

While knowledge acquisition is vital to developing your clinical skills as an EM provider, using that knowledge effectively for decision making in EM requires a whole other set of skills. In this EM Cases episode on Decision Making in EM Part 2 – Cognitive Debiasing, Situational Awareness & Preferred Error, we explore some of the concepts introduced in Episode 11 on Cognitive Decision Making like cognitive debiasing strategies, and some of the concepts introduced in Episode 62 Diagnostic Decision Making Part 1 like risk tolerance, with the goal of helping you gain insight into how we think and when to take action so you can ultimately take better care of your patients.
Walter Himmel, Chris Hicks and David Dushenski answer questions such as: How do expert clinicians blend Type 1 and Type 2 thinking to make decisions? How do expert clinicians use their mistakes and reflect on their experience to improve their decision making skills? How can we mitigate the detrimental effects of affective bias, high decision density and decision fatigue that are so abundant in the ED? How can we use mental rehearsal to not only improve our procedural skills but also our team-based resuscitation skills? How can we improve our situational awareness to make our clinical assessments more robust? How can anticipatory guidance improve the care of your non-critical patients as well as the flow of a resuscitation? How can understanding the concept of preferred error help us make critical time-sensitive decisions? and many more important decision making in EM nuggets of wisdom…
Podcast: Play in new window | Download (Duration: 1:04:35 — 59.2MB)
Subscribe: Apple Podcasts
Podcast recording April 2015
Written summary and blogpost by Anton Helman (@EMCases), Jan 2016
Cite this podcast as: Helman, A, Himmel, W, Hicks, C, Dushenski, D. Decision Making in EM – Cognitive Debiasing, Situational Awareness & Preferred Error. Emergency Medicine Cases. January, 2016. https://emergencymedicinecases.com/decision-making-in-em/. Accessed [date].
Type 1 & Type 2 Cognitive Decision Making Systems & The Nature of Expertise
“The definition of experience is the capacity to make more and more mistakes with increasing confidence” – Walter Himmel
- Type 1: The Intuitive/Reflexive System involves automatic decision making based on pattern recognition. It’s fast and requires little effort.
- Type 2: The Analytical/Problem-Solving System is more critical and logical. It involves stepping back and thinking more carefully about the patient’s presentation. It involves estimating pretest probabilities, continuous self-questioning, and considering alternative diagnoses.
The traditional view of this decision making in EM model is that while reasoning will invariably try to default to the Type 1 intuitive/reflexive approach, the most economical and fastest mode, the key to successful decision making is to step back and think analytically when you realize that there are subtle inconsistencies that arise.
The current view of this decision making in EM model is that it’s not a matter of whether Type 2 is better than Type 1 but rather, how expert decision makers blend these two systems. Experts use their experience and past errors/mistakes to reflect on their knowledge and their biases and develop heuristics (cognitive short-cuts) and cognitive forcing strategies that allow them to use their Type 1 system for rapid decision making in EM rather than having to slow down using their Type 2 system.
The Nature of Expertise
“Experts tackle problems that increase their expertise, whereas non-experts tend to tackle problems for
which they do not have to extend themselves.” – Carl Bereiter
Decision making in EM expertise comes about, not only through the acquisition of knowledge and gaining experience, but by actively using the knowledge they’ve acquired wisely. How does do we use knowledge wisely?
1. Reflect on your experience – learn from your mistakes by
- following up on all but your trivial cases within a few days
- developing your own personal heuristics based on on your experience
- consider dictating your chart which forces you to reflect on your assessment and plan
- before signing off the chart ensure that it has internal congruence – look for disconfirming evidence before you decide on a disposition
AND
2. Understand your personal cognitive biases and your particular system’s biases
3. Employ cognitive debiasing strategies based on 1 and 2
* note that only using your experience without reflection can result in excessive confidence and insecurity which may lead to more errors
“It’s not what you know, it’s what you use– how do you use your knowledge? By developing better heuristics” – Walter Himmel
Cognitive Biases discussed in this Decision Making in EM Episode
- Anchoring bias – locking on to a diagnosis early in the assessment and failing to adjust to new information
- Diagnosis momentum – accepting a previous diagnosis without considering the differential diagnosis adequately
- Confirmation bias – looking for evidence to support a pre-conceived opinion, rather than looking for dis-confirming information
- Premature closure – once you have found one diagnosis (eg: a fracture on a set of x-rays) you stop to searching for others (eg: the second fracture on the same set of x-rays)
Cognitive De-biasing Strategies: Cognitive Forcing Strategies & Heuristics
“Perception is not a passive process. Perception is an active one” – Walter Himmel
In order to identify and help mitigate some of these negative cognitive biases it is not enough to identify them. We must employ cognitive de-biasing strategies for effective decision making in EM.
Cognitive Forcing strategies can be general such as “rule out the most deadly diagnosis” or they can be be related to your own experience based on reflection on previous mistakes.
Examples of Cognitive Forcing Strategies discussed in this Decision Making in EM Episode
Missing trifascicular block on ECG – for any ECG that shows a Right Bundle Branch Block (RBBB), if the axis is pointing left then search for the findings of trifascicular block
Missing a Maisonneuve fracture – For any ankle injury, examine the proximal fibula for tenderness to assess for a Maisonneuve fracture
One important aspect of effective cognitive forcing strategies is to apply them across all clinical encounters of that kind.
Strategies to Mitigate Affective Bias & Decision Fatigue
- Overlapping shift start times where the next doc arrives an hour before the first doc finishes
- Casino shifts – preserves the anchor period (2am-6am when it is the most important for your circadian rhythm to get some sleep in order to adjust properly) and is associated with more total sleep, reduced sleep debt, shorter recovery time, reduced cognitive impairment, improved work performance and improved career longevity (listen to Episode 11 for details)
- Mutual support of colleagues working at the same time, having 2 or more physicians at each resuscitation, and ‘calling a friend’ – asking for an opinion on a case from your colleague, especially when you are at or near the end of your shift and suffering from decision fatigue
Decision Density and Anticipatory Guidance in Resuscitation Management
Human cognition has its limits. There is good evidence to suggest that our brains are not designed to function well during critical events in which multiple points of potentially unrelated information need to processed rapidly.
In critical and stressful situations we tend to ‘tunnel down’ on the task at hand and become less receptive to extraneous information that may be important. Our ability to take in this information is reduced even more when we feel high degrees of stress.
As explained below, a high performance team in which tasks and decision making responsibilities are divided up in a team huddle, having 2 doctors rather than one at every resuscitation, improving your situational awareness, and stress inoculation training can mitigate the problem of high decision density in stressful situations by cognitive unloading and managing the negative influence of stress effectively.
Mental Rehearsal & Anticipatory Guidance
Practicing or visualizing procedures ‘in your head’ (psychophysical rehearsal) before you do them has been shown to improve performance and success of procedural tasks. There is also some evidence to suggest that it may improve team performance in team-based trauma resuscitation.
The Team Huddle
Take a few minutes when you get the call from EMS about a patient who will soon be arriving in your ED to do a team huddle: predict the potential diagnoses, delegate roles, expectations and responsibilities, think about logistics in your hospital, anticipate which procedures might be necessary and set up the appropriate gear for them.
For a discussion on anticipating logistics over strategy in resuscitation go to this podcast at EMCrit
Anticipatory Guidance
There is a powerful effect on your team of stating the obvious (e.g. “this patient is in septic shock and they will get worse unless we do x, y and z”).
Anticipatory guidance and team communication is important not only in resuscitation, but in all ED patient encounters. Consider discussing with the nurse and the rest of your team what you think the most likely diagnosis is, what you’re worried about, what your management plan is and what you think the disposition might be, rather than only filling out orders for the nurses. This allows everyone to ‘be on the same page’ and may improve efficiency as well as decrease medical error.
Situational Awareness Checklist
(adapted from ‘Situational Awareness and Patient Safety – A Short Primer’ from The Royal College of Physicians and Surgeons of Canada website)
1. Get Information
- Scan and search: be proactive – look for it in your environment or solicit it from your team.
- Remain watchful: expect the unexpected
- Communicate: openly talk about your thoughts on the situation with your team, the patient and their family
2. Understand the information
- Compare: Compare the information to what you know and what you expected
- Critique: Think critically about the information – check information integrity (accuracy, completeness, source, and relevance)
3. Think Ahead
- Extrapolate and project: beyond the “now”: How will the situation unfold if the current conditions persist? Persist for how long?
- Ask “what if?”: Consider various outcomes and contingencies and communicate those possibilities to others
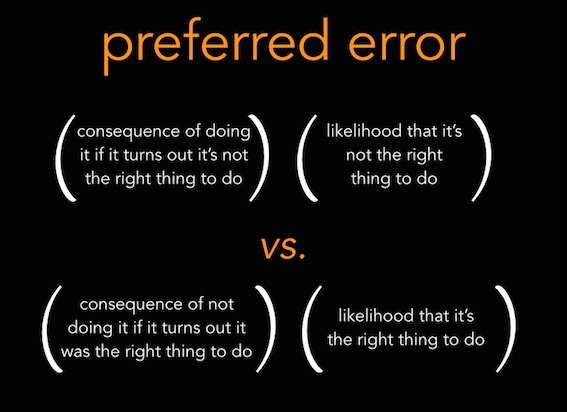
To Act or Not to Act – That is the question: Preferred error & Resilience
From emupdates by Reuben Strayer
Preferred error describes balancing the risks of action vs inaction based on the potential positive vs negative outcome of either. It begs you to consider the consequences of being wrong on both sides of the decision, and determine which course of action fails better. Factoring in how likely you are to be wrong is important in weighing the potential outcomes.
For a detailed explanation of the concept of preferred error visit emupdates
Building Resilience & Stress Inoculation Training
3 steps to building resilience
(adapted from the Harvard Business Review)
- Have an accurate understanding of the situation that you’re facing
- Give it meaning or purpose
- Be prepared to do what ever it takes regardless of the outcome, success or failure
Stress Inoculation Training
The goal of Stress Inoculation Training is to limit the impact of acute stress on performance.
Stress Inoculation Training promotes stress resilience by desensitizing the person to the negative behavioural and physiologic effects of acute stress in a simulated environment. A step-wise process involves increasingly stressful situations in a simulation training environment. During the debriefing period of the simulation the triggers of stress are identified and understood. Then, strategies to minimize the physiologic and behavioural consequences of stress are rehearsed so that the person is better prepared for similarly stressful situations.
Quote of the Month
“The value of experience is not in seeing much, but is in seeing wisely” -William Osler
![]() For more on cognitive decision making on EM Cases:
For more on cognitive decision making on EM Cases:
Episode 11: Cognitive Decision Making and Medical Error
Episode 62 Diagnostic Decision Making in Emergency Medicine
Key References on Decision Making in EM
Bereiter, C. Scardamalia, M. Surpassing ourselves: An inquiry into the nature and implications of expertise. Open Court Publishing Company. 1993, 77-120.
Chanmugam, A. Avoiding Common Errors in the Emergency Department, Chapter 78: Understand decision-making fatigue and how it influences your clinical judgement, 2010.
Crosskerry, P. The Importance of Cognitive Errors in Diagnosis and Strategies to Minimize Them. Academic Med. August 2003, 1-6.
Crosskerry, P et al. Patient Safety in Emergency Medicine. Lippincott Williams & Wilkins, 2009.
Lorello GR, Hicks CM, Ahmed SA, Unger Z, Chandra D, Hayter MA. Mental practice: a simple tool to enhance team-based trauma resuscitation. CJEM. 2015:1-7.
Petrosoniak A, Hicks CM. Beyond crisis resource management: new frontiers in human factors training for acute care medicine. Curr Opin Anaesthesiol. 2013;26(6):699-706.
Parush A, et al. Situational Awareness and Patient Safety. The Royal College of Physicians and Surgeons of Canada. 2011. Link
Scott Weingart. EMCrit Podcast 49 – The Mind of a Resus Doc: Logistics over Strategy. Link
Reuben Strayer. The Preferred Error. Emergency Medicine Updates. June 11th, 2014. Link
Dr. Helman, Dr. Hicks, Dr. Himmel & Dr. Dushenski have no conflicts of interest to declare
[ts_fab authorid=”2″ ]



[…] Cognitive debiasing, situational awareness and preferred error: decision-making analysis in an enthralling EMCases podcast. [JS] […]
Hi, great series! I just made a post in my Swedish blog about the topic and used your Picture. I hope that’s ok. I of course linked to all your podcasts.
Thanks for sharing Jonas. EM Cases content is ‘creative commons’- as long as you get our permission and aren’t making a monetary profit from it, it’s free to share!
Hi great blog post – just did one on the topic in our danish blog, Akutmedicineren.dk
Thanks for your great work!