
Podcast: Play in new window | Download (Duration: 1:01:07 — 56.0MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary by Anton Helman May, 2026
Cite this podcast as: Helman, A. Herbert, K. Mizon, T. Borgundvaag, B. Episode 218 Substance Use Disorder in the ED – Stigma, Compassion and System Change. Emergency Medicine Cases. May, 2026. https://emergencymedicinecases.com/substance-use-disorder-stigma-compassion-system-change. Accessed August 10, 2026
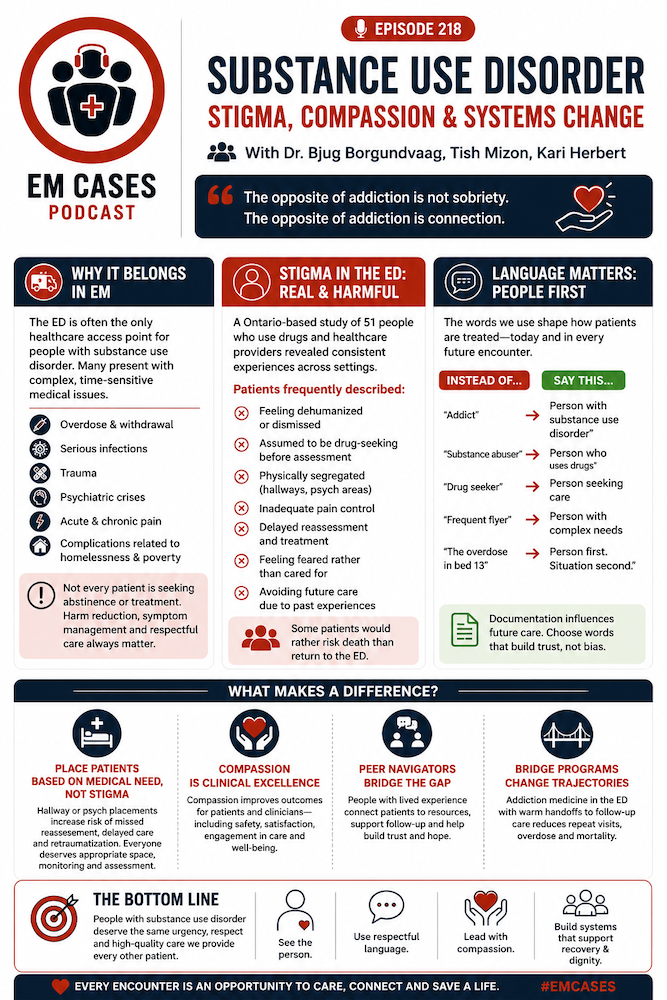
Why Substance Use Disorder Belongs Squarely in Emergency Medicine
Substance use disorder is a chronic medical illness associated with profound morbidity and mortality, and the emergency department is often the only healthcare access point for these patients. Many patients who use drugs do not have consistent access to primary care, addiction medicine, housing supports or mental health resources. The ED therefore becomes the default healthcare system for acute illness, injury, withdrawal, overdose, pain crises and infections.
Patients with substance use disorder commonly present with:
- Overdose
- Withdrawal
- Serious infections including endocarditis and abscesses
- Trauma
- Psychiatric crises
- Acute and chronic pain syndromes
- Complications related to being unhoused and poverty
One of the major themes throughout this episode is that many patients with substance use disorder present with legitimate medical emergencies that risk being missed because clinicians prematurely anchor on intoxication, drug-seeking behavior or psychiatric explanations. Medical emergencies may be missed or minimized because of assumptions surrounding their substance use history. Not every patient with substance use disorder is seeking abstinence or formal treatment. Emergency clinicians should not frame every encounter exclusively through that lens. Harm reduction, symptom management, trust-building and respectful care remain worthwhile interventions even when patients are not ready for recovery-oriented treatment.
Stigma in the ED: What Patients With Substance Use Disorder Experience
A qualitative Ontario-based research study discussed in this episode interviewed 51 people who use drugs across rural, community and academic emergency departments, as well as emergency physicians, nurses and other healthcare providers. The findings were strikingly consistent across settings.
Patients frequently described:
- Feeling dehumanized or dismissed
- Being assumed to be drug-seeking before assessment
- Being physically segregated into hallways or psychiatric areas
- Inadequate pain control
- Delayed reassessment and treatment
- Feeling feared rather than cared for
- Avoiding future healthcare encounters because of prior experiences
Several patients stated they would rather risk death than return to the ED because of prior stigmatizing experiences. One of the most sobering points is that some patients perceive the hospital as more threatening than the illness itself. Patients repeatedly described not feeling believed, particularly when reporting pain. Many perceived that clinicians saw “the substance” before seeing the person. Others described hearing stigmatizing language during EMS handoff or triage conversations, which immediately shaped their expectations for the remainder of the visit.
One important concept is that stigma often begins before the physician enters the room. Language used such as: “Drug seeker”, “Frequent flyer”, “Addict”, “The overdose in bed 13”, “The one from the park” can influence diagnostic reasoning, communication style, analgesic prescribing and disposition decisions long before a proper assessment occurs.
Person-First Language and the Hidden Power of Documentation
Reducing stigma begins with language. Person-first terminology reframes the patient as a human being first rather than defining them solely by a diagnosis or behavior. Instead of: “Addict”, “Substance abuser”, “Drug user” use: “Person with substance use disorder”, “Person who uses drugs”, “Person experiencing homelessness”. Language in the medical record shapes future encounters. Once stigmatizing labels appear in prior notes, subsequent clinicians may enter the room already biased toward mistrust or suspicion. Seemingly small language choices therefore have ripple effects that influence future care, diagnostic reasoning and patient trust. Patients are acutely aware of how staff speak about them, even when conversations occur at a distance or outside the room. The language used during triage, EMS handoff and nursing discussions can immediately signal to patients whether they are entering a safe environment or a hostile one.
Geography Is Destiny: Where Patients Are Placed Matters
Patients with substance use disorder are frequently managed in hallways, waiting rooms or psychiatric holding areas, often reflexively rather than based on clinical need.Where a patient is placed often determines the care they receive. Hallway medicine increases the risk of missed reassessment, delayed recognition of deterioration and inadequate symptom management. Psychiatric holding areas may be retraumatizing for some patients and can subtly communicate that the healthcare team views the patient primarily as a behavioral problem rather than a medical patient. The key principle is that patients with substance use disorder should be placed according to their medical needs, not according to stigma or assumptions. A patient with opioid use disorder and chest pain still deserves appropriate cardiac monitoring and serial assessment. A patient with severe infection or acute pain deserves the same standard of analgesia and reassessment as any other patient.
Compassionate Care Improves Outcomes in Patients With Substance Use Disorder
This episode builds heavily on principles discussed previously in the EM Cases Episdode 145 Compassionate Care with Dr. Barbara Tatham. Compassionate care is not merely a soft skill or optional add-on to technical emergency medicine practice. There is substantial evidence that compassion improves:
- Patient trust
- Treatment adherence
- Symptom control
- PTSD outcomes
- Healthcare utilization
- Follow-up compliance
- Provider wellness and burnout
Importantly, compassionate care may also protect clinicians themselves. Burnout and depersonalization are closely linked, and several studies suggest that meaningful human connection and compassionate practice may actually reduce emotional exhaustion and improve professional fulfillment. Compassionate care does not require lengthy encounters. Brief empathic statements, eye contact, validation and attentive listening can dramatically alter how patients experience their care. Many patients with substance use disorder arrive in the ED expecting hostility; even small gestures of respect and curiosity can therefore become disproportionately meaningful.
Practical Communication Strategies for Building Trust in Patients With Substance Use Disorder
It is important to ask permission before discussing substance use. Rather than launching into interrogation-style questioning, clinicians can ask:
- “Would it be okay if I ask you about substance use?”
- “Can we talk about that for a moment?”
This simple step restores a sense of autonomy and collaboration.
Use open-ended, motivational interviewing–style questions. Asking patients:
- “How are you feeling about your substance use?”
- “What concerns do you have?”
- “What has your experience with healthcare been like?”
- “What happened to you?”
Another important communication principle is validation. Simple statements such as:
- “I believe you.”
- “Thank you for telling me that.”
- “I appreciate you trusting me with that information.”
Patients notice body language, tone, posture and eye contact just as much as the actual words being spoken.
Trauma-informed care is a central communication strategy. Many patients with substance use disorder have extensive histories of trauma, violence, homelessness or prior negative healthcare experiences. Agitation, hostility or distrust may therefore reflect fear and self-protection rather than manipulation or aggression. Reframing the encounter from “What’s wrong with you?” to “What happened to you?” fundamentally changes the tone of care.
Pain Management and the Fear of Undertreatment in Substance Use Disorder
Patients who use fentanyl or other potent opioids often have extraordinarily high opioid tolerance, creating significant challenges around analgesia and withdrawal management. Patients report being consistently undertreated for pain, and clinicians report that they are fearful of prescribing opioids or uncomfortable managing high-tolerance states.
Opioid use disorder does not invalidate pain. Clinicians must distinguish:
- Addiction
- Tolerance
- Dependence
- Acute pain management needs
Undertreated pain contributes directly to mistrust, patient-directed discharge and poor outcomes.
The Bridge Model and the Role of Peer Navigators
The California Bridge model integrates addiction medicine directly into acute care settings through:
- ED-initiated buprenorphine
- Peer navigators
- Harm reduction
- Motivational interviewing
- Rapid outpatient linkage
Bridge programs improve treatment engagement, staff satisfaction, follow-up rates and patient experiences. One of the most powerful aspects of the model is the use of substance use navigators with lived experience who can help patients navigate the enormous logistical barriers surrounding addiction treatment.
These navigators understand the realities of:
- Transportation barriers
- Insurance limitations
- Housing instability
- Rapidly changing addiction treatment systems
- Outpatient follow-up challenges
Patients interviewed in the Ontario study similarly emphasized wanting advocates with lived experience present within emergency departments. Peer navigators were repeatedly identified as one of the most meaningful potential system improvements.
Key Take Home Points for Substance Use Disorder Stigma, Compassion and Systems Change
- Substance use disorder is a chronic medical illness that deserves the same seriousness and urgency as other high-risk chronic diseases seen in emergency medicine. Stigma directly worsens outcomes through delayed diagnosis, mistrust, inadequate analgesia and avoidance of future healthcare encounters.
- Compassionate care is not time-consuming, and even brief empathic interventions can improve trust, adherence and outcomes. Person-first language matters, both at the bedside and within chart documentation. Asking “What happened to you?” instead of “What’s wrong with you?” reframes the encounter in a trauma-informed way that can fundamentally change communication and trust.
- Patients with substance use disorder deserve appropriate analgesia, reassessment and medical care based on their presenting complaint rather than assumptions surrounding substance use. Bridge-style models and peer navigators represent promising systems-level approaches that improve outcomes for patients and clinicians alike.
Compassionate care for patients with substance use disorder is not separate from good emergency medicine — it is good emergency medicine.
References
- Koh JJ, Klaiman M, Miles I, Punja Z, Smith PM, Dong K, Borgundvaag B, et al. Emergency department management of people with opioid use disorder: a national survey of Canadian emergency physicians. Can J Emerg Med. 2020;22(5):694-703.
- Borgundvaag B, Kestler A, Campbell S, et al. Substance use disorders and the emergency department: evidence-informed approaches to care and systems integration. Acad Emerg Med. 2024;31(9):1043-1051.
- Stewart M. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423-1433.
- Fogarty LA, Curbow BA, Wingard JR, McDonnell K, Somerfield MR. Can 40 seconds of compassion reduce patient anxiety? J Clin Oncol. 1999;17(1):371-379.
- Moss J, Roberts MB, Shea L, et al. Healthcare provider compassion is associated with lower PTSD symptoms among patients with life-threatening medical emergencies: a prospective cohort study. Intensive Care Med. 2019;45(6):815-822.
- Pereira L, Figueiredo-Braga M, Carvalho IP. Preoperative anxiety in ambulatory surgery: the impact of an empathic patient-centered approach on psychological and clinical outcomes. Patient Educ Couns. 2016;99(5):733-738.
- Roter DL, Hall JA, Merisca R, Nordstrom B, Cretin D, Svarstad B. Effectiveness of interventions to improve patient compliance: a meta-analysis. Med Care. 1998;36(8):1138-1161.
- Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
- Jeffrey D. Empathy, sympathy and compassion in healthcare: is there a problem? Is there a difference? Does it matter? J R Soc Med. 2016;109(12):446-452.
- Redelmeier DA, Molin JP, Tibshirani RJ. A randomised trial of compassionate care for the homeless in an emergency department. Lancet. 1995;345(8958):1131-1134.
- Marvel MK, Epstein RM, Flowers K, Beckman HB. Soliciting the patient’s agenda: have we improved? JAMA. 1999;281(3):283-287.
- Herring AA, Schultz CW, Yang E, Greenwald MK. Rapid induction onto sublingual buprenorphine after opioid overdose and successful linkage to treatment for opioid use disorder. Am J Emerg Med. 2019;37(12):2259-2262.
- D’Onofrio G, O’Connor PG, Pantalon MV, et al. Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. JAMA. 2015;313(16):1636-1644.
- Kilaru AS, Xiong A, Lowenstein M, et al. Incidence of treatment for opioid use disorder following nonfatal overdose in commercially insured patients. JAMA Netw Open. 2020;3(5):e205852.
- Canadian Centre on Substance Use and Addiction. Toxic Drug Crisis in Canada. Ottawa, ON: CCSA; 2023.
- Substance Abuse and Mental Health Services Administration (SAMHSA). TIP 63: Medications for Opioid Use Disorder. Rockville, MD: SAMHSA; 2021.



I’m grateful for this podcast and as usual it was informative and helpful for regular practise. However, I felt it was unbalanced. One guest could only think of 1 patient who was treated well. This episode to be honest was a disservice to the many, many interactions that ER nurses and doctors undertake with compassion, expertise and frankly, mercy. The guests were pretty negative overall of ER doctors and nurses as we try to help people to the best of our ability, often with lacking resources. This is one of the challenges of guests with a focused interest but without a balanced view of the volume and diversity of clinical problems we face. Also, there was little or no recognition of the behavioural challenges that ER nurses and doctors face, and that we try to put it aside and give people time and what resources we have. What was missing is the good work we do.
Thank you for this thoughtful comment. I agree it’s important to recognize the enormous amount of compassionate, skilled, and often difficult care that ED nurses and physicians provide every day for patients with substance use disorder, usually in very challenging circumstances with limited resources and significant behavioural and safety pressures.
I also think it’s important to clarify that the guests were largely discussing findings from patient and physician perspectives in the research literature and implementation work — findings showing that many patients with substance use disorder still experience stigma and barriers to care in healthcare systems. Those findings are fairly consistent across studies and difficult to dismiss outright.
I don’t think the episode was intended as criticism of emergency clinicians as uncaring people. Rather, it was an exploration of how systems, language, workflows, and culture can unintentionally affect care, even among well-intentioned clinicians working incredibly hard under pressure.
Both things can be true at once: emergency clinicians are doing excellent compassionate work, and there is still room for improvement in how healthcare systems care for patients with substance use disorder.
I appreciate you raising the point because balanced discussion is important.