
Cardiac arrest care hasn’t changed as much as we might think—but how we think about it has. Once CPR and defibrillation are optimized—the two interventions that matter most—we’re often left in the messy middle, where the guidelines are less clear and the decisions feel less certain. It’s here that we start reaching for adjuncts, tweaking airway strategies, and thinking about post-ROSC care—sometimes without a clear sense of what actually improves outcomes versus what just makes us feel like we’re doing something.
In this Part 2 or our 2-part EM Cases podcast series on Cardiac Arrest Update, Dr. Sheldon Cheskes and Dr. Rob Simard take us beyond the algorithms and into the real-world decision-making of cardiac arrest care. We answer questions like: Do vasopressin and steroids improve survival or just ROSC? Should we be giving amiodarone earlier—and is lidocaine just as good? When should we use calcium, bicarbonate, or magnesium, and when should we avoid them? What role does ketamine play in CPR-induced consciousness? How should we choose between supraglottic airways and endotracheal intubation? What are the pitfalls of waveform capnography (ETCO2) to help guide CPR quality, detect ROSC, and inform prognosis? What is the role of PoCUS and TEE during cardiac arrest? When should we terminate resuscitation—and how do ETCO2 and POCUS factor into that decision? Should we widen the criteria to consider thrombolytics and who should go to the cath lab, and should we be ordering whole-body CT after ROSC for everyone who isn’t going to the cath lab or getting ECMO? And finally, what are the key post-ROSC targets that actually impact neurologic outcomes in cardiac arrest patients? and many more…
Podcast: Play in new window | Download (Duration: 1:41:55 — 93.4MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Erik Krosby
Written Summary and blog post by Sara Brade, edited by Anton Helman April, 2026
Cite this podcast as: Helman, A. Simard, R. Cheskes, S.Ep 216 Cardiac Arrest Update: Beyond the 2025 ACLS Guidelines Part 2 – Medications, Airway, Termination and Post-ROSC Care. April, 2026. https://emergencymedicinecases.com/cardiac-arrest-update-part-2/. Accessed August 9, 2026
Cardiac arrest medications beyond epinephrine: Vasopressin and steroids
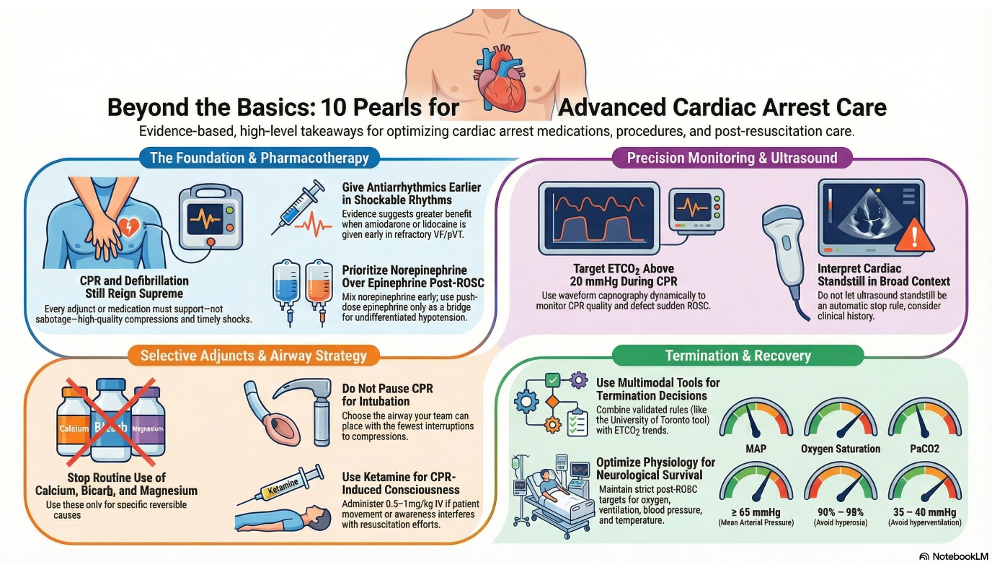
Once CPR quality and defibrillation strategy are optimized, adjunctive medications should be used selectively.
- There is some limited evidence that suggests bundled administration of vasopressin, steroids, and epinephrine in cardiac arrest may improve survival to hospital discharge, but more research is needed to support routine administration. Our experts advise against routine administration of vasopressin and steroids.
- Steroids may still be reasonable after ROSC for narrow indications such as known adrenal insufficiency, septic shock physiology, or refractory vasoplegia.
Post-ROSC vasopressors: Norepinephrine is the go-to pressor
- Norepinephrine is the practical first-line vasopressor for most post-ROSC undifferentiated hypotension.
- Prepare norepinephrine early, even as soon as EMS calls ahead, so it is ready before ROSC is achieved.
- Use push-dose epinephrine as a bridge post-ROSC if there is a delay to starting norepinephrine infusion.
Pitfall: Delay in starting the norepinephrine infusion. If a patient rearrests while the team is still mixing a vasopressor, the opportunity to maintain ROSC may be lost.
Amiodarone vs lidocaine in refractory VF and pulseless VT
The guideline-level message remains that amiodarone and lidocaine are acceptable antiarrhythmics for shock-refractory VF/pVT. AHA Guidelines recommend giving first dose of an antiarrhythmic after the third shock; however, evidence suggests greatest benefit when given as early as possible in refractory shockable arrest. If administering amiodarone, prioritize intravenous administration as intraosseous administration may blunt efficacy. Lidocaine is an effective alternative to amiodarone, although it is used less commonly. Lidocaine is formulated in pre-filled syringes which may be advantageous for remote or low-resource environments.
The ALPS trial (2016) showed no overall survival benefit of amiodarone or lidocaine, but a 2022 re-analysis found that earlier amiodarone administration was associated with improved ROSC and neurologic outcomes.
Pitfall: The earlier antiarrhythmics like amiodarone or lidocaine in cardiac arrest, the better the outcomes. A common pitfall is waiting several rounds of CPR before starting antiarrhythmic medications.
Calcium, sodium bicarbonate, and magnesium in cardiac arrest: Use only for specific indications
Routine calcium, bicarbonate, and magnesium administration are not recommended in cardiac arrest.
Calcium should be reserved for suspected
- Severe hyperkalemia,
- Hypocalcemia, or
- Calcium channel blocker toxicity.
Despite widespread use, evidence supporting calcium in hyperkalemia is weak, with a 2025 systematic review showing no proven clinical benefit and the COCA trial (2021) suggesting possible harm when used routinely in arrest. Despite weak evidence, the experts still favour calcium when the clinical picture points to hyperkalemia due to clinical experience.
Sodium bicarbonate should not be given simply because an arrest is prolonged, and the patient is presumed to be acidotic; bicarb worsens intracellular acidosis and does not improve outcomes. Consider it for sodium channel blocker toxicity such as TCA or cocaine overdose, salicylate toxicity, or hyperkalemia in the setting of DKA.
Magnesium is indicated for Torsades de Pointes, marked QTc prolongation prior to arrest, or cardiac arrest secondary to a QTc prolonging medication overdose. If cardiac arrest occurs during a magnesium infusion (i.e., for eclampsia/pre-eclampsia), immediately stop the infusion and administer calcium to reverse potential magnesium toxicity.
Ketamine for CPR-induced consciousness
- Studies suggest a high rate of patient awareness during CPR; ketamine administration has been suggested as a tool to prevent and manage CPR-induced consciousness.
- While there are no randomized controlled trials demonstrating improved survival or neurologic outcomes with ketamine during cardiac arrest, observational data and evolving protocols support its use for sedation in CPR-induced consciousness (CPRIC), with ketamine favoured for its relative hemodynamic stability compared to other agents. Its proposed neuroprotective effects via NMDA antagonism remain theoretical and unproven, with ongoing trials investigating this role; current expert opinion supports selective use only when CPRIC interferes with resuscitation, not as a routine intervention.
- When patient movement or awareness during CPR/after defibrillation/post-ROSC interferes with effective resuscitation or airway management, consider giving ketamine 0.5-1mg/kg IV.
- Consider giving ketamine only after the high-priority tasks of resuscitation are completed.
Airway management in cardiac arrest: BVM vs SGA vs endotracheal tube
- Airway choice matters less in most cases than minimizing interruptions, avoiding hyperventilation, and matching the airway strategy to operator skill.
- In prehospital systems without frequent intubation exposure, a supraglottic airway is often the best choice.
- In the ED, endotracheal intubation remains the preferred advanced airway when an experienced operator is available, but CPR should not be paused for intubation.
- If EMS arrives with a functioning supraglottic airway and ventilation is adequate, it is often reasonable to keep it in place during the arrest and exchange it after ROSC.
Pitfall: Airway management interrupting high-quality CPR.
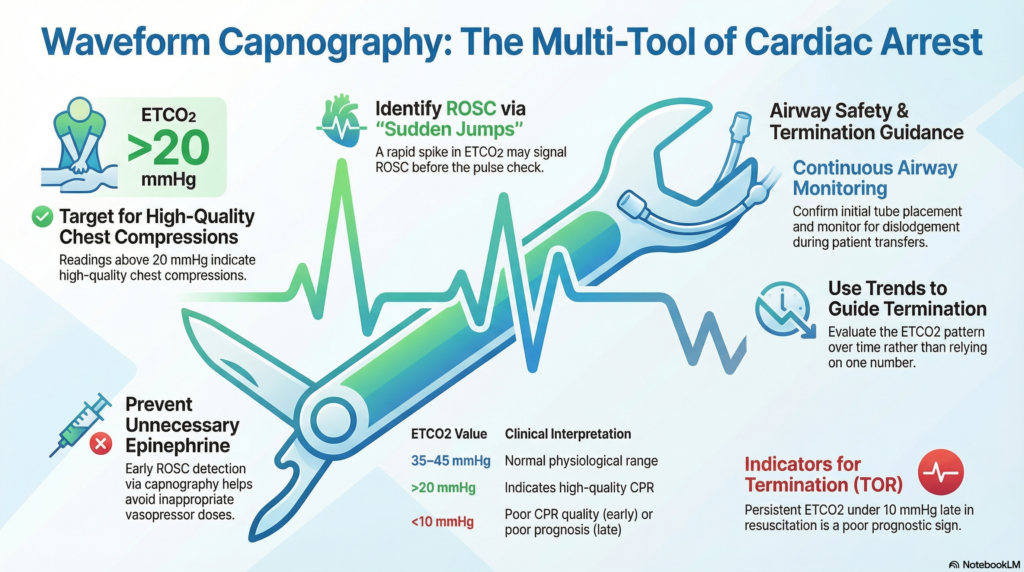
Using ETCO2 waveform capnography in cardiac arrest to guide CPR, detect ROSC and predict outcomes
Waveform capnography can be used to:
- Confirm tube placement,
- Detect tube dislodgement,
- Monitor CPR quality,
- Monitor for ROSC, and
- Supports termination decisions when interpreted over time.
Normal ETCO2 is around 35-45 mmHg. ETCO2 above 20mmHg indicates high-quality CPR. Early in cardiac arrest, a low ETCO2 indicates poor CPR quality. An ETCO2 persistently under 10 despite ongoing high-quality CPR is a poor prognostic sign, especially later in the arrest. A sudden jump in ETCO2 may signal ROSC before the next pulse check and can prevent an unnecessary dose of epinephrine. Loss of a previously present waveform, particularly after transfer, should prompt immediate concern for tube displacement.
Optimizing PoCUS and TEE in cardiac arrest
- Transesophageal Echo (TEE) offers continuous and high-quality imaging during compressions, allows optimization of hand position, and may improve detection of reversible causes such as tamponade, massive PE, aortic dissection, etc. RCT data, however, is lacking.
- The limitation is operational: cost, cleaning, training, simulator access, and team readiness mean TEE is currently a high-value adjunct in select centres rather than a routine ED capability.
- Standard PoCUS still plays a major role, especially in PEA, where the goal is to distinguish true PEA from pseudo-PEA and to look for immediately reversible causes.
- PoCUS should support clinical reasoning while not interrupting compressions.
TEE in Cardiac Arrest EM Quick Hit
PEA Arrest and PoCUS with Rob Simard
Termination of resuscitation : University of Toronto tool, ETCO2, and cardiac standstill
- AHA suggests Termination of Resuscitation (TOR) decision-making should be structured and multi-modal:
- Eligibility check: arrest not causes by hypothermia/toxins/asphyxial asthma/PE/tamponade/other potentially reversible causes; not an ECPR candidate in an ECPR-capable pathway.
- Rule-based support: locally validated TOR rule (adult OHCA) rather than gestalt alone (i.e., University of Toronto tool).
- Physiology: ETCO2 pattern (and if present, arterial line diastolic pressure trend), not a single number.
- Cardiac mechanics: POCUS as an adjunct—especially persistent standstill over time—but with strict compression pause minimization.
- Systems/ethics: documented goals of care when available; team-based model.
- University of Toronto termination of resuscitation tool for out-of-hospital cardiac arrest is used mainly to guide patch physicians when EMS crews are considering TOR in the field:
- No EMS-witnessed arrest,
- No bystander CPR, no shocks,
- No ROSC, and
- No reversible cause identified all push strongly toward termination in the right context.
- End-tidal CO2 trends help refine the decision, and the clinical story still matters – especially patient age, arrest circumstances, and whether the rhythm or downtime fits a potentially salvageable scenario.
- True cardiac standstill on ultrasound is a strong negative prognostic sign, but inter-rater reliability is poor as minimal cardiac movement/flickers are often mistakenly interpreted as standstill. If cardiac standstill is suspected, integrate this finding into the broader clinical context to guide TOR decisions.
Intra-arrest thrombolytics and cath lab activation post-ROSC
- Thrombolytics have no role as routine arrest therapy. AHA guidelines recommend intra-arrest lytics for PE only if PE is confirmed on CT pulmonary angiogram, and only for STEMI (not NSTEMI). Our experts feel that the indications for lytics intra-arrest could be widened on a case-by-case basis to include those with a convincing history for MI or PE with objective ECG evidence of occlusion MI or objective PoCUS findings consistent with PE, although this is not supported by RCTs. If used, they should be given early, rather than as a last resort.
- It is recommended to continue CPR for at least 1 hour post-lytics.
- Emergent indications for peri-arrest PCI include:
- STEMI,
- Cardiogenic shock,
- Recurrent ventricular arrhythmias.
Post-ROSC care: oxygen, ventilation, MAP, temperature, and whole-body CT
It is increasingly recognized that meticulous post-ROSC care is critical for giving the patient the best chance at neurologically intact survival. The immediate post-ROSC phase is one of the highest-risk periods for re-arrest. Hemodynamic instability is common, and rapid intervention is required.
The priorities include:
- Stabilizing blood pressure, typically with norepinephrine
- Identifying and treating reversible causes
- Avoiding hypotension and hypoxia
Targeted Temperature Management
Prevent fever in all post-arrest patients, and consider a target temperature of 32-34 degrees Celsius in the sickest patients based on local protocol and ICU capability.
Pan-CT Post-ROSC
There is increasing interest in the use of early whole-body CT scanning in post-ROSC patients who are not immediately directed to the cath lab or ECMO. This approach aims to identify occult causes such as pulmonary embolism, aortic dissection, or intracranial pathology. Studies suggest that pan-CT has a higher diagnostic yield than gestalt alone and is recommended in the AHA Guidelines. In patients with ROSC and no clear cause of arrest, observational studies and the CT FIRST trial (2023) show that early head-to-pelvis CT increases diagnostic yield and shortens time to diagnosis, but does not improve survival or neurologic outcomes. While not yet standard practice, it reflects a shift toward early, comprehensive diagnostic evaluation in undifferentiated cardiac arrest. The decision to pursue pan-CT must be balanced against the patient’s stability and the resources available, but it represents an evolving area of post-arrest care.
Post-ROSC targets
| Oxygen saturation | 90-98% (avoid hyperoxia) |
| PaO2 | 60-105 mmHg |
| PaCO2 | 35-40 mmHg (avoid hyperventilation) |
| MAP | ≥65 mmHg |
| Temperature | Avoid fever (consider cooling) |
References
- American Heart Association. 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152(16_suppl_2).
- Branch KRH, Gatewood MO, Kudenchuk PJ, et al. Diagnostic Yield, Safety, and Outcomes of Head-to-Pelvis Sudden Death CT Imaging in Post Arrest Care: The CT FIRST Cohort Study. Resuscitation. 2023;188:109785.
- Branch KRH, Strote J, Gunn M, et al. Early Head-to-Pelvis Computed Tomography in Out-of-Hospital Circulatory Arrest Without Obvious Etiology. Acad Emerg Med. 2021;28(4):394-403.
- Cao D, Arens AM, Chow SL, et al. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025.
- Chelly J, Mongardon N, Dumas F, et al. Benefit of an Early and Systematic Imaging Procedure After Cardiac Arrest: Insights From the PROCAT Registry. Resuscitation. 2012;83(12):1444-1450.
- Geldermann N, Dzimiera J, Fischer H, Christ M. Acute Hyperkalaemia in Emergency Care: Evidence-Based Approaches. Emerg Med J. 2026.
- Hirsch KG, Amorim E, Coppler PJ, et al. Part 11: Post–Cardiac Arrest Care: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152(16_suppl_2):S673-S718.
- Jessen MK, Andersen LW, Djakow J, et al. Pharmacological Interventions for the Acute Treatment of Hyperkalaemia: A Systematic Review and Meta-Analysis. Resuscitation. 2025.
- Kudenchuk PJ, Brown SP, Daya M, et al. Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Cardiac Arrest. N Engl J Med. 2016;374:1711-1722.
- Rahimi M, Dorian P, Cheskes S, et al. Effect of Time to Treatment With Antiarrhythmic Drugs on Return of Spontaneous Circulation in Shock-Refractory Out-of-Hospital Cardiac Arrest. J Am Heart Assoc. 2022;11:e023958.
- Vallentin MF, Granfeldt A, Meilandt C, et al. Effect of Intravenous or Intraosseous Calcium vs Saline on Return of Spontaneous Circulation in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2021;326(22):2268-2276.
- Yamanoglu NG, Yamanoglu A. The Effect of Calcium Gluconate in the Treatment of Hyperkalemia. Turk J Emerg Med. 2022;22(2):75-82.
Dr. Cheskes is on the speakers’ bureau of Zoll, received a Zoll Medical Honorarium for CPR Quality and Ventilation during Cardiac Arrest, and received grant funding for studies from Laerdal and Zoll. Drs. Helman and Simard have no conflicts of interest to declare.
Now test your knowledge with a quiz.



Hi,
I cannot find the recommandation for intra arrest lytics in case of STEMI in the 2025 guidelines. Can you find the actual text that says this?