
Topics in this EM Quick Hits podcast
Walter Himmel on new diseases associated with immune checkpoint inhibitors (00:54)
Leeor Sommer on the evolution of epiglottitis – adult epiglottitis clinical pearls (15:40)
Sarah Reid on how to pick up HSP (23:12)
Anand Swaminathan on an approach to management of heat stroke (31:02)
Justin Morgenstern on the association between pediatric Bell’s palsy and leukemia (37:12)
Podcast: Play in new window | Download (Duration: 43:59 — 40.3MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Anton Helman
Cite this podcast as: Helman, A. Morgenstern, J. Himmel, W. Sommer, L. Reid, S. Swaminathan, A, H. EM Quick Hits 32 – Checkpoint Inhibitors, Adult Epiglottis, HSP, Heat Stroke, Bell’s Palsy and Leukemia. Emergency Medicine Cases. August 2021. https://emergencymedicinecases.com/em-quick-hits-september-2021/. Accessed [date].
Checkpoint inhibitors and their immune related diseases: What we need to know about the “mabs”
- Checkpoint inhibitors (easily identified on a patient’s medication list as they end in the syllable “mab”) are immunotherapy drugs that have been shown to be effective in treating some malignancies such as melanoma
- They cause immunosuppression which can lead to inflammatory conditions such as dermatitis, colitis, myocarditis, iritis, arthritis, pneumonitis, thyroiditis and aseptic meningitis
- The first presentation of these checkpoint inhibitor related inflammatory conditions are often dermatologic (eg. eczema, DRESS syndrome, Stephens-Johnsons) usually 2-4 weeks after starting the checkpoint inhibitor or gastroenterologic (e.g. colitis); other “mab”-related disease may present months after starting the medication
- The management of these diseases usually involves stopping the checkpoint inhibitor, starting steroids and consulting their oncologist
König D, Läubli H: Mechanisms of Immune-Related Complications in Cancer Patients Treated with Immune Checkpoint Inhibitors. Pharmacology 2021;106:123-136.
The evolution of epiglottitis to an adult disease – key clinical pearls
- Epiglottitis is an adult disease: while epiglottitis has been classically taught as an acute onset, rapidly progressive pediatric emergency with obvious clinical features, in the post-H.Influenza vaccine era, epiglottitis has emerged as an uncommon (1-3 per 100,000 patient encounters) predominantly adult disease with an indolent onset (usually present on day 3 or 4 of illness) that may present to the ED with subtle findings and be more difficult to diagnose, but carries a higher mortality rate in adults than in children
- The predominant complaint is sore throat in 94% of patients, 80% dysphagia/odonophaagia, 60% fever
- The symptom that should raise your suspicion of epiglottitis is throat pain out of proportion to minimal/no pharyngeal findings
- Other useful clues include choking sensation on lying supine and “hot potato” voice
- The use of flexible nasopharyngoscopy to directly visualize the “cherry-red” swollen epiglottis is invaluable in making the diagnosis in the ED and is recommended by our expert to be a core competency skill in our training programs; direct laryngoscopy is an alternative modality to directly visualize the epiglottis
- Plain x-rays have poor accuracy for the diagnosis of epiglottitis and CT has the disadvantage of requiring the patient to leave the ED while potentially running the risk of airway compromise while outside the ED
- Shah RK, Stocks C. Epiglottitis in the United States: national trends, variances, prognosis, and management. Laryngoscope. 2010; 120:1256–1262.
- Cheung CS, Man SY, Graham CA, Mak PS, Cheung PS, Chan BC, Rhainer TH. Adult epiglottitis: 6 years experience in a university teaching hospital in Hong Kong. Eur J Emerg Med. 2009; 16:221–22.
- Ng HL, Sin LM, Li MF, Que TL, Anandaciva S. Acute epiglottitis in adults: a retrospective review of 106 patients in Hong Kong. Emerg Med J. 2008; 25:253–255. P
- Tamir, Marom, et al. Adult supraglottitis: changing trends. European Archives of oto-rhinolaryngology and Head and Neck. 2014; 272:2464.
Henoch Schonlein Purpura: The most common vasculitis in children
- HSP is the most common pediatric vasculitis generally seen in children <10 years of age
- Two important sources of morbidity are kidney involvement (about 1% of kids go on to end stage renal disease and some develop hypertension) and intussusception (the rash of HSP may appear after the abdominal pain)
- The diagnosis of HSP is based on the presence of:
- Palpable purpura or petechiae (without thrombocytopenia) with lower limb predominance plus at least 1 of:
- 1. Diffuse abdominal pain
- 2. Acute arthritis or arthralgia
- 3. Any biopsy showing predominant IgA (skin, kidney)
- 4. Renal involvement (any hematuria or proteinuria)
- Initial investigations in ED: weight, height, BP (there are tables of normal BP for kids based on gender, age, height), CBCD, coags, BUN, Cr, albumin, total protein; urinalysis, throat swab, ASOT (if current/recent sore throat)
- Admit if severe abdominal pain, volume depletion – sometimes these children are treated with short course of oral steroids
- Patients with HSP who are discharged from the ED require close follow-up for development of hypertension and renal dysfunction
- Trnka P. Henoch-Schönlein purpura in children. Journal of Paediatrics and Child Health 49 (2013) 995–1003.
- McCarthy HJ, Tizard EJ. Diagnosis and management of Henoch-Schonlein purpura. Eur J Pediatr (2010) 169:643-650.
- Hahn D, Hodson EM, Willis NS, Craig JC. Interventions for preventing and treating kidney disease in Henoch‐Schönlein Purpura (HSP). Cochrane Database of Systematic Reviews 2015, Issue 8. Art. No.: CD005128.
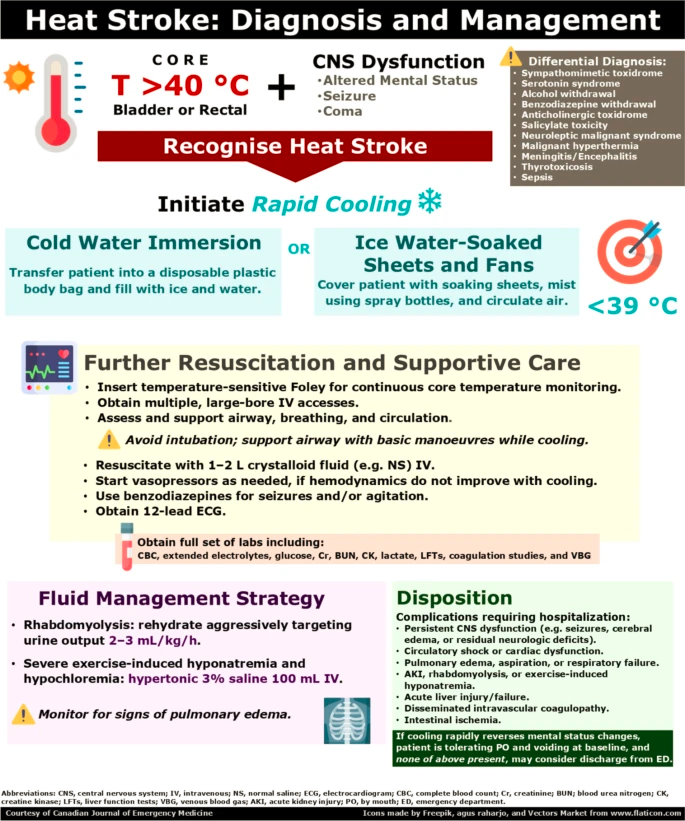
Recognition and management of heat stroke
- Heat stroke is an elevated body temperature (typically >105 degrees F) that results from a failure to handle intrinsic and extrinsic heat generation leading to multiorgan failure characterized by altered mental status
- Obtaining a core temperature (rectal or esophageal) is key to recognition of heat stroke as surface temperatures obtained at triage may be inaccurate and/or misleading; continuous core temperature monitoring is required
- Early initiation of rapid cooling measures is perhaps the most important aspect of treatment as the longer patients with heat stroke remain hyperthermic, the worse the outcomes
- Immersion in icewater bath is probably the most effective rapid cooling method (use a bodybag with enough ice cubes and cold water to cover the patients skin from the neck down) with the goal of 101 degrees F (38.3 degrees C) core temperature; you may need to ask someone to run to the hospital cafeteria ice machine to get enough ice if you do not have an ice in your ED
- Dysrhthmias associated with heat stroke usually do not resolve until normothermia is achieved
- Some patients may have concomitant sepsis, so it is not unreasonable to cover with broad spectrum antibiotics in unclear cases
- Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
- Tran TP. Heat emergencies. In: Ma OJ, Cline DM, ed. Emergency medicine manual. 6th ed. McGraw-Hill, NY: 2004:564-565.
Underlying causes of Bell’s palsy in children
- There are many etiologies of pediatric Bell’s palsy besides benign viruses including Ramsay Hunt syndrome, tubercolosis, Lyme disease, rubella, mumps, HSP, Kawasaki, rhabdomyosarcoma and parotid gland tumors
- A recent triple blind multicenter trial of steroids in children with peripheral facial palsy found that 0.8% of these patients had Leukemia as an underlying cause with most of them being a novel diagnosis of leukemia
- Consider obtaining a screening CBC in children who present with Bell’s palsy to screen for leukemia as steroid therapy typically given for Bell’s may trigger a tumor lysis syndrome on those who have occult leukemia as the underlying casue of the palsy.
![]()
Update 2022: A randomized controlled trial of 187 children (between 6 months to 18 years old) with Bell’s palsy presenting within 72 hours of onset found no difference in 1 or 3 month facial motor function recovery between those who received prednisolone (1mg/kg/day) and placebo. Abstract
- Babl FE, Kochar A, Osborn M, Borland ML, West A, Williams A, Dalziel SR; PREDICT network. Risk of Leukemia in Children With Peripheral Facial Palsy. Ann Emerg Med. 2020 Aug 9:S0196-0644(20)30491-1.
None of the authors have any conflicts of interest to declare



Dear Walter and Anton;
As a medical oncologist and regular listener to your podcast I really enjoyed your segment on immune checkpoint inhibitors!
I would add that the indications for immune checkpoint inhibitors have widely expanded recently and they are increasingly being utilized as part of definitive or adjuvant treatments for cancer with curative intent (not just later line / palliative intent as was stated). Therefore we shouldn’t automatically associate checkpoint inhibitors with a poor long-term prognosis these days — in some cases the cancer will have already been cured while the pt is receiving an ICI.
Keep up the great work!
Tom
Dear Dr Anton I really enjoy reading everything u post here..Excellent and exceptional work.Working in a remote Island County as Fiji ILearn a lot from everything you update here.
Thank you ????.
Which monoclonal antibodies only change the Timor cell so it no longer self ?