
The management of acute pharyngitis remains one of the most common—and surprisingly controversial—decisions in emergency and primary care. While many clinicians and patients assume that a positive streptococcal test should automatically lead to antibiotic treatment, a deeper dive into the literature on this month’s Journal Jam podcast with Dr. Justin Morgenstern and Dr. Casey Parker reveals substantial uncertainty around the magnitude of benefit, the prevention of complications like peritonsillar abscess and rheumatic fever, and the balance between benefit and harm. This Journal Jam examines the world’s evidence supporting antibiotic treatment for presumed streptococcal pharyngitis and highlights several important evidence-based medicine (EBM) concepts…
Podcast: Play in new window | Download (Duration: 1:19:21 — 72.7MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Anton Helman June, 2026
Cite this podcast as: Morgenstern, J. Parker, C. Helman, A. Journal Jam 24 Antibiotics for Strep Throat: Evidence, Myths and Misperceptions. Emergency Medicine Cases. June, 2026. https://emergencymedicinecases.com/journal-jam-antibiotics-strep-throat-evidence-myths-misperceptions. Accessed August 2, 2026
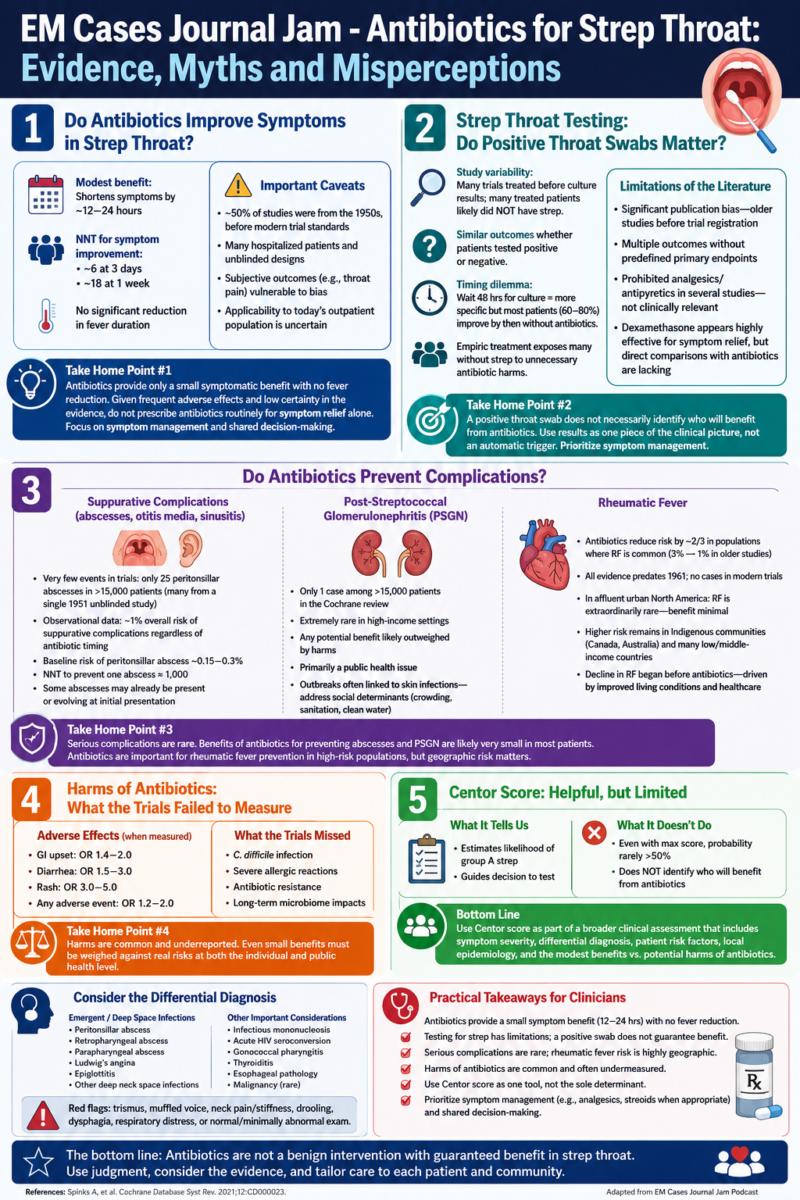
Do Antibiotics Improve Symptoms in Strep Throat?
The strongest evidence synthesis with regards to antibiotics improving symptoms in strep throat comes from the 2021 Cochrane review on the topic, which found that antibiotics modestly improve symptom resolution in acute sore throat. There was no significant reduction in fever duration, but headache and sore throat improved somewhat faster with antibiotics. The estimated number needed to treat (NNT) for symptom improvement at 3 days was approximately 6, increasing to approximately 18 by 1 week. Depending on the analytic approach, antibiotics shortened symptom duration by only roughly 12–24 hours. However, the our experts emphasize that these apparently favorable results require careful interpretation. Approximately half of the studies included in the evidence base were conducted in the 1950s, many before modern standards of randomization, blinding, and trial registration. In several studies, patients were hospitalized for uncomplicated pharyngitis, raising questions about external validity and applicability to contemporary outpatient populations. Subjective outcomes such as throat pain are particularly vulnerable to bias in unblinded trials. Our experts suggest that while a small symptomatic benefit likely exists, the magnitude of that benefit is probably modest and may not outweigh treatment-related harms for most patients.
Take home point #1: While antibiotics for strep throat may shorten symptoms by approximately 12–24 hours, the benefit is modest and based largely on older studies with important methodological limitations. The best available evidence suggests that treating six patients will result in one additional patient feeling better by day 3, but there is no meaningful reduction in fever duration. Given the frequency of antibiotic-related adverse effects and the uncertainty surrounding the quality of the evidence, antibiotics should not be prescribed routinely for symptom relief alone. Instead, clinicians should focus on effective symptom management and engage patients in shared decision-making about the potential benefits and harms of antibiotic therapy.
Strep Throat Testing: Do Positive Throat Swabs Matter?
One of the most striking findings from the literature review on throat swabs for strep throat for the diagnosis of strep throat was the variability in inclusion criteria across trials. Some studies required microbiologic confirmation of group A streptococcal infection, whereas many initiated treatment before culture results were available. Consequently, a substantial proportion of treated patients likely did not have streptococcal pharyngitis. Paradoxically, several studies demonstrated similar outcomes regardless of whether patients ultimately tested positive for streptococcus. This observation raises important questions. Either the studies are affected by bias, particularly given the prevalence of unblinded designs, or antibiotics may be exerting some anti-inflammatory effect independent of bacterial eradication. If symptom improvement results primarily from anti-inflammatory properties, simpler interventions such as ibuprofen may provide similar benefits with fewer harms.
Timing creates an additional clinical dilemma. Waiting 48 hours for culture confirmation increases diagnostic specificity but occurs after most patients have already improved clinically. Across multiple studies, approximately 60–80% of patients were substantially better within 48 hours without antibiotic therapy. Conversely, immediate empiric treatment exposes many patients without streptococcal infection to unnecessary antibiotic-related harms.
Limitations of the Strep Throat Literature: Publication Bias and Other Medications Included or Excluded
In reviewing the strep throat literature we had significant concerns about publication bias. Much of the evidence predates trial registration, raising the possibility that negative studies were never published and that positive findings are overrepresented. Many older trials also reported multiple outcomes without predefined primary endpoints, increasing the risk of selective outcome reporting and exaggerated treatment effects.
Another limitation is that several studies prohibited analgesics and antipyretics. While this may help isolate the effect of antibiotics, it has little clinical relevance because physicians want to know whether antibiotics add benefit beyond standard symptom management with medications such as ibuprofen or acetaminophen. Our experts also noted that dexamethasone appears highly effective for symptom relief, although direct comparisons between corticosteroids and antibiotics for uncomplicated pharyngitis have not been adequately studied.
Take Home Point #2: A positive throat swab for strep does not necessarily identify the patients most likely to benefit from antibiotics. In many studies, outcomes were similar whether patients ultimately tested positive or negative for streptococcus, raising concerns about study bias and the true mechanism of symptom improvement. Waiting for culture confirmation improves diagnostic accuracy but often delays treatment until most patients are already improving, while empiric treatment exposes many patients without strep throat to unnecessary harms. Given the limitations of the evidence, clinicians should focus on symptom management and use throat swab results as just one piece of the overall clinical picture rather than an automatic trigger for antibiotic prescribing.
Harms of Antibiotics for Strep Throat: What the Trials Failed to Measure
Perhaps the most important limitation identified in the literature was the inadequate reporting of harms. Meaningful risk-benefit analysis requires accurate measurement of both benefits and adverse events, yet most studies focused almost exclusively on efficacy outcomes. The few studies that systematically reported adverse events demonstrated measurable harm. One study reported a 15% absolute increase in nausea and vomiting and a 10% increase in diarrhea among antibiotic-treated patients. Another reported adverse events in 21% of antibiotic recipients compared with 5% in the placebo group. A third found that 6% of patients discontinued antibiotics because of side effects. Our experts conclude that if symptom benefit is measured in hours while adverse effects occur in 10–20% of treated patients, the balance may favor withholding routine antibiotics when symptom control is the sole goal.
Does Antibiotic Treatment Prevent Strep Throat Complications like Peritonsillar Abscess, Glomerulonephritis and Rheumatic Fever?
Evidence for Antibiotics Preventing Suppurative Complications of Strep Throat
A major argument for antibiotic therapy is prevention of suppurative complications such as peritonsillar abscess, retropharyngeal abscess, parapharyngeal abscess, sinusitis, and otitis media. The Cochrane review reported an odds ratio of 0.21 for otitis media and 0.16 for peritonsillar abscess, suggesting substantial relative risk reduction. However, closer examination reveals remarkably few events. Across more than 15,000 patients, only 25 peritonsillar abscesses were reported. Sixteen of those events originated from a single unblinded 1951 study involving hospitalized patients. We have to wonder about data accuracy, event adjudication, and generalizability. In one instance, Cochrane reported 15 abscesses in a control group while the original manuscript reportedly documented only 9. An observational study of 14,610 patients with acute pharyngitis found an overall suppurative complication rate of approximately 1%, with similar complication rates among patients receiving immediate antibiotics, delayed antibiotics, or no antibiotics. While observational data cannot establish causality, these findings suggest that complications are relatively uncommon in modern practice.
Using the available data, we estimate a baseline risk of peritonsillar abscess of approximately 0.15–0.3%, implying a rough NNT approaching 1,000 to prevent a single abscess. Many peritonsillar abscesses may not represent late complications of untreated pharyngitis at all. Instead, some may already be evolving at the time of initial presentation, making antibiotics more a treatment of early abscess than prevention of future abscess. The available evidence is insufficient to resolve this question definitively.
Evidence for Antibiotics for Strep Throat preventing Post-Streptococcal Glomerulonephritis
The evidence that antibiotics prevent post-streptococcal glomerulonephritis (PSGN) is remarkably weak. The Cochrane review identified only a single case of glomerulonephritis among more than 15,000 patients, making it impossible to draw meaningful conclusions about treatment effect. PSGN is extremely rare in most high-income settings, and any potential benefit from routine antibiotic treatment is likely outweighed by the harms of exposing large numbers of patients to antibiotics. PSGN should be viewed primarily as a public health issue rather than an individual patient issue. In outbreak settings or high-risk communities, a more liberal antibiotic strategy may be reasonable, particularly because outbreaks are often associated with streptococcal skin and soft tissue infections rather than pharyngitis. Indeed, observational data from Australia suggest that interventions targeting skin infections during outbreaks may help reduce subsequent PSGN cases, highlighting the importance of addressing underlying social determinants such as overcrowding, inadequate sanitation, and limited access to clean water.
Evidence for Antibiotics for Strep Throat preventing Rheumatic Fever: Geography Matters
Unlike PSGN, there is convincing evidence that antibiotics reduce the risk of acute rheumatic fever in populations where rheumatic fever remains common. The Cochrane review found that antibiotics reduced the odds of rheumatic fever by approximately two-thirds, with rates falling from roughly 3% to 1% in the historical studies. However, virtually all of this evidence comes from studies conducted before 1961, and no cases of rheumatic fever were reported in modern trials. The key issue is therefore not whether antibiotics can prevent rheumatic fever, but whether the patient population being treated remains at meaningful risk. In affluent urban populations in North America, rheumatic fever has become extraordinarily rare, with incidence approaching zero. In these settings, routine antibiotic treatment of strep throat is unlikely to provide meaningful protection against rheumatic fever. In contrast, significant geographic variability persists. Rheumatic fever remains a major cause of morbidity in certain Indigenous communities in Canada and Australia, as well as in many low- and middle-income countries. In these higher-risk populations, clinicians may reasonably adopt a much lower threshold for antibiotic treatment. The dramatic decline in rheumatic fever over the last century began long before the introduction of antibiotics and is largely attributable to improvements in housing, sanitation, nutrition, and access to healthcare. Thus, while antibiotics remain an important preventive tool in high-risk populations, the most effective long-term strategy for preventing rheumatic fever is likely to be addressing the socioeconomic conditions that allow streptococcal disease to flourish.
Take Home Point #3: The evidence that antibiotics prevent serious complications of strep throat is far weaker than many clinicians assume. Suppurative complications such as peritonsillar abscess are rare, with a baseline risk likely well under 1%, meaning hundreds to thousands of patients may need treatment to prevent a single abscess. Evidence that antibiotics prevent post-streptococcal glomerulonephritis is extremely limited, and in high-income settings the condition is so uncommon that any potential benefit is unlikely to outweigh antibiotic harms. Rheumatic fever is the exception: antibiotics clearly reduce risk in populations where rheumatic fever remains prevalent. However, because rheumatic fever has become extraordinarily rare in affluent urban populations, the decision to prescribe antibiotics for strep throat should depend heavily on local epidemiology and patient risk factors rather than a one-size-fits-all approach.
Consider the Differential Diagnosis of Sore Throat Presentations
While most patients presenting with sore throat have uncomplicated viral or streptococcal pharyngitis, clinicians should remain vigilant for alternative diagnoses that may require urgent intervention. Important conditions to consider include peritonsillar abscess, retropharyngeal abscess, parapharyngeal abscess, Ludwig’s angina, epiglottitis, and other deep space neck infections, particularly in patients with trismus, muffled voice, neck pain or stiffness, drooling, dysphagia, or respiratory symptoms. Other considerations include infectious mononucleosis, acute HIV seroconversion, gonococcal pharyngitis, thyroiditis, esophageal pathology, and, rarely, malignancy. A sore throat with a normal or minimally abnormal oropharyngeal examination should prompt clinicians to broaden the differential diagnosis and consider potentially life-threatening causes.
How Useful is the Centor Score in Deciding on Antibiotics for Sore Throat?
The Centor score is often used to estimate the probability of group A streptococcal pharyngitis and guide testing decisions, but it has important limitations. Even patients with the maximum Centor score rarely have a pretest probability much above 50%, meaning considerable diagnostic uncertainty remains. One of the key themes of this Journal Jam is that identifying strep does not necessarily identify patients who will benefit from antibiotics. As such, the Centor score may be useful for estimating the likelihood of streptococcal infection, but it should not be used in isolation to determine antibiotic prescribing. Instead, clinicians should integrate Centor criteria into a broader clinical assessment that considers symptom severity, alternative diagnoses, patient risk factors, local epidemiology, and the modest benefits and potential harms of antibiotic therapy.
Strep Throat Management in the ED: An Evidence-Based Approach
For patients with uncomplicated pharyngitis in high income settings, symptom-directed management appears reasonable. This includes:
- Acetaminophen and/or NSAIDs, throat lozenges and/or sprays for pain control
- Consideration of dexamethasone for severe symptoms
- Clear return precautions
- Shared decision-making regarding antibiotic therapy
- Careful assessment for deep space neck infection or other alternative diagnoses
Education may be one of the most valuable interventions clinicians provide. Helping patients understand the modest benefits and potential harms of antibiotics can empower them to make informed decisions and may reduce unnecessary healthcare utilization in the future.
The evidence suggests that antibiotics provide, at most, modest symptomatic benefit in uncomplicated pharyngitis, shortening illness duration by approximately 12–24 hours in some patients. Important limitations include methodological weaknesses, publication bias, inconsistent inclusion criteria, and inadequate reporting of harms. Adverse effects occur commonly and may outweigh symptomatic benefits for many patients. Evidence supporting prevention of suppurative complications is weaker than often assumed because absolute event rates are very low and modern data are limited. A symptom-directed management approach is reasonable for most patients, reserving antibiotics for selected higher-risk patients based on overall clinical assessment and epidemiological risk rather than relying solely on scoring systems or microbiologic testing. Patients with severe symptoms, concern for early deep-space infection, prior peritonsillar abscess, immunocompromise, or other high-risk features may warrant antibiotics.
References
Drs. Helman, Morgenstern and Parker have no conflicts of interest to declare.



Great discussion!
Y’all might be interested to know that in the United States, we have a quality program called MIPS that encourages strep testing prior to antibiotic administration.
https://qpp.cms.gov/docs/QPP_quality_measure_specifications/CQM-Measures/2020_Measure_066_MIPSCQM_v4.1.pdf
Payment is tied to this, and meeting MIPS metrics is heavily encouraged.
Thanks gents – very engaging and interesting. Certainly practice refining for a junior Australian GP Reg – the Australian guidelines prevaricate on both swabbing and giving antibiotics so I found this discussion really illuminating.