

In this ECG Cases blog we look at pitfalls from ECG artifact and lead misplacement, and pearls to prevent misdiagnosis.
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman, August, 2024.
Five patients had ECGs suggesting dangerous pathologies. Which were simply ECG acquisition errors?
Case 1: 95-year-old, history of AF, with shortness of breath. Is this polymorphic VT?

–
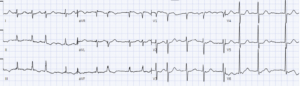
Case 2: 60-year-old with syncope. Is this atrial fibrillation?

–
Case 3: 60-year-old, recent alcohol and crack use, with vomiting. Is this inferior infarct?

–
Case 4: 60-year-old with intermittent chest pain. Is this septal infarct?

–
Case 5: 20-year-old with syncope. Is this Brugada or STEMI?

–
ECG artifact and lead misplacement
Before interpreting an ECG, you need to make sure it has been properly acquired. There are four common types of ECG acquisition error:
- Artifact:
- Pitfall: can mimic tachy-arrhythmias
- Pearl: unaffected lead recorded at the same time, or if there are narrow R waves marching through the noise
- limb lead reversal:
- Pitfall: can mimic infarct or ischemia
- Pearl: consider if there’s abnormal atrial axis (P wave in normal sinus should be upright in I and II, taller in II than in I, and inverted in aVR), abnormal ventricular axis, or if one of the limb leads has a flat line
- high precordial lead
- Pitfall: can mimic septal infarct, Wellens, or Brugada
- Pearl: P wave from sinus rhythm should be biphasic in V1 and upright in V2. Consider high lead placement if P wave is fully inverted V1 or not fully upright in V2, and if aVR/V1/V2 all look similar
- precordial lead reversal
- Pitfall: can mimic infarct
- Pearl: consider if bizarre R wave progression
Back to the cases
Case 1: 95-year-old, history of AF, with shortness of breath. Is this polymorphic VT?
Apparent polymorphic wide complex tachycardia, but lead I is unaffected, and there are narrow R waves marching through the noise. ECG repeated: atrial fibrillation with narrow QRS:
–
Case 2: 60-year-old with syncope. Is this atrial fibrillation?
There appears to be atrial fibrillation but the rhythm is regular, and lead I shows clear P waves without artifact. ECG repeated: normal sinus rhythm.

–
Case 3: 60-year-old, recent alcohol and crack use, with vomiting. Is this inferior infarct?
There’s an apparent left axis deviation from inferior Q waves with T wave inversion, but they are all preceded by inverted P waves. Sinus rhythm should have P wave upright in II and inverted in aVR but this is the opposite. There’s also a T wave inversion in V2 preceded by an inverted P wave. So there’s both limb lead misplacement and high precordial lead placement. ECG repeated with correct placement: normal sinus rhythm (P wave upright in II>I and inverted in aVR, biphasic in V1 and upright in V2) and normal ECG

–
Case 4: 60-year-old with intermittent chest pain. Is this septal infarct?
Apparent Q and T wave inversion in V2. But P wave is fully inverted in V1 and biphasic in V2, and aVR/V1/V2 all look similar. This is high lead placement of V1-2. ECG repeated with lead correction: now P wave is biphasic in 1 and upright in 2, and ECG is normal

–
Case 5: 20-year-old with syncope. Is this Brugada or STEMI?
Apparent saddle-back ST elevation in V2 and ST elevation with large T wave in V1. But the P waves are not fully upright in V2-3, and the R wave progression is bizarre (tall R in V1, then small V2-3 then tall again V3), from precordial lead reversal and high lead placement. ECG repeated: now normal P waves and normal R wave progression, with baseline tall voltages and proportional ST/T

–
Take home points on ECG artifact and lead misplacement
- Artifact: consider if apparent tachy-arrhythmia spares a lead, or if there’s narrow R waves marching through the noise
- Limb lead reversal: consider if abnormal atrial axis, abnormal ventricular axis, or flat line in one of the limb leads
- High precordial lead: consider if P wave is fully inverted in V1 or not fully upright in V2, and if aVR/V1/V2 all look similar
- Precordial lead reversal: consider if R wave progression is bizarre
For more cases and articles from the literature, see ECG Cases 29: misdiagnosis from lead misplacement, artifact and lead reversal
* For interactive, online, and live ECG interpretation courses for medical/paramedic/nursing students, residents, paramedics, cardiac technologists, and emergency physicians, visit heartsECGcourse.com.




The repeat ECG for case 1 and the main ECG for Case 2 are the same and presumably shouldn’t be.
Thanks for catching that Nick! I’ve added the correct repeat ECG for case 1.