
In the ED, we often care for patients who arrive tachycardic, altered, febrile, or in heart failure. Most of the time the diagnosis is familiar — sepsis, intoxication, or primary cardiac disease. But occasionally the cause is endocrine, and when it’s missed, the consequences may be significant. Thyrotoxicosis is common; thyroid storm is not. Yet when it occurs, it is one of the most time-critical and easily missed emergencies we face. In this EM Cases episode with guest experts Dr. Alyssa Louis and Dr. George Willis, we focus on recognizing thyroid storm when it doesn’t look “stormy.” While younger patients may present with classic hyperadrenergic features, older adults often present quietly — with apathy, confusion, new atrial fibrillation, or heart failure out of proportion to the story. These are the patients we anchor on as septic or delirious, where delays in treatment drive mortality. This episode zeroes in on bedside decision-making and high-risk pitfalls: why TSH can mislead you in a crashing patient, when tachycardia is compensatory rather than dangerous, and how the wrong β-blocker can precipitate cardiovascular collapse. We walk through how PoCUS should guide early β-blockade, when to treat before labs return, and why the medication sequence in thyroid storm is important. We answer these questions: When a patient presents with “sepsis without a source,” what bedside features should trigger you to prioritize thyrotoxicosis? How can PoCUS help you decide whether tachycardia is dangerous — or lifesaving — before starting β-blockade? Why can TSH and free T4 be falsely reassuring in a crashing patient, and what labs actually matter early? In which patients does propranolol increase the risk of cardiovascular collapse — and why is esmolol the safer first line medication? Why does the order β-blocker → thionamide → steroid → iodine matter, and what happens if you get it wrong? When is not giving a β-blocker the safest decision in thyroid storm, even in a profoundly tachycardic patient? In an agitated, hyperthermic patient with thyrotoxicosis, why might intubation be more dangerous than helpful in the first hour? How does amiodarone-induced thyrotoxicosis fundamentally change your management — and why can iodine make it worse? and many more…
Podcast: Play in new window | Download (Duration: 1:13:18 — 67.2MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Anton Helman December, 2025
Cite this podcast as: Helman, A. Louis, A. Willis, G. Thyrotoxicosis and Thyroid Storm Recognition and Management. Emergency Medicine Cases. Decemeber, 2025. https://emergencymedicinecases.com/thyrotixicosis-thyroid-storm. Accessed June 14, 2026
Why thyrotoxicosis and thyroid storm matter
Hyperthyroidism affects approximately 1.2% of the population, but when it decompensates into thyroid storm, mortality rises into the double digits without prompt treatment. Thyroid storm is therefore a rare but time-critical endocrine emergency.
Importantly, thyroid storm does not always present with dramatic hyperadrenergic features. While younger patients may appear overtly “stormy,” older adults often present subtly, mimicking more common ED diagnoses such as sepsis, heart failure, or delirium. Emergency clinicians must maintain a high index of suspicion, particularly in patients with “sepsis without a source” or new, difficult-to-control atrial fibrillation.
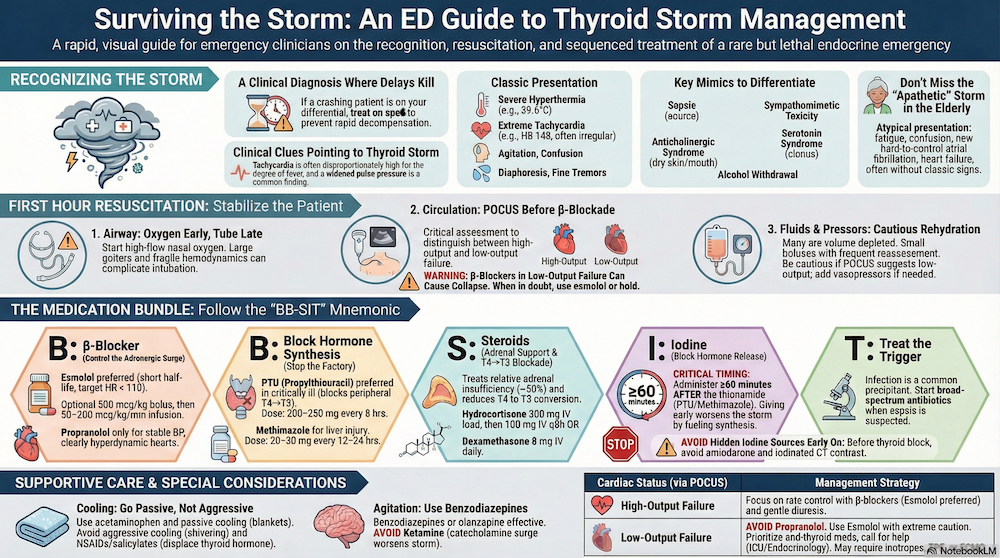
Clinical Recognition: Thyroid Storm Versus Mimics
Classic Thyroid Storm
Typical features include:
- Hyperthermia
- Tachyarrhythmias, commonly atrial fibrillation
- Agitation or altered mental status
- Widened pulse pressure
Atrial fibrillation occurs in approximately 10–35% of patients with thyrotoxicosis. While exophthalmos may be present in Graves’ disease, it does not correlate with biochemical severity, and a goitre may be absent.
Apathetic Thyrotoxicosis (Older Adults)
In older patients, thyroid storm may present without classic “hyper” features:
- Fatigue or apathy
- Depression or confusion
- Profound weight loss and muscle wasting
- Mild tachycardia or new atrial fibrillation
- Congestive heart failure
- Often no fever or agitation
Mortality is higher when this presentation is missed.
Pearl: A quiet older patient with new atrial fibrillation, CHF out of proportion to the story, or “sepsis without a source” should prompt consideration of thyrotoxicosis—even in the absence of fever or agitation.
Sorting out the differential diagnosis at the bedside
When evaluating the undifferentiated tachyarrhythmic or altered patient/febrile patient:
- Dry mouth and urinary retention → anticholinergic toxidrome
- Clonus or hyperreflexia → serotonin syndrome
- Seizures with alcohol history → withdrawal
- New, stubborn atrial fibrillation or sepsis without a source → prioritize thyrotoxicosis and initiate the storm bundle
ED Workup of suspected thyrotoxicosis/thyroid storm: Think beyond TSH and free T4
Don’t wait for TSH/T4 in a crashing patient; they can be delayed or even misleading (rarely normal/slightly ↑ TSH). Never use TSH to rule out storm in a crashing patient.
Consider:
- Free T3 in those with atypical TSH/T4 levels
- Calcium
- Liver function tests (helps inform thionamide choice)
- Cortisol (up to half of patients may have relative adrenal insufficiency, supporting empiric stress-dose steroids)
- ECG, troponin, BNP (heart failure is a common complication of thyroid storm)
- Sepsis and toxicology workup as indicated
When to treat suspected thyrotoxicosis on speculation before labs return
If a patient is:
- Hyperthermic
- Profoundly tachycardic (often atrial fibrillation)
- Altered
- With a history suggestive of Graves’, recent iodine load (contrast, amiodarone), or missed anti-thyroid medications
Start therapy immediately. Delay in treatment is associated with increased mortality. Laboratory confirmation should never delay initial management in a crashing patient.
Thyroid Storm Scoring Systems: Strengths and Limitations
Burch–Wartofsky Point Scale (BWPS)
- Assigns points for temperature, CNS effects, tachycardia, heart failure, GI symptoms, and precipitating events
- ≥45: strongly suggests thyroid storm
- 25–44: impending storm
- <25: argues against storm
BWPS can help legitimize early empiric therapy, particularly before labs return, but may overcall storm in septic or delirious patients.
Japan Thyroid Association (JTA) Criteria
- Requires biochemical thyrotoxicosis plus CNS involvement and ≥1 systemic feature (fever, tachycardia, heart failure, or GI/hepatic dysfunction)
- More specific but less sensitive
- Useful once labs are available
Practical take on thyroid storm scoring systems
BWPS can raise suspicion and legitimize early treatment (especially before labs return). JTA helps confirm once you have labs. Neither should delay β-blocker → thionamide → steroid → (1 h) iodine.
Pathophysiology of thyroid storm to guide therapy
It’s not just absolute hormone levels—it’s the rate of rise plus tissue sensitivity and sympathetic dysregulation that crash patients. T3 is the potent hormone, mostly generated peripherally from T4, which is why therapies that block conversion matter. Thyroid hormone upregulates β-receptors and oxygen demand across systems—hence the tachyarrhythmias and heat.
Thyroid storm and first-hour resuscitation and stabilization: Calming the Storm
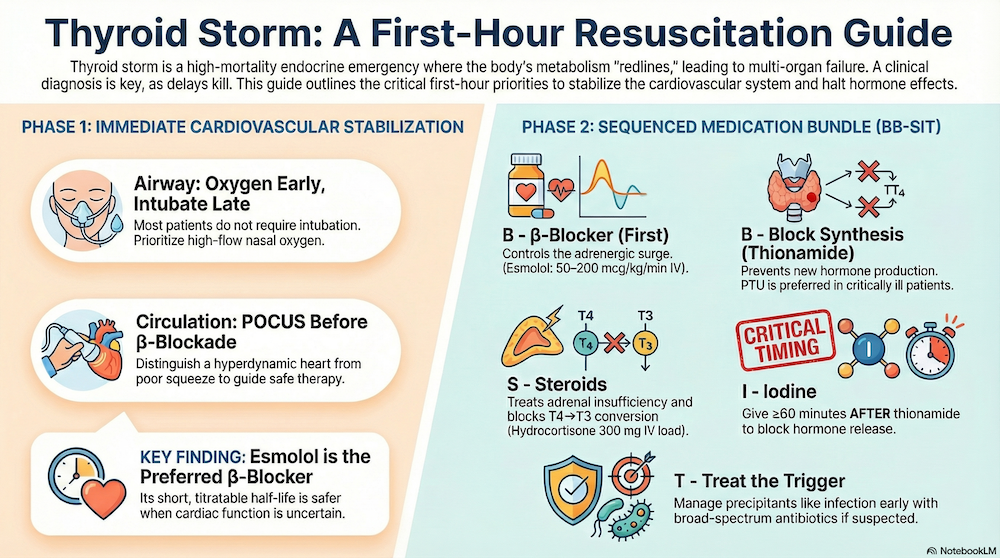
Airway Management in Thyroid Storm: Oxygen Early, Tube Late
Most patients do not require immediate intubation.
- Large goitres and airway edema can complicate anatomy
- Hemodynamics are usually fragile post-RSI
Preferred approach:
- High-flow nasal oxygen
- NIV only if the patient is calm and cooperative (uncommon in thyroid storm)
Circulation: PoCUS before β-blockade in thyroid storm
Stabilize the cardiovascular system while you start the anti-thyroid bundle.
You don’t need a perfect EF on PoCUS—just distinguish hyperdynamic vs poor squeeze to guide β-blockade.
PoCUS to determine:
- Hyperdynamic/high-output physiology
- Low-output cardiogenic failure
This distinction is critical, as β-blockade can precipitate cardiovascular collapse in low-output states. Case reports describe low-output cardiac failure patients crashing after a single IV propranolol dose.
Fluids/Pressors: Many patients are volume depleted (hypermetabolic, febrile diuresis, vomiting). Small bolus, frequent reassessments, and be more cautious if your PoCUS suggests low-output failure. Add vasopressors if needed.
β-blocker strategy: “A brake you can undo”
Esmolol (preferred in most patients)
- Short half-life, rapid titration on/off
- Ideal when EF or hemodynamics are uncertain
- Target HR <110 (especially in high-output physiology)
Esmolol dose in thyroid storm:
- Optional bolus: 500 mcg/kg IV
- Infusion: 50–200 mcg/kg/min IV
Propranolol
- Strongest blocker of T4→T3 conversion
- Acceptable only when cardiac function is clearly hyperdynamic and BP is stable
- Higher risk if EF is depressed
Propranolol dose in thyroid storm:
-
0.5–1 mg IV every 2–5 min, maximum 10 mg
Pitfall: Tachycardia may be compensatory in low-output failure. Blasting the patient with propanalol may lead to cardiovascular collapse. When in doubt, start esmolol or hold β-blockade until cardiac function is clarified. The safest brake is one you can release. In the undifferentiated or borderline-EF patient, esmolol lets you test the waters and turn it off fast if perfusion drops.
Thyroid storm medication sequence: BB-SIT mnemonic
Order matters. Think Beta-blocker → Block synthesis (thionamide) → Steroid → (after ≥60 min) Iodine → Treat the trigger.
1. β-Blocker (first)
As above (esmolol preferred).
2. Block Hormone Synthesis (Thionamide)
Both agents may be given PO, NG, or rectally.
PTU (Propylthiouracil)
- Advantages: Blocks synthesis and peripheral T4→T3 conversion
- Dose: 200–250 mg PO/NG/PR every 8 hours
- Avoid in significant liver disease
- Preferred in critically ill patients when hepatic function allows
Methimazole
- Advantages: Less hepatotoxic, longer half-life
- Dose: 20–30 mg PO/NG/PR every 12–24 hours
- Avoid in first-trimester pregnancy
- Preferred in patients with liver injury
3. Steroids (Adrenal Coverage + T4→T3 Blockade)
- Treat relative adrenal insufficiency (seen in ~50%)
- Reduce peripheral conversion of T4→T3
- Blunt systemic inflammation
-
Hydrocortisone dose:
- 300 mg IV loading dose
- Then 100 mg IV every 8 hours
-
Alternative:
-
Dexamethasone 8 mg IV daily
-
4. Iodine (Block Hormone Release)
Timing is critical: administer ≥60 minutes after the thionamide to avoid Jod-Basedow (worsening synthesis).
-
- Administer ≥60 minutes after thionamide
- Dose every 6 hours to maintain effect
Avoid iodine if:
-
- Amiodarone-induced thyrotoxicosis
- Toxic multinodular goitre
Hidden iodine sources to avoid early:
- Amiodarone
- Iodinated CT contrast (contains >50× pharmacologic iodine dose)
If iodine is contraindicated or not tolerated, lithium may be considered in consultation with Endocrinology.
5. Treat the trigger early
- Infection (common): start empiric antibiotics when appropriate
- Withdrawal, trauma, surgery, medication non-adherence
Pitfall: Iodine timing is important. Give thionamide first, then iodine ≥60 min later. Mind the hidden iodine. Amiodarone and iodinated contrast can undermine your plan—avoid until the thyroid is blocked (unless truly time-critical).
Supportive Care: Fever and Agitation Management in Thyroid Storm
Fever
- Acetaminophen
- Passive cooling only (avoid aggressive cooling!)
- Avoid NSAIDs and salicylates (increase free hormone levels)
Agitation
- Benzodiazepines or olanzapine as needed, avoid haloperidol
- Avoid Ketamine as it may exacerbate the hypermetabolic state and agitation
Fluids
- Often volume depleted
- Small boluses with reassessment
- Caution if low-output physiology on PoCUS
Thyroid storm, atrial fibrillation, and heart failure: A therapeutic challenge
Atrial fibrillation is common in thyrotoxicosis and thyroid storm and associated with worse outcomes.
High-Output Failure
- Hyperdynamic LV, small collapsible IVC
- β-blocker (often esmolol) + cautious diuresis
Low-Output Failure
- Depressed EF, plethoric IVC
- Hold β-blocker
- Initiate inotrope (dobutamine or milrinone)
- Consider early mechanical circulatory support and plasma exchange in refractory cases
Special Situations: Pregnancy, Amiodarone, and Drug Routes in Thyroid Storm
- Pregnancy: Avoid methimazole in the first trimester; use PTU early then switch later as appropriate.
- Amiodarone toxicosis & multinodular goitre: Avoid iodine; it may worsen the pathophysiology.
- Alternative routes: Both methimazole and PTU can be given NG or rectal if oral isn’t possible.
Practical bedside algorithm for recognition and management of thyrotoxicosis and thyroid storm
Recognition & first moves
- Consider storm in hot, tachyarrhythmic, altered patients or “sepsis without a source.”
- Don’t rush to intubate. HFNC first; NIV only if the agitated patient tolerates it; be wary of difficult airways (goitre).
- Bring PoCUS—decide hyperdynamic vs poor squeeze before pushing β-blockers.
Rate, pump, and fluids
- Esmolol for most; propranolol only if clearly high-output and BP ok. Goal HR <110 (especially in high-output).
- Small, reassessed fluid boluses—these patients are often volume down; be cautious if low-output physiology.
BB-SIT sequence
B: Esmolol drip (reversible) first.
B: Thionamide next (PTU if critically ill without liver disease; methimazole safer in liver disease; avoid methimazole in 1st trimester). NG/PR if NPO.
S: Hydrocortisone (or dex if needed) for adrenal cover + conversion block.
I: Iodine ≥60 min after thionamide; q6 h; watch for amiodarone/contrast iodine loads; avoid in amiodarone-induced or multinodular thyrotoxicosis; lithium is a backup (Endo call).
T: Trigger treatment in parallel (often infection).
Hidden traps
- Amiodarone and CT contrast can silently derail your medication timing—avoid until ≥1 h after thionamide when possible.
- Propranolol in low-output failure can crash the patient—esmolol first or hold until you understand the pump.
Take home points for recognition and management of thyrotoxicosis and thyroid storm
- Consider storm in: hot, agitated, tachyarrhythmic patients; AF difficult to rate-control; “sepsis without source”; new dilated cardiomyopathy.
- Do not wait for TSH/T4 in a crasher; order free T3, Ca, LFTs, cortisol, ECG/troponin/BNP, sepsis/tox labs.
- PoCUS early to separate high- vs low-output failure before committing to β-blockade.
- Start BB-SIT: Esmolol drip first (test dose if uncertain), then thionamide, hydrocortisone 300 mg → 100 mg q8h (or dex 8 mg), then iodine ≥60 min later, q6h. Treat triggers.
- Supportive care: Acetaminophen + passive cooling; avoid NSAIDs/salicylates; benzodiazepine/olanzapine for agitation as needed.
- Consult early: Endocrinology/ICU, consider TPE and ECMO/Impella in refractory cardiogenic shock.
- Don’t crash the low-output heart. In depressed EF, hold β-blocker and start inotrope; use esmolol only if you can turn it off quickly under PoCUS guidance. Treating tachycardia reflexively with long-acting β-blockers in low-output states → cardiogenic shock. Prefer esmolol or no β-blocker until your PoCUS says it’s safe.
- Apathetic = deadly. In older patients with AF, CHF, weight loss, confusion but no fever, storm is still on the table.
- TSH can mislead. Rarely, TSH is normal or slightly ↑; never use it to rule out storm in a crashing patient.
- Rate control: Esmolol test dose/drip wins for reversibility; propranolol only in clear high-output profiles. Goal HR <110.
- Aspirin/NSAIDs for fever → worsen thyrotoxicosis (protein-binding displacement, catecholamine surge). Use acetaminophen.
- Iodine before thionamide → exacerbation via Jod-Basedow. Wait ≥60 min after thionamide.
- Anchoring on sepsis when it’s storm: if it’s “sepsis without a source”, order TSH/free T4/free T3 and start the storm pathway in parallel when suspicion is high.
References
- Farooqi S, Raj S, Koyfman A, Long B. Thyroid storm. Am J Emerg Med. 2023;69:127-135. (Background, epidemiology, management overview)
- Idrose AM. Acute and emergency care for thyrotoxicosis and thyroid storm. Acute Med Surg. 2015;2(3):147-157. (Signs, supportive care)
- Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343-1421. (Guideline perspective, clinical judgment with BWPS/JTA)
- Satoh T, Isozaki O, Suzuki A, et al. 2016 Guidelines for the management of thyroid storm (Japan Thyroid Association/Endocrine Society). Endocr J. 2016;63(12):1025-1064. (JTA diagnostic/management criteria)
- Elendu C, Amaechi DC, Amaechi EC, et al. Diagnostic criteria and scoring systems for thyroid storm: comparative review. Medicine (Baltimore). 2024;103(13):e37396. (BWPS vs JTA comparison)
- Lee SY, Modzelewski KL, Law AC, et al. Comparison of propylthiouracil vs methimazole for thyroid storm in critically ill patients. JAMA Netw Open. 2023;6(4):e238655. (Thionamides in storm; no mortality difference)
Drs. Helman, Willis and Louis have no conflicts of interest to declare
Now test your knowledge with a quiz.
Leave A Comment