

When was the last time you saw ventricular fibrillation in a 4 month old? Dr. Rob Simard tells his Best Case Ever of a Pediatric Cardiac Arrest in which meticulous preparation, sticking to his guns, early activation of the transportation service, and clever use of point of care ultrasound helped save the life of a child. He explains the importance of debriefing your team after an emotionally charged case.
Published November 2015
Dr. Simard’s tips on drawing up epinephrine in preparation for pediatric cardiac arrest
Use 3 tuberculin syringes (1mL each) and attach a 3-way stopcock to the cardiac ![]() cart epinephrine syringe and draw up 3 tuberculin syrninges of epinephrine in advance.
cart epinephrine syringe and draw up 3 tuberculin syrninges of epinephrine in advance.
Annals of EM study on colour coded pre-filled syringes for pediatric resuscitation showing faster time to administration and lower medication error rates Full PDF
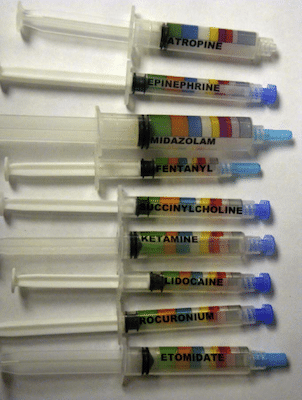
From Annals of EM
References
Moreira ME, Hernandez C, Stevens AD, et al. Color-Coded Prefilled Medication Syringes Decrease Time to Delivery and Dosing Error in Simulated Emergency Department Pediatric Resuscitations. Ann Emerg Med. 2015;66(2):97-106.e3.
Other FOAMed Resources
Debriefing in the ED on St Emlyns Blog
American College of Cardiology 2015 Update for Pediatric Life Support Guidelines Key Points
Dr. Helman & Dr. Simard of no conflicts of interest to declare
For more EM Cases content on Pediatric Emergencies check out our free interactive eBook,
EM Cases Digest Vol. 2 Pediatric Emergencies here.



Great case discussion! I would totally echo the comments on the utility of P.O.C.U.S. in paediatric pneumothorax.
I had a recent case of a crashing term neonate in the NICU with a tension pneumo. The clinical signs were all present (tachycardia, desaturation, narrowing pulse pressure, hypotension, terrible peripheral perfusion) and neither I nor the other paediatrician were able to hear any breath sounds on the right. We set up for needle decompression just as one of our nurses brought over the US. A 2 second scan with the linear probe showed beautiful lung sliding on the right. On the left however, there was no lung sliding and a clear lung point was present. The pneumo was completely on the left and resolved nicely with intervention on the correct side.
The clinical exams we talk about and look for in tension pneumo (shifted trachea, hyper resonance to percussion, elevated JVP etc) are rarely easy to assess in small babies and as I learned from this case, my ability to hear where the breath sounds are in a noisy NICU is not as good as I would like it to be. I’m pretty thankful we had the use of a bedside US.