
Hip complaints are bread-and-butter emergency medicine—but every so often they are anything but straightforward. The obvious shortened, externally rotated leg after a fall is one thing; the patient with acute hip pain, a normal x-ray, unremarkable blood work, and no clear diagnosis is another. Hip fractures are also far from benign, carrying a 30-day mortality of 6–7% and a 1-year mortality of about 20%, often triggering a cascade of pain, immobility, delirium, deconditioning, and death. But hip fractures are only the tip of the iceberg. In this EM Cases episode, Dr. Arun Sayal and Dr. Matt DiStefano go beyond “get an x-ray and call ortho” to tackle hip fractures, occult injuries, atraumatic hip pain, and hip dislocations. We answer questions like: Why do so many patients never return to baseline after a hip fracture? What can we do in the ED to avoid delaying surgery? What are the best pain management and delirium prevention strategies? Which physical exam findings help diagnose an occult hip fracture? How do we distinguish hip from pelvic fractures clinically? When is a normal x-ray not enough, and when should we proceed to CT or MRI? What is POCUS useful for in the painful hip? How should hip fractures be classified to change ED management? How should we approach atraumatic hip pain? How do native and prosthetic hip dislocations differ? What clinical position suggests posterior versus anterior dislocation? Which reduction technique should we choose? What is the Whistler technique? What are the nuances of post-reduction management? And much more.
Please consider a donation to EM Cases to support ongoing high-quality Free Open Access Medical Education: https://emergencymedicinecases.com/donation/
Podcast: Play in new window | Download (Duration: 1:25:19 — 78.2MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Sara Brade, edited by Anton Helman June, 2026
Cite this podcast as: Helman, A. DiStefano, M. Sayal, A. Ep 219 Hip Emergencies: Recognition and Management. Emergency Medicine Cases. June, 2026. https://emergencymedicinecases.com/hip-emergencies. Accessed July 26, 2026
Why hip fractures cause significant morbidity and mortality in the elderly
Hip fractures are not isolated events in older patients. They often occur in patients with low physiologic reserve and comorbidities, and once older adults begin falling, falls beget falls; the fall itself may be a sign that independence and quality of life are already threatened. The high mortality is driven less by the bone injury itself than by what can follow secondary to immobilization: delirium, pneumonia, venous thromboembolism, pressure injuries, myocardial infarction and deconditioning.
Time-to-OR targets for hip fractures
The evidence suggests best outcomes when surgery is performed within 24 hours. Outcomes worsen after 24-48 hours. There is no demonstrable benefit to targeting surgery within 6-12 hours.
Preventing delirium and delays to OR for hip fractures
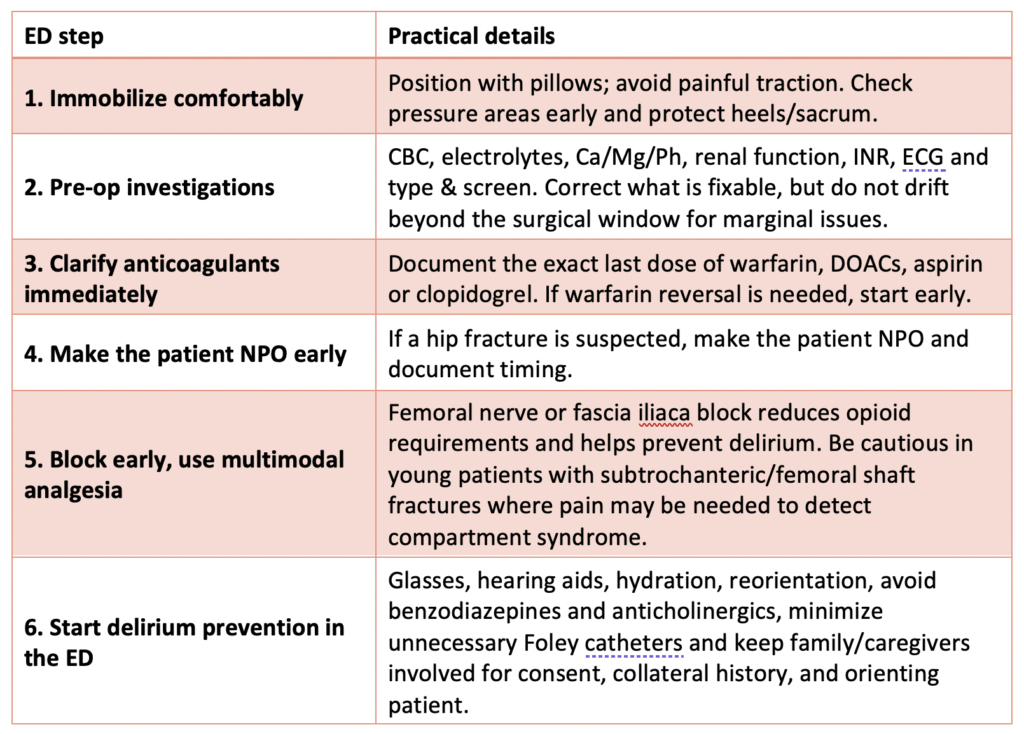
Our role in the ED is to expedite pre-OR requirements, and to prevent and remove barriers that would delay the OR. Delirium prevention is critical to improve outcomes for these patients. Steps we can take in the ED:
If the patient needs to be transferred to a different facility for surgery this process should start immediately upon diagnosis.
Optimizing analgesia in hip fractures: multimodal analgesia including regional nerve blocks
- Minimize the use of opioids as these are a major driver of delirium.
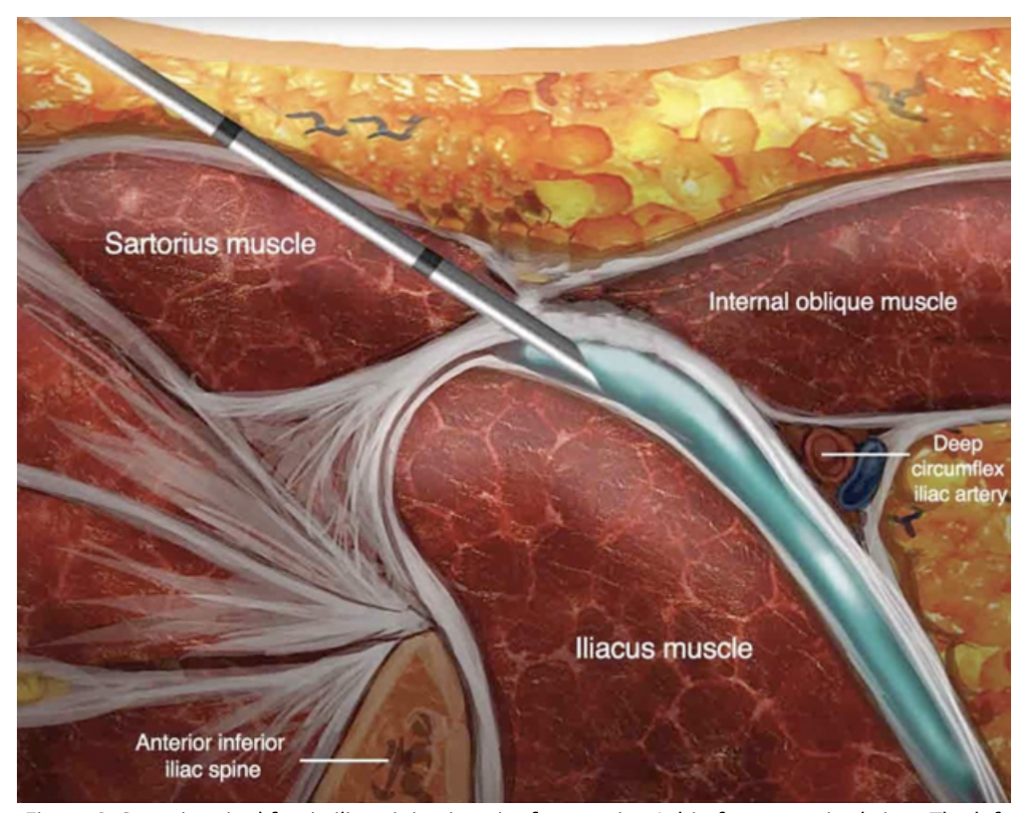
- Evidence suggests femoral nerve blocks or fascia iliaca blocks provide effective analgesia and are associated with decreased opioid use.
- Consider making hip block kits with all the supplies in one place for your ED to decrease barriers to performing this procedure.
- Avoid a dense regional block in younger patients with subtrochanteric or femoral shaft fractures where compartment syndrome is a concern, because a block could mask evolving pain.
- Procedural Tip: Pressing firmly, hold your hand on the hip a few centimetre below your block for 5 minutes to concentrate the block around the femoral nerve and minimize inferior spread.
Historical clues that raise suspicion for occult hip fracture despite a normal x-ray
- Older adult with low-energy fall, especially a sideways fall onto the painful side.
- Sudden groin pain before the fall
- Persistent groin or anterior thigh pain, night pain, or pain out of proportion to the x-ray.
- New limp, shortened stride, inability to manage stairs or rise from a chair, even if the patient can take a few steps. Patients with non-displaced femoral neck fractures and valgus-impacted fractures may present with a limp or partial weight bearing.
- Past history of osteoporosis, chronic steroid use, long-term bisphosphonate use, inflammatory disease, immunosuppression, anticoagulation or multiple/recent falls.
- Knee pain that cannot be reproduced at the knee on exam points to a more proximal or distal source of pain.
Mechanism of injury can seem minor in older adults with hip fractures
We often assume that it is a fall that causes the hip fracture. In older patients, the sequence can be reversed: the patient pivots on an arthritic, stiff hip; range of motion stops; rotational force is transferred to osteoporotic bone; the hip fractures; pain causes the fall. The patient may tell you they turned, felt or heard a crack, then fell because of pain. Do not dismiss the potential for hip fracture because the fall seems minor or because the patient did not clearly land on the hip. In older adults, low-energy or even no-clear-trauma hip fractures occur not infrequently.
Physical exam tools to diagnose occult hip fractures in the ED

Practical bedside sequence to examine for hip/pelvic pathology: inspect for deformity and bruising; locate the pain; gently log roll; gently internally and externally rotate; assess active straight-leg raise; consider axial load only if not obviously deformed; and examine the pelvis.
Bruising pattern can also help with diagnosis. Bruising over the greater trochanter should raise concern for subcapital fracture or acetabular injury. Bruising around the knee may mean the patient fell onto the knee and transmitted force up the femur into the hip. Absence of bruising does not rule anything out.
Pearl: In areas with limited access to CT, altered sound transmission on patellar-pubic percussion is a useful data point to support transfer for advanced imaging.
Patellar-pubic percussion test
Clinical clues to distinguish hip fractures from pelvic fractures
Pelvic ring injury becomes more likely when pain is more medial, with tenderness over the pubic symphysis, sacrum or iliac crests, or pain with pelvic compression. Hip fracture becomes more likely with focal hip pain, deep groin pain, lateral hip tenderness over the greater trochanter after a fall, and pain with hip rotation or log roll.
Low-energy pubic rami fractures are common and often nonoperative, but missing them still matters for analgesia, mobility planning and avoiding bounce backs.
Pitfall: Missing the second fracture: hip and pelvic fractures can co-exist.
Hip Fractures Occult to X-ray: CT or MRI?
A normal x-ray lowers the likelihood but does not eliminate the possibility of hip fracture. Roughly 2-10% of hip fractures are radiographically occult.
If clinical suspicion remains high after a normal x-ray (i.e. persistent groin pain, inability to bear weight, abnormal gait, pain with internal rotation or log roll), obtain advanced imaging. CT is fast and available and is often the practical first test. Modern multi-slice CT can pick up cortical fractures, displaced fractures, acetabular injuries, subchondral insufficiency fractures and peri-prosthetic complications, but it can still miss diagnoses that MRI can pick up: non-displaced femoral neck fractures, intertrochanteric extension of greater trochanter fractures, early marrow edema, and subchondral fractures.
MRI remains the gold standard when suspicion remains after negative CT and/or normal labs, especially in older patients with persistent inability to walk, deep groin pain, pain with internal rotation, or pain with minimal to no trauma. If MRI is not available promptly, do not simply discharge the high-risk patient because CT is negative. Admit or arrange a safe non-weight-bearing plan and repeat/advanced imaging according to local resources.
Pearl: Subchondral insufficiency fracture is essentially a stress fracture of the hip in older adults. Risk factors include sports that repetitively load the hip, and factors associated with poor bone quality like smoking, alcohol use and chronic steroids. It may present with acute groin pain, normal x-rays and pain with internal rotation without major trauma. It is often diagnosed only on CT/MRI.
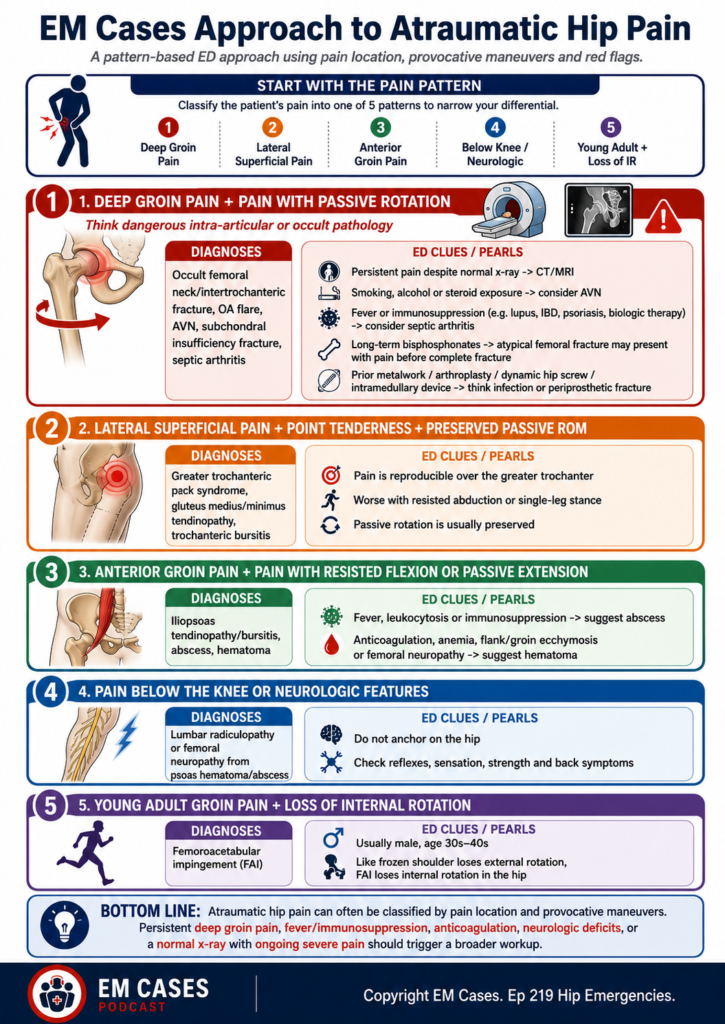
Approach to atraumatic hip pain in the ED
Not all atraumatic hip pain in older adults is osteoarthritis. Focus on duration of pain and localization to narrow down the diagnosis.
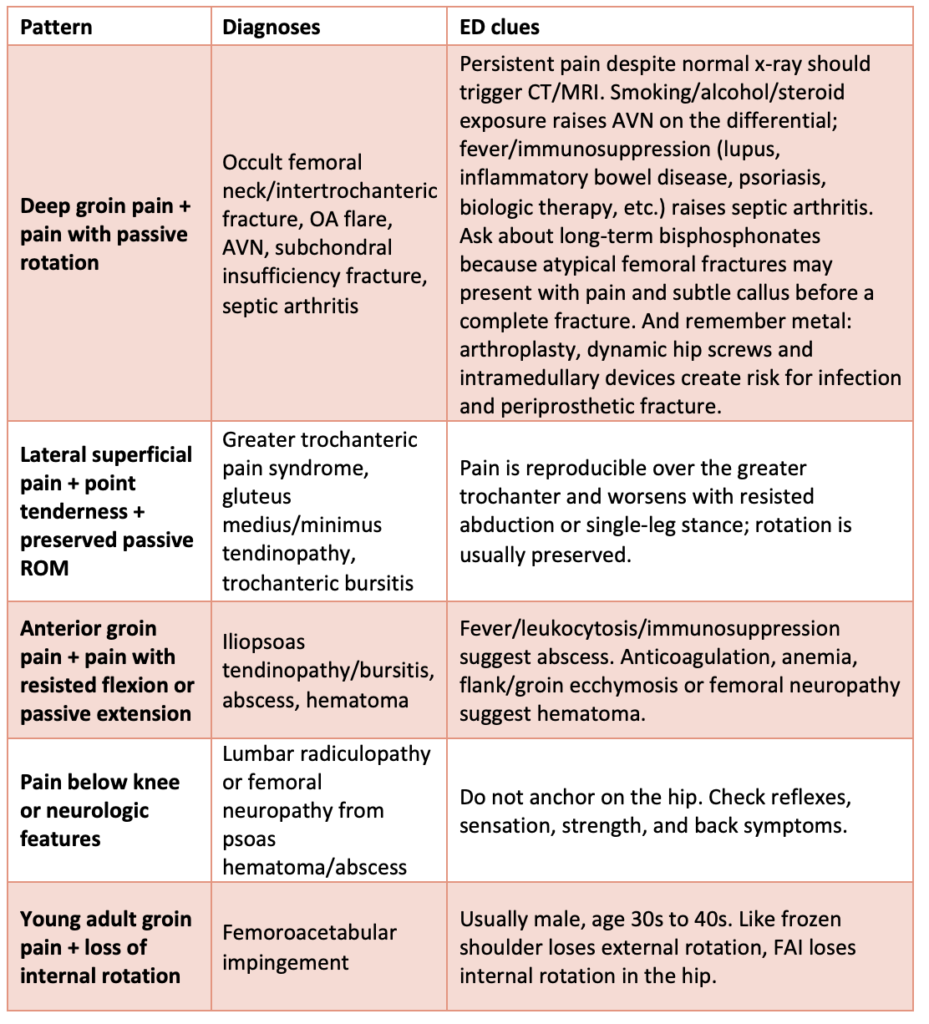
Pitfall: Assuming lateral hip pain is bursitis only. Greater trochanteric pain syndrome is analogous to rotator cuff tendinopathy. A tendon that degenerates, tears and that irritates the adjacent bursa. Bursitis may be the smoke; but tendinopathy is the fire.
PoCUS for atraumatic hip pain in the ED: identifying hip effusions
PoCUS can identify a hip effusion and guide hip aspiration when septic arthritis is suspected and interventional radiology is not available. Measure the joint space of bilateral hips; a difference of 2mm or more is significant. Absence of an anterior effusion early in disease does not completely rule out septic arthritis, and the presence of effusion is non-specific, occurring in fracture, infection (don’t forget to consider STI risk factors), inflammatory arthritis or hemarthrosis. PoCUS cannot rule out a hip fracture – sensitivity is poor.

Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC11628435/
Classification of hip fractures in the ED by location and age of patient
Two questions to guide hip fracture management in the ED:
- Is the fracture intracapsular (femoral neck and proximal) or extracapsular (distal to femoral neck)?
- Is the patient young or old?
Intrascapular fractures: The concern with an intracapsular fracture is compromise of the femoral head bloody supply, increasing the risk of avascular necrosis of the femoral head. In a young patient, an intracapsular fracture is an orthopedic emergency. Time is femoral head. Preserving the native femoral head is a priority, and these patients need OR as soon as possible. Conversely, in an older adult with an intracapsular fracture, preserving the native femoral head is less of a priority and these patients are often treated with hip arthroplasty.
Extracapsular fractures include intertrochanteric and subtrochanteric fractures. They bleed outside the capsule and therefore can bleed more substantially. Subtrochanteric fractures behave more like femoral shaft fractures and are particularly important in anticoagulated elderly patients because of blood loss and transfusion risk. Younger patients with extracapsular fractures should be monitored for compartment syndrome.

Source: https://paulthorntonbott.com/hip-conditions/hip-fracture/
Calling a hip injury consult: what does orthopedics want to know
- Mechanism: low-energy fragility fall vs high-energy trauma.
- Fracture description: femoral neck, intertrochanteric, subtrochanteric, greater trochanter, acetabular/pelvic involvement, displacement and whether x-ray/CT/MRI is pending.
- Baseline function: ambulatory status, independence, cognition and goals of care where relevant.
- Comorbidities and medications, especially anticoagulants/antiplatelets and exact last dose.
- Bloodwork concerns: hemoglobin, renal function, electrolytes, INR and type & screen.
- Analgesia given, whether a block was done, NPO status and delirium-prevention steps already started.
Diagnosing and managing greater trochanter fractures in the ED
Greater trochanter fractures are usually managed non-operatively, weight bearing as tolerated, but apparent isolated greater trochanter fractures may have occult intertrochanteric extension on MRI. If the fracture extends across the midline or the patient has persistent inability to weight bear, the injury may be unstable and require operative fixation.
There is also an important exception in younger active patients: a large displaced greater trochanter fracture may function like an avulsion of the gluteus medius insertion, analogous to a full-thickness rotator cuff tear of the shoulder. Even without major intertrochanteric extension, loss of the abductor mechanism can cause major functional impairment and may warrant operative fixation.
Systematic approach to reading hip and pelvis x-rays in the ED
- On the AP pelvis, force yourself to read systematically – outside to inside or inside to outside – from greater trochanter to pubic symphysis, comparing both sides. Don’t forget to scrutinize the acetabulum.
- Look at the femoral head/neck, intertrochanteric line, lesser and greater trochanters, acetabular roof and columns, pubic rami and sacrum.
- If there is prosthetic hardware, the x-ray must include the tip of the prosthesis. Periprosthetic fractures often occur at the stress riser at the end of the stem. A standard hip series may not show the tip of a long stem; order femur films if needed.
Native hip dislocation: reduce early after life threats
Native hip dislocation is usually secondary to high-energy trauma. Posterior dislocation is most common: shortened, internally rotated and adducted. Anterior dislocation is rare and likely externally rotated and shortened.
- Get an x-ray to confirm direction/pattern unless the patient is crashing and/or the diagnosis is clinically obvious.
- Reduce early: native hip dislocation is an orthopedic emergency. Once life threats are addressed, reduction should not wait for a CT just to map every fragment. Prolonged dislocation threatens femoral head perfusion and sciatic nerve function.
- Do not keep pulling through repeated failed attempts. If it will not reduce with good sedation and technique, stop and call for help.
- CT usually comes after reduction for a posterior dislocation. Fragments are common and not usually a reason to delay reduction. CT before reduction is more compelling when the plain film shows bone clearly blocking the reduction path, the pattern is not understood, or the patient has a complex polytrauma workflow where CT is happening immediately anyway.
- The most common reason for irreducible native hip dislocation is soft-tissue buttonholing through the posterior capsule, requiring open reduction.
Reducing posterior hip dislocations in the ED: tricks and techniques
Our guest experts’ preferred technique for reducing hip dislocations is the Whistler technique. This is a modification of the Captain Morgan technique that requires less brute force and is less dangerous to the clinician than the traditional Allis technique. The Whistler technique is done with the patient lying supine on the stretcher with both knees flexed and feet on the stretcher; assistant stabilizing the pelvis; put your arm under the affected side knee onto the contralateral knee; hold the affected side ankle with your other hand; lift from your knees while adding the appropriate vector; internally rotate the hip.
If a couple of good attempts fail despite adequate sedation and a change in technique, stop and involve orthopedics/anesthesia for reduction in the OR with paralysis.
Pearl: Internal rotation at the hip while performing the Whistler technique puts the knee in valgus and helps the femoral head clear the acetabular rim.
Pitfall: Light sedation for a hip reduction. Hip dislocations involve some of the largest muscles in the body and appropriate sedation, sometimes requiring airway management, is more important than the choice of technique.
Post-reduction care of hip dislocation patients in the ED
- Gently assess stability. If the hip falls back out with gentle flexion/internal rotation/external rotation, that is critical information, especially in an arthroplasty patient who may need revision.
- Reassess and document sciatic nerve function when the patient is awake.
- Obtain post-reduction imaging. Consider CT after reduction for native hip dislocations to assess for acetabular or intra-articular fragments, femoral head injury, and congruity.
- Immobilize appropriately to prevent re-injury. Preventing knee flexion with a knee immobilizer helps prevent hip flexion into the unstable position, reducing the chance of re-dislocation.
Key take home pearls and pitfalls for hip emergencies in the ED
Pearls:
- Surgical repair of hip fractures within 24 hours is ideal to restore mobility. The high morbidity/mortality is driven less by the bone injury itself than by what can follow secondary to immobilization: delirium, pneumonia, venous thromboembolism, pressure injuries, myocardial infarction and deconditioning.
- The hip fracture can occur before the fall or with no fall. In older adults, in particular those with osteoporosis, twisting/jerking movements alone are enough to cause a fracture.
- Symmetric non-painful bilateral active straight leg essentially rules out serious injury from L spine to proximal femur. The iliopsoas originates from the L-spine and inserts on the lesser trochanter and actively stressing this mechanism tests multiple areas at the same time.
- The patellar-pubic percussion test is a highly sensitive and specific physical exam maneuver for hip fracture. In resource limited settings, an abnormal test could support a decision to transfer urgently for more advance imaging.
- Not all atraumatic hip pain is arthritis. Broaden your differential for atraumatic hip pain to include AVN, iliopsoas abscess/ hematoma, septic hip, atypical femur fractures, subchondral insufficiency fractures, and greater trochanteric pain syndrome.
- Young patient + femoral neck fracture = orthopedic emergency. A femoral neck fracture portends risk of bleeding within the joint capsule, putting the femoral head at risk. While older adults with femoral neck fractures typically require a hip arthroplasty, the goal in young patients is to preserve the native hip and this requires getting to the OR as soon as possible.
- Be prepared for blood loss in patients with intertrochanteric and more distal fractures. Especially be cautious in older patients on anticoagulation or DAPT. Younger patients are at risk for compartment syndrome with these fractures; consider avoiding hip blocks that could mask pain in these patients.
- The Whistler technique for reducing posterior hip dislocations is safer for the clinician and requires less force than other methods. However, what matters more than technique choice is a patient who is appropriately sedated which may require a general anaesthetic.
Pitfalls:
- Missing the basics in the ED can delay OR. Clarify last dose of anticoagulation and reverse if necessary, order NPO, prevent delirium by minimizing opioids , perform a hip block early, pre-op labs and ECG.
- Ruling out a hip fracture based on a normal x-ray and CT. If clinical suspicion for fracture is high and x-ray is normal, advanced imaging should be pursued as 2-10% of hip fractures are radiographically occult. Even CT isn’t perfect, and MRI is sometimes needed to pick up non-displaced femoral neck fractures, intertrochanteric extension of greater trochanter fractures, early marrow edema, and subchondral insufficiency fractures (i.e. stress fracture of the older adult hip).
- Missing a pelvic fracture because we aren’t looking for it. Features on exam suggestive of a pelvic fracture: medial groin pain, public symphysis pain, pain with compression of the pelvis. Adopt a systematic approach to reading hip and pelvis x-rays that includes careful interrogation of the acetabulum/ pubic rami.
- Ruling out a periprosthetic fracture with incompletely imaged hardware. Often need to order femur series along with hip images in patients with prosthetic joints to see the distal tip of the prosthesis as this is a common location for periprosthetic fracture.
- Forgetting to test internal rotation at the hip in patients with atraumatic hip pain. Femoroacetabular impingement presents with hip pain and loss of passive internal rotation usually in males in their 30s and 40s. It is analogous to frozen shoulder.
- Not examining the hip in a patient presenting with knee pain. If pain is not reproducible on exam of the knee, look more proximally.
References
- Asher R. The Dangers of Going to Bed. Br Med J. 1947;2(4536):967-968.
- Bolt C, O’Keeffe F, Finnegan P, et al. Straight Leg Elevation to Rule Out Pelvic Injury. Injury. 2018;49(2):279-283.
- Boniface K, Pyle M, Jaleesah N, Shokoohi H. Point-of-Care Ultrasound for the Detection of Hip Effusion and Septic Arthritis in Adult Patients With Hip Pain and Negative Initial Imaging. J Emerg Med. 2020;58(4):627-631.
- British Orthopaedic Association, National Institute for Health and Care Excellence (NICE). Hip Fracture: Management (NG124). Updated 2023.
- Bunker TD, Esler CNA, Leach WJ. Rotator-Cuff Tear of the Hip. J Bone Joint Surg Br. 1997;79(4):618-620.
- de Haan E, Roukema GR, van Rijckevorsel VAJIM, Kuijper TM, de Jong L. Risk Factors for 30-Days Mortality After Proximal Femoral Fracture Surgery, a Cohort Study. Clin Interv Aging. 2024;19:539-549.
- Downey C, Kelly M, Quinlan JF. Changing Trends in the Mortality Rate at 1-Year Post Hip Fracture: A Systematic Review. World J Orthop. 2019;10(3):166-175.
- Goh EL, Khatri A, Costa AB, et al. Prevalence of Complications in Older Adults After Hip Fracture Surgery: A Systematic Review and Meta-Analysis. Bone Joint J. 2025;107-B(2):139-148.
- Guay J, Parker MJ, Griffiths R, Kopp S. Peripheral Nerve Blocks for Hip Fractures. Cochrane Database Syst Rev. 2017;5(5):CD001159.
- Haj-Mirzaian A, Guermazi A, Omoumi P, et al. Imaging of Occult Hip Fractures: CT or MRI? AJR Am J Roentgenol. 2020;214(3):W94-W103.
- HIP ATTACK Investigators. Accelerated Surgery Versus Standard Care in Hip Fracture (HIP ATTACK): An International, Randomised, Controlled Trial. Lancet. 2020;395(10225):698-708.
- Mariconda M, Costa GG, Cerbasi S, et al. The Determinants of Mortality and Morbidity During the Year Following Fracture of the Hip: A Prospective Study. Bone Joint J. 2015;97-B(3):383-390.
- Maruenda JI, Barrios C, Llombart R, et al. Traumatic Hip Joint Tamponade: A Cause of Avascular Necrosis After Femoral Neck Fracture. J Trauma. 1997;42(5):944-946.
- Pincus D, Ravi B, Wasserstein D, et al. Association Between Wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery. JAMA. 2017;318(20):1994-2003.
- Rahman LA, Adie S, Naylor JM, et al. A Systematic Review of the Diagnostic Performance of Orthopedic Physical Examination Tests of the Hip. BMC Musculoskelet Disord. 2013;14:257.
- Rajeev A, Seneviratne S, Radha S, et al. The Patellar-Pubic Percussion Test in Occult Hip Fractures. Injury. 2013;44(12):1862-1865.
- Stahl CC, Funk LM, Schumacher JR, Zarzaur BL, Scarborough JE. The Relative Impact of Specific Postoperative Complications on Older Patients Undergoing Hip Fracture Repair. Jt Comm J Qual Patient Saf. 2021;47(4):210-216.
- Sung A, Kim DH, Kim DH, Jeong JH. Patient and Emergency Department Factors Influencing Surgery Timing in Patients With Hip Fracture. Sci Rep. 2025;15(1):22682.
- Welford P, Jones CS, Davies G, et al. The Association Between Surgical Fixation of Hip Fractures Within 24 Hours and Mortality: A Systematic Review and Meta-Analysis. Bone Joint J. 2021;103-B(7):1176-1186.
- Welch JM, Gomez GI, Chatterjee M, et al. Contextual Determinants of Time to Surgery for Patients With Hip Fracture. JAMA Netw Open. 2023;6(12):e2347834.
- Yamamoto T. Subchondral Insufficiency Fractures of the Femoral Head. Clin Orthop Surg. 2012;4(3):173-180.
Drs. Helman, DiStefano and Sayal have no conflicts of interest to declare.
Now test your knowledge with a quiz.



Leave A Comment