don’t wanna give it all away at the top of the post.
Let’s hear what EM doc and sports medicine guru Ivy Cheng, and the orthopedic surgeon who everyone at North York General turns to when they need help with a difficult ortho case, Hossein Medhian, have to say about Commonly Missed Uncommon Orthopedic Injuries.
Written Summary & Blogpost written and prepared by Keerat Grewal and Anton Helman, Oct 2014
Cite this podcast as: Cheng, I, Medhian, H, Helman, A. Commonly Missed Uncommon Orthopedic Injuries. Emergency Medicine Cases. October, 2014. https://emergencymedicinecases.com/episode-52-commonly-missed-uncommon-orthopedic-injuries/. Accessed [date].
Quick Reference Cards for each injury discussed in this episode (click on card to view pdf)

Ch1 Lisfranc Injuries

Ch 2 Perilunate Injuries

Ch3 DRUJ injuries

Ch4 Pelvic Apophyseal Injuries
Lisfranc Injuries – Commonly Missed Uncommon Orthopedic Injuries
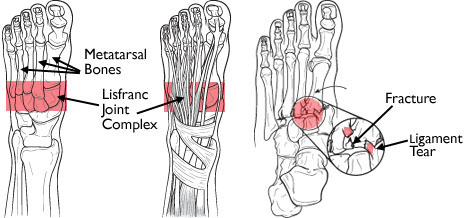
Lisfranc injuries are a spectrum of injuries, from a simple sprain to complete disruption of the tarso-metatarsal joints in the midfoot. These typically occur at the base of the 2nd metatarsal. Lisfranc injuries are easy to miss because they are very uncommon and because the x-ray findings are often subtle or even absent on standard views. Low velocity injuries are typically more commonly missed than high velocity ones. It’s these subtle, low velocity injuries that we should be on the look out for.
The usual mechanism of injury for a Lisfranc is plantar flexion with external rotation of the ankle. A classic example is a fall from a horse with the foot caught in the foot stirrup. Other examples include: MVC, foot planted in hole, awkward step off of a curb. In children, a classic history for a Lisfranc injury is the “bunk bed fracture” where a child leaps onto a bunk bed, landing on their toes with an axial load on a plantar flexed ankle.

Look for signs of compartment syndrome, which may include: parasthesias or hyperesthesia, particularly in the first dorsal webspace.
For more on compartment syndrome see Episode 28 on Vascular Catastrophes with Anil Chopra and David Carr.

Normal alignment of 2nd metatarsal on AP view

Normal alignment of the 3rd and 4th metatarsals on the oblique view
Common x-ray findings include:
- Widening – look for widening between the bases of the 1st and 2nd or 2nd and 3rd metatarsal bases. Widening >2mm is an indication for urgent surgical intervention.
- Any fracture or avulsion – look for a ‘fleck sign’, which is pathognomonic for a Lisfranc injury. This is a small bony fragment avulsed from the second metatarsal base or medial cuniform.

Lisfranc ‘Fleck Sign’ – avulsion fracture
Obtain a 30 degree oblique x-ray – this eliminates overlap of metatarsals.
Consider weight-bearing stress views, following an ankle nerve block.
Consider a CT of the foot if the x-rays still do not show an injury and you remain suspicious.[/wpspoiler][wpspoiler name=”Question 6: What is the appropriate ED management for a patient with a Lisfranc injury?”]
For an undisplaced or suspected injury without radiographic findings, place the patient in a posterior back slab. Patients should be non-weight bearing, and outpatient follow up should be arranged with orthopedics. Discharge instruction should include elevation of the leg, and warning signs of compartment syndrome of the foot.
In a significantly displaced injury or dislocation (>2mm widening at the Lisfranc joint) – immediate orthopedics referral in the ED is required for urgent surgical intervention.
Perilunate Injuries –
Commonly Missed Uncommon Orthopedic Injuries
- Scapho-lunate dissociation – a ligamentous injury with minimal clinical findings and a gap on the AP x-ray of the wrist between the scaphoid and the lunate (The Terry Thomas, or David Letterman or Madonna sign); this the most common cause of SLAC (scapholunate advanced collapse).
- Perilunate dislocation – with advancement of injury, the capitate dislocates from the lunate fossa.
- Lunate dislocation occurs with further advancement of this injury, which is a volar dislocation of the lunate out of the ‘seat’ of the capitate.
- On the AP x-ray of the wrist, think of carpal bones as flagstones that should have equal distances of 1-2mm between them. Any narrowing/overlap or widening between carpal bones should make you suspicious of a serious perilunate ligamentous injury. If you can’t ‘drive a car around the bones’ then you should suspect a perilunate injury.
- There are typically 3 smooth Gilula lines, which form arcs between the rows of carpal bones. These lines should be smooth, if there any steps or disruption of these lines, you need to consider a perilunate ligamentous injury.
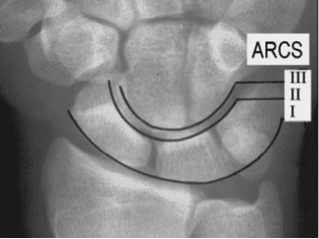
Gilula-lines on a normal AP x-ray of the wrist – any disruption in these lines should raise your suspicion for a ligamentous injury
A gap between the scaphoid and lunate on the AP x-ray of the wrist of >3mm is a scapholunate dissociation until proven otherwise. This x-ray finding has been described as The Terry Thomas Sign or The David Letterman Sign as well as The Madonna Sign as all 3 of these famous entertainers have an obvious gap between their two front teeth.

Terry Thomas or David Letterman or Madonna sign – a gap between the scaphoid and lunate on the AP view of the wrist indicating a scapholunate dissociation
On the lateral x-ray, there should be normal ‘stacking of cups’. The radius, capitate, and base of metacarpals are all look like cups and should stack on top of each other in a straight line. Assess the radio-lunate-capitate line, a vertical line through the radius, which should normally bisect the capitate. If there is not normal stacking, consider a perilunate dislocation. With further displacement of the lunate out of the seat of the capitate, the lunate appears like a ‘spilled tea cup’ and then is classified as a complete lunate dislocation.

‘Stacking of cups’ alignment of radius, capitate, lunate and 2nd metacarpal on normal lateral x-ray of the wrist

The ‘spilled tea cup’ appearance of a lunate dislocation
Clinical Pearl
A FOOSH injury + acute carpal tunnel syndrome = perilunate dislocation until proven otherwise

Reduction technique of perilunate dislocation
Post-reduction, these patients should be placed in a volar slab, in neutral position to avoid median nerve damage.
If adequate anatomical reduction is achieved, these patients require close orthopedics follow up in 1-2 days for possible operative management.
For more on periluate and lunate dislocations visit Sinai EM
Distal Radius Ulnar Joint (DRUJ) Injuries
Be suspicious of a DRUJ dislocation if:
- The ulnar styloid is more or less prominent on the affected wrist or looks displaced.
- You may feel crepitus and/or blocking on pronation or supination of the wrist.
- You may feel the ‘piano key’ sign, which is the ability to ballot the ulnar styloid.
- Look for the ulnar fovea sign, which is point tenderness over the ulnar capsule, palmar to the extensor carpi ulnaris tendon.

Ulnar Fovea Sign in DRUJ injuries
Pelvic Apophyseal Avulsion Fractures
Q: What are the common sites affected by pelvic apophyseal avulsion fractures?
The ischial tuberosity is the most common site of a pelvic apophyseal avulsion fracture that results from a sudden contraction of the hamstring muscle.
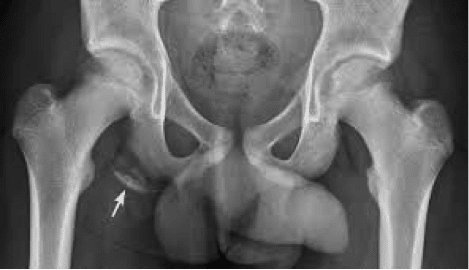
Ischial pelvic apophyseal avulsion fracture
Other Pelvic Apophyseal Injuries include:
- iliac crest avulsion
- anterior superior iliac spine (ASIS) avulsion
- anterior inferior iliac spine (AIIS) avulsion
- greater trochanter avulsion
- lesser trochanter avulsion
![]() For more on missed orthopedic injuries on EM Cases:
For more on missed orthopedic injuries on EM Cases:
Episode 1 Occult Fractures and Dislocations
Episode 58 Tendon and Ligament Commonly Missed Uncommon Orthopedic Injuries
For more on Orthopedic Pearls & Pitfalls download our free interactice eBook EM Cases Digest Vol.1 MSK & Trauma
Dr. Helman, Dr. Mehdian and Dr. Cheng and no conflicts of interest to declare.
Key References
- Anderson, RB, Hunt, KJ, & McCormick, JJ. Management of common sports-related injuries about the foot and ankle. 2010. J Am Acad Orthop Surg, 18(9): 546-56. Abstract
- Caswell, F & Brown C. Identifying foot fractures and dislocations. 2014. Emerg Nurse, 22(6): 30-4. Abstract
- Stanbury, SJ & Elfar, JC. Perilunate dislocation and perilunate fracture-dislocation. 2011. J Am Acad Orthop Surj, 19(9): 554-562. Abstract
- Boyd, KT, Peirce, NS, & Batt, ME. Common hip injuries in sport. 1997. Sports Med, 24(4): 273-88. Abstract
- Moeller, JL. Pelvic and hip apophyseal avulsion injuries in young athletes. 2003. Curr Sports Med Rep, 2(2): 110-5. Abstract
Now test your knowledge with a quiz.



{kind=link}
i am so ever grateful to you for the great work
This MSK episode was just great. Precisely the kind of info on these zebras that we need to bring them into our awareness and great detail on mechanisms and management. It certainty elevated my understanding of Lisfranc, as it had been my impression that this was a rare injury, requiring a considerable force, usually occurring when a driver hits something hard with the foot jammed on the brakes.
Lisfranc, as I am sure everyone knows, was Napoleon’s physician, and the metatarsal/tarsal joint was where he performed his eponymous front foot amputations (with an axe) on those soldiers unfortunate enough to have stepped on a piece of exploding ordinance.
Great work guys. We in ER practice are indebted to the entire team.
[…] EM Cases: Missed Ortho Injuries […]
Thank You for the the informative evuidence-based practice knowledge ,It adds a real life case presentation and hone the experience