
Facial trauma is everywhere in Emergency Medicine—from assaults and sports injuries to motor vehicle collisions and devastating polytrauma. While many facial injuries are not immediately life-threatening, the misses can be significant: a threatened airway you did not anticipate, a retrobulbar hematoma you did not recognize, or a nasal septal hematoma that progresses to cartilage necrosis. Even a patient who is unnecessarily transferred—or not transferred when they should be. Which facial fracture is most likely to cause delayed airway obstruction, and what simple bedside maneuver can be lifesaving? Why does the physical examination often matter more than the CT scan in determining disposition for facial trauma? How can thinking in facial complexes instead of memorizing Le Fort fractures improve your assessment and communication with facial trauma surgeons? Which seemingly straightforward facial lacerations hide injuries to the facial nerve, parotid duct, canaliculus, or levator muscle? Which fractures require urgent specialist involvement and which can safely go home? What physical examination findings should trigger imaging, consultation, or transfer? In this episode of EM Cases, Anton is joined by Dr. Jeff Fialkov, plastic surgeon and educator at Sunnybrook Health Sciences Centre in Toronto, and Dr. Andrew Petrosoniak, Trauma Team Leader and Emergency Physician at St. Michael’s Hospital, for a practical, top-down approach to facial trauma focused on airway, bleeding, vision-threatening injuries, fracture assessment, soft tissue injuries, and disposition.
Podcast: Play in new window | Download (Duration: 1:43:20 — 94.7MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Anton Helman
Written Summary and blog post by Anton Helman June, 2026
Cite this podcast as: Helman, A. Petrosoniak, A. Fialkov, J. Episode 220 Facial Injuries: Assessment, Management and Disposition. Emergency Medicine Cases. June, 2026. https://emergencymedicinecases.com/facial-injuries-assessment-management-disposition. Accessed August 10, 2026
Facial Injuries Part 1: Airway, Facial Hemorrhage and General Approach
Facial Trauma in the ED: Don’t Let the Face Distract You From What Matters
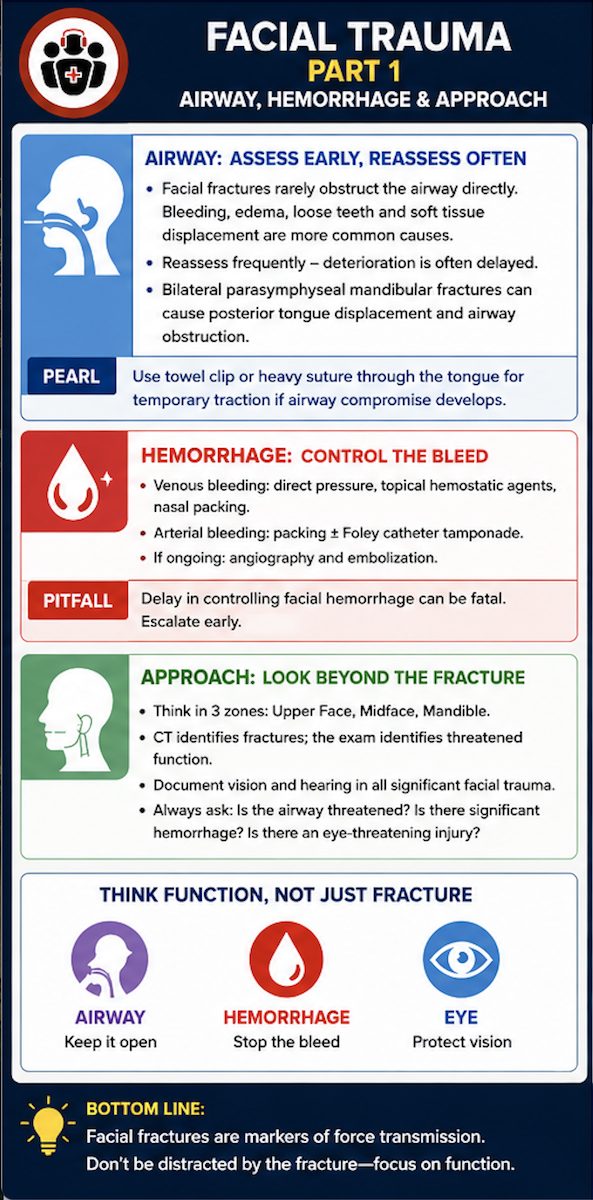
While facial injuries are often visually dramatic, the most important management decisions are frequently unrelated to the fracture pattern itself. Swelling, bruising, bleeding, and deformity naturally draw attention to the face, yet the Emergency Physician’s primary responsibility is identifying injuries that threaten airway patency, vision and neurologic function. Facial fractures should be viewed primarily as markers of force transmission rather than isolated injuries. The same force that fractures the facial skeleton may also injure the brain, cervical spine, globe, optic nerve, carotid arteries, or airway. Consequently, facial trauma should always be approached systematically, beginning with airway, breathing, circulation, and associated injuries before focusing on the facial bones themselves.
A common pitfall is assuming that the severity of visible injury reflects the severity of underlying pathology. Some patients look terrible but have relatively minor injuries, while others have surprisingly subtle external findings despite harboring vision-threatening orbital injuries, unstable midface fractures, blunt cerebrovascular injuries, or intracranial trauma.
When evaluating facial trauma, three questions should be answered:
- Is the airway threatened or anticipated to be threatened?
- Is there significant hemorrhage?
- Is there an eye-threatening injury?
Airway and Hemorrhage: The Facial Trauma Emergencies
The most time-sensitive complications of facial trauma are airway compromise and uncontrolled hemorrhage. Contrary to common teaching, facial fractures themselves rarely obstruct the airway directly. More commonly, airway compromise results from bleeding, loose teeth, bone fragments, displaced soft tissues, expanding edema, or associated laryngeal injury. One of the most important concepts in facial trauma is that airway deterioration is often delayed. Patients speaking comfortably on arrival may develop progressive obstruction over the next several hours as swelling and bleeding worsen. Reassessment is therefore critical throughout the ED stay. Search for loose teeth, dental fragments, and foreign material that may become airway hazards. Midface fractures deserve particular vigilance because posterior displacement of facial structures can alter upper airway anatomy and complicate subsequent airway management.
For deep dive into the Trauma Airway and Airway Trauma: Episode 199 Airway Trauma and Trauma Airway
Bilateral Parasymphyseal Mandibular Fractures and Airway Obstruction
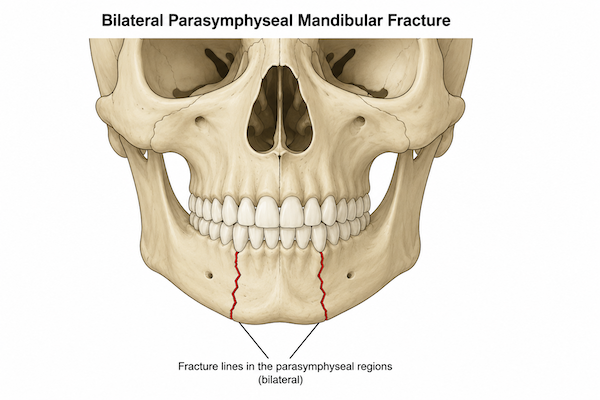
Bilateral parsymphyseal mandibular fractures are a classic cause of tongue airway obstruction
The facial fracture most classically associated with airway obstruction is the bilateral parasymphyseal mandibular fracture. These injuries disrupt anterior support of the floor of mouth, allowing posterior displacement of the tongue and potential airway obstruction, particularly after sedation or paralysis. If posterior tongue displacement is contributing to airway compromise, temporary tongue traction can be lifesaving. Placement of a heavy suture or towel clip through the anterior tongue allows the tongue to be pulled forward and secured externally while preparations are made for definitive airway management.
Clinical Pearl The bilateral parasymphyseal mandibular fracture is the classic facial fracture associated with airway obstruction. If posterior tongue displacement is present, temporary tongue traction with a towel clip or suture through the tongue may prevent complete airway collapse.
Massive Facial Hemorrhage in Facial Trauma
Life-threatening facial hemorrhage is uncommon but can be challenging to control. Severe bleeding is most often associated with high-energy midface trauma involving branches of the internal maxillary artery (see image below). Initial management focuses on rapid control of bleeding while simultaneously addressing airway and hemodynamic status.
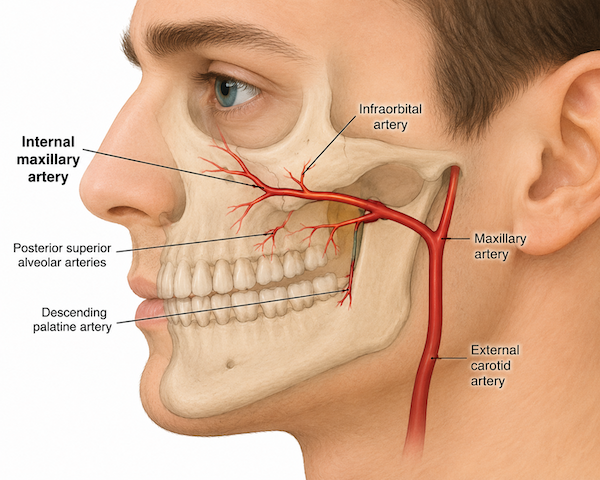
Internal maxillary artery is often the source of difficult-to-control bleeding in facial trauma
Emergency Management of Massive Facial Hemorrhage
- Airway protection
- Blood product resuscitation
- Direct pressure
- Aggressive anterior and posterior packing
- Tranexamic acid when appropriate
- Foley catheter tamponade of deep wound tracts
- Reduction of displaced maxillary fracture
Patients with persistent hemorrhage despite packing and resuscitation may require angiography and embolization, which has largely replaced surgical ligation for inaccessible facial bleeding vessels.
An underappreciated maneuver is reduction of a displaced maxillary fracture. Restoring normal fracture alignment may compress bleeding vessels and provide hemostasis in the same way that reduction of long-bone fractures reduces hemorrhage elsewhere in the body.
Pearl: For facial bleeding after midface fracture that is difficult to control, consider reduction of the displaced maxillary fracture to provide hemostasis.
The Physical Examination for Facial Trauma Matters More Than the CT Scan
CT scanning identifies fractures with remarkable accuracy, but fractures rarely determine urgency. Function does. Many of the findings that alter management are entirely clinical. Visual acuity, ocular motility, hearing, facial nerve function, mandible malocclusion, and sensory deficits cannot be assessed by CT. These findings often determine whether a patient requires urgent intervention, specialist consultation, transfer, or safe outpatient follow-up. Every patient with significant facial trauma should undergo a systematic examination.
Facial trauma assessment should include:
| Structure | Key Exam Findings |
|---|---|
| Eye | Visual acuity, pupils, EOMs, globe position |
| Nose | Septal hematoma, CSF leak |
| Midface | Telecanthus, tenderness, instability |
| Mandible | Occlusion, trismus, lower lip sensation |
| Ears | Hearing, canal injury, hemotympanum |
| Soft tissue | Facial nerve function, parotid duct injury |
Patients frequently provide the most important diagnostic clues. One of the highest-yield historical findings is subjective malocclusion. When a patient reports that their bite feels different that complaint should be taken seriously. Similarly, hearing assessment is commonly overlooked despite the fact that hearing loss, hemotympanum, and external auditory canal injuries may accompany facial fractures.
Key physical exam findings to screen for:
| Examination Finding | Why It Matters |
|---|---|
| Visual acuity deficit | Potential globe injury or optic nerve compromise |
| Diplopia | Orbital injury, entrapment |
| Restricted extraocular movement | Possible entrapment |
| Malocclusion | Mandibular or midface fracture |
| Septal hematoma | Time-sensitive intervention required |
| Lower lip numbness | Inferior alveolar nerve injury |
| Midface instability | Urgent consultation required |
| Facial asymmetry | Displaced fracture |
=> CT identifies fractures. The physical examination identifies threatened function.
A Practical Approach to Facial Fractures: Thinking in Facial Complexes
Emergency physicians are traditionally taught the Le Fort classification system, yet facial trauma surgeons often conceptualize injuries differently. Rather than memorizing Le Fort patterns, it is more useful to think about facial trauma in terms of three major facial complexes because this framework better predicts threatened structures, functional consequences, and operative requirements.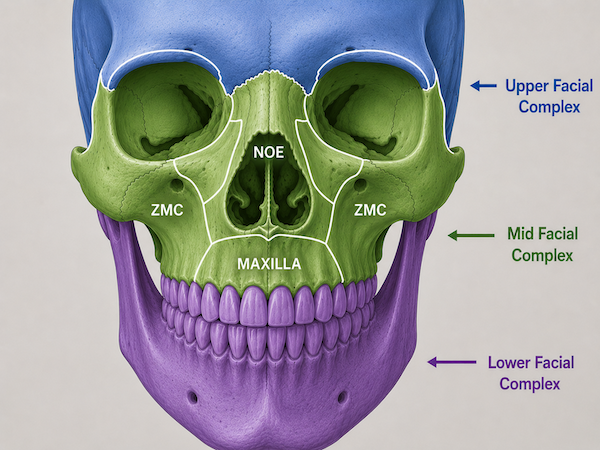
Upper Facial Complex
- Frontal bone
- Frontal sinus
- Superior orbital rims
Fractures in this region generally require high-energy trauma and are important primarily because of their association with intracranial injury, cervical spine injury, and CSF leak.
Midfacial Complex
- Orbits
- Zygomas
- Maxilla
- Naso-orbito-ethmoid (NOE) complex
This region supports vision, globe position, airway structure, facial width, and facial projection. Most clinically significant facial fractures occur here.
Lower Facial Complex
- Mandible
- Dentoalveolar structures
Major concerns include airway compromise, mastication, malocclusion, and inferior alveolar nerve injury.
Thinking in facial complexes also makes Le Fort fractures easier to understand. The facial skeleton is organized around several structural complexes attached to the skull base along natural areas of weakness corresponding to craniofacial suture lines. High-energy trauma propagates along these stress risers, allowing facial complexes to separate from the skull base. A Le Fort I fracture represents separation of the maxillary complex. A Le Fort II fracture involves separation of the maxillary and NOE complexes. A Le Fort III fracture, often referred to as craniofacial dissociation, occurs when the maxillary, NOE, and zygomaticomaxillary complexes become detached from the skull base.
Clinical Pearl: Think of the upper face as protecting the brain and frontal sinus, the midface as protecting vision and facial support, and the mandible as protecting airway and occlusion. This approach more closely reflects how facial trauma surgeons evaluate injuries in practice.
Frontal Sinus Fractures: Posterior Table and Sinus Floor Injuries Require Urgent Consultation
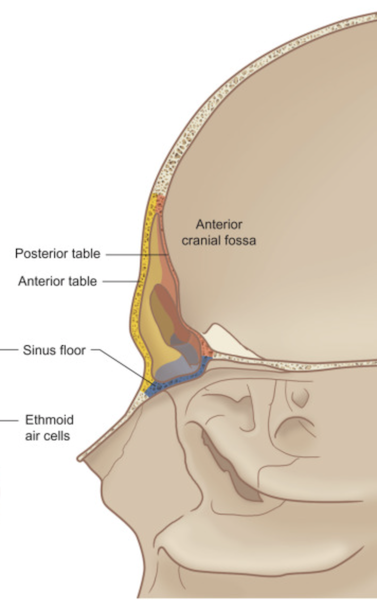
Frontal sinus fractures are relatively uncommon because the frontal bone is one of the strongest bones in the facial skeleton. Significant force is generally required to produce injury, making associated intracranial and cervical spine injuries common. The most important ED concerns are posterior table involvement, CSF leak, intracranial communication, and disruption of sinus drainage pathways.
Patients should be specifically questioned about clear rhinorrhea/intermittent nasal drainage and postnasal drip/salty or sweet taste in the mouth. These symptoms may be subtle and often are not volunteered spontaneously. A useful bedside maneuver is asking the patient to lean forward. If a CSF leak is present, drainage often becomes much more obvious in this position.
Complications of Frontal Sinus Fractures
- CSF leak
- Intracranial communication
- Meningitis
- Chronic sinus obstruction
- Mucocele formation
Posterior table fractures and frontal sinus floor fractures warrant urgent specialist involvement because of the risk of intracranial communication and long-term complications. In contrast, isolated anterior table fractures are frequently managed with delayed reassessment once swelling improves.
Orbital Fractures: Focus on the Eye, Not the Fracture
Orbital fractures are among the most common facial fractures encountered in Emergency Medicine, but the fracture itself is rarely the emergency. The eye is.
Orbital Examination
- Visual acuity
- Pupillary examination
- Relative afferent pupillary defect
- Extraocular movements
- Diplopia assessment
- Globe position
- Intraocular pressure when appropriate
Pearl: Assess globe position from below while the patient looks upward. Subtle asymmetry is often easier to appreciate from this perspective than from a standard frontal view.
Infraorbital numbness/decreased sensation to light touch is another important finding and strongly suggests orbital floor involvement.
Episode 107 – Blunt Ocular Trauma
Orbital Compartment Syndrome
Orbital compartment syndrome is one of the true vision-threatening emergencies in facial trauma. Retrobulbar hemorrhage can rapidly elevate orbital pressure, compromise optic nerve perfusion, and result in irreversible blindness.
Clinical features include:
- Decreased visual acuity
- Proptosis
- Relative afferent pupillary defect (RAPD)
- Elevated intraocular pressure
- Ophthalmoplegia
Emergency physicians must be prepared to perform lateral canthotomy and cantholysis when orbital compartment syndrome is suspected rather than delaying intervention while awaiting specialist arrival.
Pitfall: Waiting for CT imaging before performing a lateral canthotomy in a patient with clear clinical evidence of orbital compartment syndrome.
Pearl: large orbital fractures often appear alarming on CT but are actually less likely to trap extraocular muscles than smaller fractures.
Immediate Consultation for Orbital Injuries
- Visual loss
- Orbital compartment syndrome
- Retrobulbar hematoma
- Extraocular muscle entrapment
- Globe injury
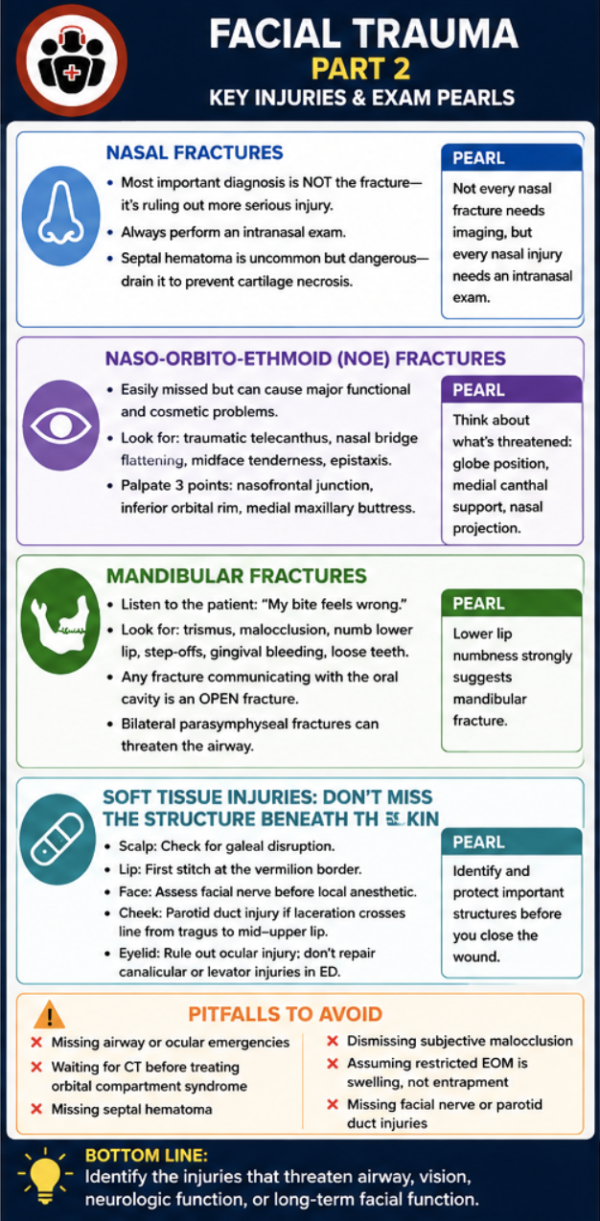
Facial Injuries Part 2: Key Injuries and Physical Exam Pearls
Nasal Fractures: The Most Important Diagnosis Is Not the Fracture
Nasal fractures are the most common facial fractures, yet they are also among the most over-imaged. In most cases, the diagnosis is clinical and imaging rarely changes management. The more important question is not whether the nose is broken, but whether the injury represents an isolated nasal fracture or a more significant midface injury and whether or not a septal hematoma is present. Patients frequently present with swelling, epistaxis, and tenderness that make fracture diagnosis obvious. What is less obvious is the associated injury pattern. Widening of the nasal bridge, traumatic telecanthus, orbital findings, malocclusion, clear rhinorrhea, or significant midface tenderness should prompt consideration of a more complex facial injury.
Nasal Trauma Examination
- External deformity
- Septal hematoma assessment
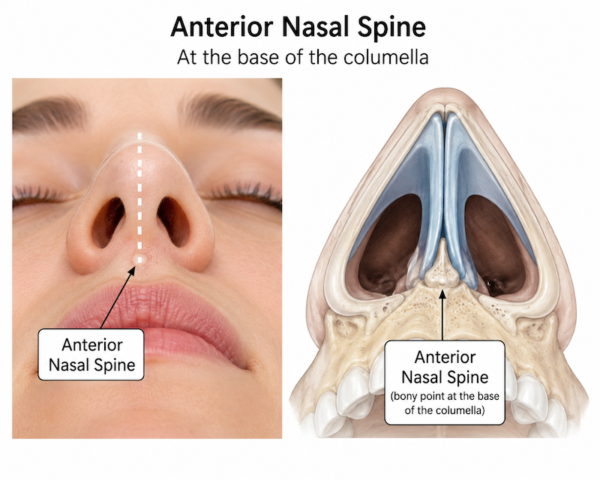
- Anterior nasal spine palpation
- Evaluation for CSF rhinorrhea
Pearl: Palpation tenderness or instability of the anterior nasal spine at the base of the columella should raise suspicion for a more significant central facial injury rather than an isolated nasal fracture.
Septal hematoma
Although relatively uncommon, failure to identify and treat a septal hematoma can result in cartilage necrosis, septal abscess, septal perforation, and permanent saddle-nose deformity. Because these complications are preventable, every patient with nasal trauma requires an intranasal examination regardless of how minor the injury appears externally. Septal hematomas appear as fluctuant swelling along the nasal septum and may be bilateral. Because the septal cartilage relies on the overlying perichondrium for its blood supply, untreated hematomas can rapidly result in cartilage necrosis.
Distinguishing a septal hematoma from simple post-traumatic edema is primarily a tactile, not just visual, diagnosis. A septal hematoma is boggy and fluctuant, whereas post-traumatic edema is typically firm and diffuse. Palpate both sides of the septum—hematomas often produce smooth, bilateral bulging that narrows the nasal airway. If the finding is equivocal, have a low threshold to perform needle aspiration or a small incision. A negative aspiration causes little harm, whereas early drainage of a septal hematoma prevents cartilage necrosis and permanent saddle nose deformity.

Pearl: A septal hematoma is boggy and fluctuant, whereas traumatic edema is typically firm and diffuse. If the finding is equivocal, have a low threshold to aspirate or incise a suspicious lesion—missing a septal hematoma risks cartilage necrosis and permanent saddle nose deformity, while a negative aspiration causes minimal harm.
When Is Imaging Necessary for Suspected Nasal Fractures?
Imaging is generally unnecessary for isolated nasal fractures because management is determined by physical examination findings rather than radiographic appearance. CT imaging should be reserved for patients with suspected:
- NOE fractures
- Orbital fractures
- Le Fort fractures
- Significant midface instability
- CSF leak
- Other associated facial fractures requiring operative planning
Naso-Orbito-Ethmoid (NOE) Fractures: The Easily Missed Midface Injury
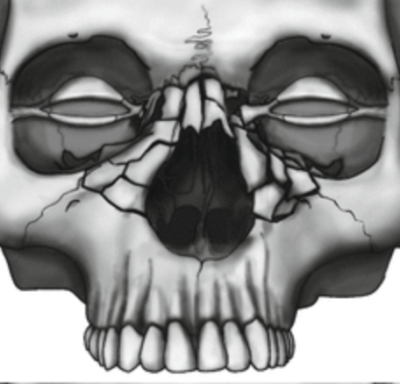
NOE fractures are among the most commonly missed clinically significant facial fractures because the external findings may initially appear deceptively subtle. These injuries occur within the central midface where the nasal bones, ethmoid bone, medial orbital walls, and facial buttresses converge. Unlike isolated nasal fractures, NOE fractures threaten both function and appearance. Disruption of the central facial support structures may affect globe position, medial canthal support, nasal projection, sinus drainage, and facial symmetry.
The most important examination finding is traumatic telecanthus. The medial canthal tendon anchors the eyelids to the central facial skeleton. Disruption of this attachment widens the distance between the medial canthi and alters normal eyelid position. Telecanthus may be subtle initially and become more apparent as swelling resolves.

Left image: Left telecanthus, Right image: post reconstruction of NOE fracture
Clinical Findings Suggestive of an NOE Fracture
- Traumatic telecanthus
- Flattening of the nasal bridge
- Severe periorbital ecchymosis
- Central midface tenderness
- Orbital injury
- Midface instability
A practical examination strategy is to assess tenderness at three key locations:
- Nasofrontal junction
- Inferior orbital rim
- Medial maxillary buttress near the piriform aperture
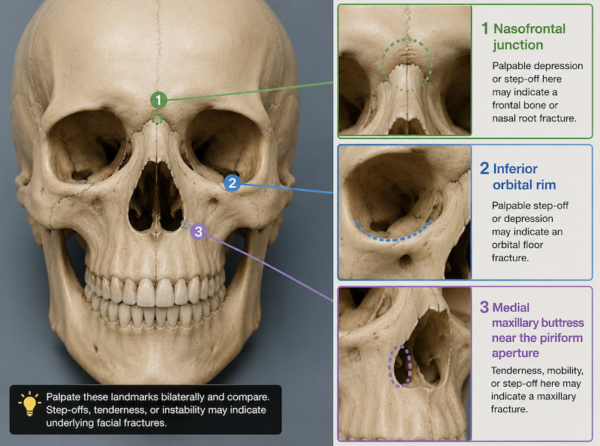
Key palpation points to screen for NOE fracture
Tenderness involving all three regions should raise suspicion for an NOE fracture rather than isolated nasal trauma.
Why NOE Fractures Matter
Potential complications include:
- Telecanthus
- Orbital injury
- Nasofrontal duct disruption
- Cosmetic deformity
- Midface instability
- CSF leak
Because of their proximity to the orbit and skull base, NOE fractures should prompt careful evaluation for ocular injury, CSF leak, and associated midface fractures.
Clinical Pearl: When evaluating an NOE fracture, think about what functions are threatened: globe position, medial canthal support, nasal projection, and central facial stability.
Mandibular Fractures Assessment and Management
Mandibular fractures are among the most clinically important facial injuries because of their effects on airway patency, mastication, occlusion, and lower facial support. One of the highest-yield lessons in mandibular trauma is that patients often provide the diagnosis before the physical examination begins. Subjective malocclusion is one of the most useful indicators of a clinically important mandibular fracture. When a patient says, “My bite feels wrong,” that complaint should be taken seriously regardless of how normal the jaw appears externally.
Key Examination Findings
- Subjective malocclusion
- Trismus
- Gingival bleeding
- Loose teeth
- Dental injury
- Lower lip numbness
- Step-offs
- Crepitus
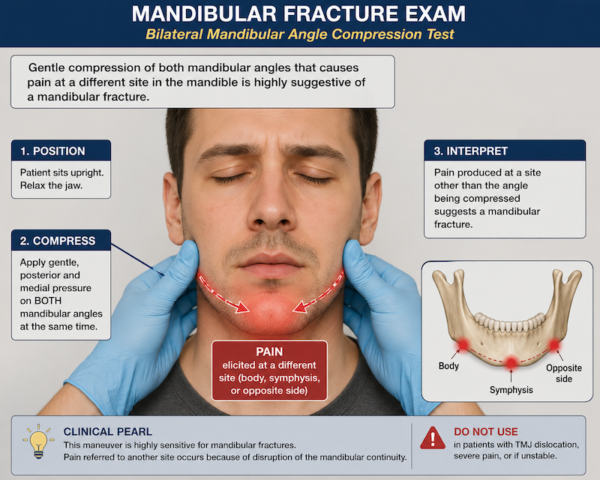
Lower lip numbness deserves particular attention because it suggests injury to the inferior alveolar nerve and is strongly associated with mandibular fracture. Rather than focusing solely on the site of impact, the entire mandible should be examined as a ring structure. Fractures often occur in more than one location. Gentle compression of the mandibular angles may reproduce pain from fractures remote from the area of tenderness and can be a useful adjunct to palpation.
The tongue depressor test remains a useful screening tool. Patients with an intact mandible can usually bite hard enough to break a tongue depressor while those with a mandibular fracture frequently cannot. While helpful, the test should not replace a comprehensive examination.
Pearl: gentle compression of both mandibular angles that cause pain at a different site in the mandible is highly suggestive of a mandibular fracture
Open Mandibular Fractures
Any fracture that communicates with the oral cavity through the tooth-bearing portion of the mandible is, by definition, an open fracture because oral bacteria have direct access to the fracture site. These injuries carry an increased risk of infection and osteomyelitis and generally warrant antibiotic prophylaxis.
Clues to an Open Mandibular Fracture
- Gingival lacerations
- Bleeding around teeth
- Visible fracture lines
- Exposed bone
- Mobile teeth adjacent to the fracture
Airway Pearl: Bilateral Parasymphyseal Fractures
Among all mandibular fracture patterns, bilateral parasymphyseal fractures deserve special attention because they can eliminate anterior support of the tongue and floor of mouth, resulting in posterior tongue displacement and airway obstruction. If airway compromise develops, temporary tongue traction using a towel clip or heavy suture can be an effective bridge to definitive airway management.
Mandibular Fractures Requiring Urgent Consultation
- Open fractures
- Significant malocclusion
- Bilateral fractures
- Airway compromise
- Inability to tolerate oral intake
- Major functional impairment
Many isolated mandibular fractures without airway concerns or severe malocclusion can be managed with analgesia, a soft diet, and outpatient follow-up.
Facial Soft Tissue Injuries: Don’t M iss the Structure Beneath the Skin
One of the most important principles in facial trauma is that the goal is not simply to close a wound. The real objective is identifying and protecting the important structures beneath the skin. A cosmetically imperfect repair can often be revised later. A missed facial nerve injury, parotid duct injury, canalicular injury, or galeal disruption may result in permanent functional deficits. Before repairing any facial laceration, ask: What important structure lies underneath this wound?
Scalp and Forehead Lacerations: Don’t Miss the Galea
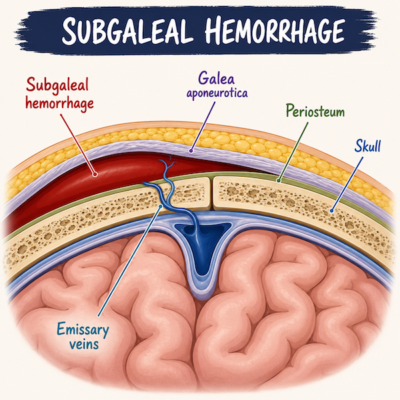
Scalp wounds often appear dramatic because of the rich vascular supply of the scalp. The key management decision is determining whether the galea aponeurotica has been violated. Missed galeal injuries can result in wound dehiscence, widening of the scar, poor cosmetic outcomes, subgaleal hematoma and impaired healing. The galea is hard and white so relatively easy to identify. Deep scalp wounds should therefore be carefully inspected for visible disruption of the galea, and repaired accordingly to prevent subgaleal hematoma formation.
Lip Lacerations: Vermilion Border Considerations and Through-and-Through Lacerations
Lip lacerations create significant anxiety because even small alignment errors can produce highly visible cosmetic deformities. The most important landmark is the vermilion border. Misalignment by as little as 1–2 mm may be noticeable after healing. For this reason, the first suture should almost always be placed at the vermilion border. Once perfect alignment is achieved, the remainder of the repair becomes significantly easier.
Pearl: In order to ensure that the vermilion border lines up Dr. Fialkov recommends before infiltrating local anesthetic, use a #15 blade to place a tiny score mark on each side of the vermilion border. Unlike a skin marker, the scores won’t wash off or disappear after epinephrine-induced blanching, making accurate alignment of the first vermilion border suture much easier.
Through-and-Through Lip Lacerations
Layered closure may be required: Oral mucosa, orbicularis oris muscle, outer layer/vermilion border
Facial Nerve and Parotid Duct Injuries
Facial nerve and parotid duct injuries are frequently missed because clinicians focus on the skin defect rather than the structures beneath it. Facial nerve function should always be documented before infiltration of local anesthetic.
Facial Nerve Examination
| Facial Nerve Branch | Examination |
|---|---|
| Frontal | Raise eyebrows |
| Zygomatic | Close eyes tightly |
| Buccal | Smile/show teeth |
| Marginal mandibular | Depress lower lip |
| Cervical | Tense platysma |
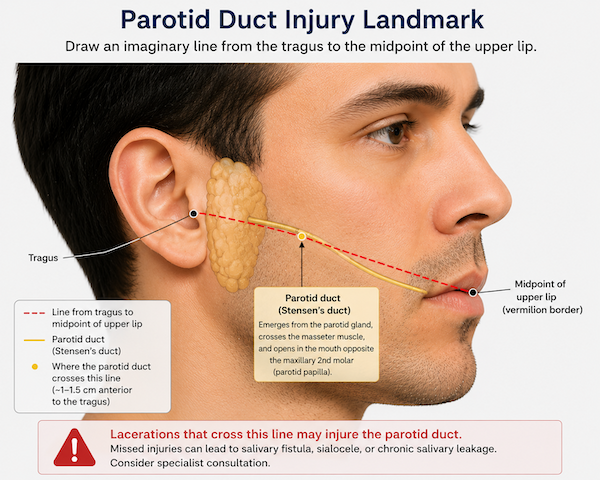
Parotid Duct Injuries
A useful landmark is the line extending from the tragus to the midpoint of the upper lip. Any cheek laceration crossing this line should raise concern for parotid duct injury.
Potential complications include:
- Salivary fistula
- Sialocele
- Chronic salivary leakage
- Delayed reconstructive surgery
Clinical Pearl Any cheek laceration crossing a line from the tragus to the lip should prompt consideration of parotid duct injury.
Eyelid Lacerations: Know When Not to Repair
The most important question in eyelid trauma is not how to repair the wound but whether there is an associated ocular injury. Vision-threatening ocular injuries always take priority over eyelid closure. Particular attention should be paid to injuries involving the medial canthus because of the risk of canalicular injury. Attempting repair before specialist evaluation may make definitive repair more difficult.
Eyelid Injuries Requiring Specialist Consultation
- Canalicular injuries
- Medial canthal injuries
- Lid margin involvement
- Tarsal plate injuries
- Full-thickness eyelid lacerations
- Ptosis suggesting levator injury
A useful principle is that skin can always be closed later. A missed canalicular injury or levator injury is much harder to fix than an open eyelid wound.
Pitfall: A common pitfall is attributing ptosis to swelling along. Ptosis after eyelid trauma should raise concern for levator injury rather than simply being attributed to swelling.
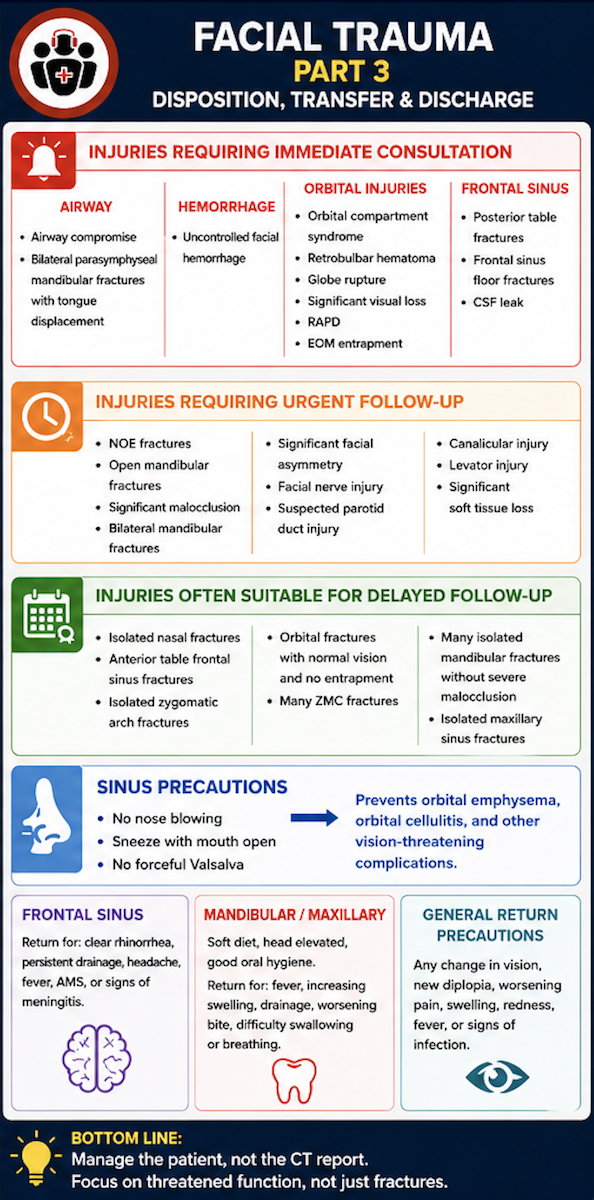
Facial Injuries Requiring Immediate Consultation
Certain injuries threaten airway, vision, or neurologic function and require immediate specialist involvement.
Airway
- Airway compromise
- Progressive facial swelling threatening the airway
- Bilateral parasymphyseal mandibular fractures with tongue displacement
Hemorrhage
- Uncontrolled facial hemorrhage
- Persistent bleeding despite packing and resuscitation
Orbital Injuries
- Orbital compartment syndrome
- Retrobulbar hematoma
- Globe rupture
- Significant visual loss
- Relative afferent pupillary defect
- Extraocular muscle entrapment
Frontal Sinus Injuries
- Posterior table fractures
- Frontal sinus floor fractures
- CSF leak
These injuries are true emergencies because delays in treatment may result in blindness, intracranial complications, airway loss, or life-threatening hemorrhage.
Facial Injuries Requiring Urgent Specialist Follow-Up
Many facial injuries require specialist assessment but not necessarily immediate intervention.
Urgent Facial Trauma Assessment
- Naso-orbito-ethmoid (NOE) fractures
- Open mandibular fractures
- Significant malocclusion
- Bilateral mandibular fractures
- Significant facial asymmetry
- Facial nerve injury
- Suspected parotid duct injury
- Canalicular injury
- Levator injury
- Significant soft tissue loss
The timing of specialist assessment will depend on local resources, but these patients generally warrant expedited review because delayed treatment may affect long-term function or cosmetic outcome.
Facial Injuries Often Suitable for Delayed Follow-Up
Many fractures are actually best assessed after swelling has improved. For these injuries, immediate operative decisions are often difficult because edema obscures the true degree of deformity.
Injuries Commonly Managed with Delayed Follow-Up
- Isolated nasal fractures
- Anterior table frontal sinus fractures
- Isolated zygomatic arch fractures
- Orbital fractures with normal vision and no entrapment
- Many uncomplicated zygomaticomaxillary complex fractures
- Many isolated mandibular fractures without severe malocclusion
- Isolated maxillary sinus fractures
Patients with these injuries frequently benefit from reassessment several days later after swelling has subsided and facial symmetry can be more accurately evaluated.
Discharge Instructions for Facial Fractures
Discharge instructions are often overlooked but can significantly affect outcomes.
Upper Facial and Orbital Fractures
Patients should return immediately for:
- Any change in vision
- New diplopia
- Worsening pain
- Increasing swelling
- Progressive redness
- Fever
- Signs of infection
Patients should be warned that orbital complications occasionally evolve over hours to days and that delayed deterioration requires urgent reassessment.
Sinus Precautions
Fractures involving the orbit, maxilla, NOE complex, frontal sinus, or other paranasal sinus structures require strict sinus precautions.
Patients should be instructed to:
- Avoid blowing their nose
- Sneeze with their mouth open
- Avoid forceful Valsalva maneuvers
The rationale is important. Forceful nose blowing can introduce air and bacteria into the orbit through fracture defects, resulting in orbital emphysema, orbital cellulitis, and potentially vision-threatening complications.
Frontal Sinus Fractures discharge instructions
Patients with frontal sinus injuries should be instructed to return for:
- Clear rhinorrhea
- Persistent nasal drainage
- New headache
- Fever
- Altered level of consciousness
- Symptoms concerning for meningitis
Because CSF leaks may not be apparent initially, patients should be educated about delayed presentations.
Mandibular and Maxillary Fractures discharge instructions
Patients discharged with lower facial fractures should generally be instructed to:
- Maintain a soft or pureed diet
- Elevate the head when resting
- Avoid further facial trauma
- Maintain good oral hygiene
Return precautions include:
- Fever
- Increasing swelling
- Purulent drainage
- Worsening malocclusion
- Difficulty swallowing
- Difficulty breathing
For most isolated mandibular fractures, infection is the primary delayed complication of concern.
Facial Fracture Summary Table
| Fracture Type | What Is It? | Why It’s Important | Key Complications | Key Physical Exam Findings | Imaging Pearls | Urgency of Consultation |
|---|---|---|---|---|---|---|
| Frontal Sinus Fracture | Fracture involving the anterior table, posterior table, or floor of the frontal sinus | May communicate with the intracranial space or disrupt sinus drainage pathways | CSF leak, meningitis, intracranial communication, chronic sinus obstruction, mucocele formation | Forehead swelling, periorbital ecchymosis, raccoon eyes, CSF rhinorrhea, salty/sweet taste, clear nasal drainage | Distinguish anterior table from posterior table and floor fractures; posterior table and floor injuries are the important ones | Immediate: Posterior table fracture, frontal sinus floor fracture, CSF leak. Delayed: Isolated anterior table fracture |
| Orbital Fracture | Fracture of the orbital floor, medial wall, roof, or lateral wall | The fracture itself is rarely the emergency; ocular injury is | Retrobulbar hematoma, orbital compartment syndrome, muscle entrapment, persistent diplopia, enophthalmos, hypoglobus | Visual acuity changes, diplopia, restricted EOMs, ptosis, globe asymmetry, infraorbital nerve numbness | Large fractures often look worse than they are; clinical exam drives management more than CT appearance | Immediate: Visual loss, orbital compartment syndrome, retrobulbar hematoma, entrapment. Delayed: Enophthalmos, hypoglobus, large fractures without ocular dysfunction |
| Nasal Fracture | Isolated fracture of the nasal bones | Usually a minor injury; the main concern is associated injuries and septal hematoma | Septal hematoma, septal abscess, septal necrosis, saddle nose deformity | Nasal deformity, tenderness, epistaxis, septal hematoma on intranasal exam | Imaging rarely needed for isolated nasal fractures | Usually outpatient follow-up after swelling resolves |
| NOE (Naso-Orbito-Ethmoid) Fracture | Central midface fracture involving nasal bones, ethmoid, medial orbital walls, and adjacent buttresses | Commonly missed; affects facial support, canthal position, and sinus drainage | Telecanthus, orbital injury, cosmetic deformity, nasofrontal duct injury, midface instability | Telecanthus, periorbital ecchymosis, tenderness at nasofrontal junction, infraorbital rim, and medial maxillary buttress | Often mistaken for a nasal fracture; diagnosis depends heavily on exam | Urgent facial trauma assessment |
| Zygomaticomaxillary Complex (ZMC) Fracture | Fracture involving the zygoma and its articulations with the orbit, maxilla, frontal bone, and temporal bone | Can affect globe position, orbital support, and facial width/projection | Enophthalmos, hypoglobus, infraorbital nerve injury, cosmetic deformity | Flattened cheek prominence, infraorbital numbness, tenderness over zygoma and orbital rim, globe asymmetry | Often associated with orbital fractures; assess orbit carefully | Usually urgent but not emergent unless associated ocular injury is present |
| Le Fort Fractures | High-energy midface fractures involving combinations of maxillary, NOE, and zygomatic complexes | Marker of significant force transmission and associated injuries | Airway compromise, hemorrhage, CSF leak, BCVI, facial instability | Midface mobility, malocclusion, facial swelling, epistaxis, associated orbital findings | Rarely occur as “pure” Le Fort I, II, or III injuries; think in terms of disrupted facial complexes | Depends on associated airway, ocular, neurologic, and hemorrhagic complications |
| Mandibular Fracture | Fracture involving condyle, angle, body, symphysis, or parasymphysis | Affects airway, occlusion, mastication, and lower facial support | Airway obstruction, malocclusion, osteomyelitis, inferior alveolar nerve injury | Subjective malocclusion, trismus, gingival bleeding, loose teeth, lower lip numbness | CT is preferred when available; many fractures communicate with the oral cavity and are open fractures | Urgent: Open fractures, bilateral fractures, significant malocclusion, airway concerns. Outpatient: Many isolated fractures |
Soft tissue facial injury summary table
| Soft Tissue Injury | Why It’s Important | Key Physical Exam Findings | Critical Pearl from Dr. Fialkov | Specialist Consultation Needed? |
|---|---|---|---|---|
| Scalp & Forehead Lacerations (Galeal Injuries) | Missing a galeal injury can lead to wound dehiscence, hematoma and poor cosmetic outcomes | Deep forehead/scalp laceration with visible galea or separation of galeal edges | Always inspect for galeal disruption and repair the galea before closing the skin | Usually no if galea can be repaired appropriately |
| Lip Lacerations | Small errors in alignment produce obvious long-term cosmetic deformity | Vermilion border disruption, through-and-through lacerations, intraoral extension | The first stitch should precisely align the vermilion border; if that stitch is perfect, the rest of the repair is usually easy; consider scoring the skin with #15 blade | Usually no; most can be repaired in the ED |
| Facial Nerve & Parotid Duct Injuries | Frequently missed injuries that may result in permanent facial weakness or salivary fistula formation | Facial asymmetry, weakness of facial expression, cheek laceration along the tragus-to-upper-lip line, clear fluid from wound | Document facial nerve function before injecting local anesthetic. Any laceration crossing a line from the tragus to the mid-upper lip should raise suspicion for parotid duct injury | Yes if facial nerve injury or parotid duct injury suspected |
| Eyelid Lacerations | Missing canalicular or levator injuries can cause permanent tearing or eyelid dysfunction | Medial canthus involvement, lid margin disruption, ptosis, tarsal plate involvement, inner eyelid injury | A missed canalicular injury is much harder to fix than an open eyelid wound. Look carefully for canalicular injuries, lid margin injuries, and ptosis suggesting levator injury | Yes for canalicular injuries, medial canthal injuries, lid margin injuries, ptosis, tarsal plate involvement |
Key take home points on facial injuries
- Facial fractures are markers of force transmission; always look for associated injuries.
- Facial fractures rarely obstruct the airway directly; bleeding, loose teeth, and soft tissue displacement are more common causes.
- Reassess the airway frequently because deterioration is often delayed.
- The bilateral parasymphyseal mandibular fracture is the classic fracture associated with airway obstruction.
- Visual acuity and gross hearing testing should be documented in every patient with significant facial trauma.
- Telecanthus is one of the most important clues to an NOE fracture.
- Lower lip numbness strongly suggests mandibular fracture.
- Any mandibular fracture communicating with the oral cavity is an open fracture.
- Before closing a facial laceration, identify the important structure beneath it.
- Do not wait for CT imaging before treating orbital compartment syndrome.
- Think in terms of bony complexes: upper face, midface, and mandible rather than memorizing Le Fort classifications.
- Posterior table and frontal sinus floor fractures are the frontal sinus injuries that matter most.
- Large orbital fractures are often less dangerous than small fractures.
- Facial nerve, parotid duct, canalicular, and levator injuries are commonly missed.
References
- American College of Surgeons Committee on Trauma. Advanced Trauma Life Support (ATLS®): Student Course Manual. 11th ed. Chicago, IL: American College of Surgeons; 2023.
- Holmes JF, Akkinepalli R. Computed tomography versus physical examination in the identification of facial fractures in patients with blunt trauma. Ann Emerg Med. 2005;45(2):196-200.
- Hohlrieder M, Hinterhoelzl J, Ulmer H, et al. Maxillofacial fractures masking traumatic brain injury. Int J Oral Maxillofac Surg. 2004;33(4):389-395.
- Advanced Trauma Life Support Subcommittee, American College of Surgeons Committee on Trauma. Advanced Trauma Life Support (ATLS®): the ninth edition. J Trauma Acute Care Surg. 2013;74(5):1363-1366.
- Ellis E III, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol. 1985;59(2):120-129.
- Bynoe RP, Kerwin AJ, Parker HH III, et al. Maxillofacial injuries and life-threatening hemorrhage: treatment with transcatheter arterial embolization. J Trauma. 2003;55(1):74-79.
- Cogbill TH, Cothren CC, Ahearn MK, et al. Management of maxillofacial injuries with severe hemorrhage. J Trauma. 2000;48(2):311-316.
- Hoffmann J, Cornelius CP, Groten M, et al. The comprehensive examination of facial trauma. J Craniomaxillofac Surg. 2015;43(7):1207-1215.
- Manson PN, Markowitz B, Mirvis S, et al. Toward CT-based facial fracture treatment. Plast Reconstr Surg. 1990;85(2):202-212.
- Le Fort R. Experimental study of fractures of the upper jaw. Rev Chir Paris. 1901;23:208-227.
- Strong EB, Sykes JM. Frontal sinus fractures. Facial Plast Surg Clin North Am. 2006;14(1):25-34.
- Alinasab B, Borstedt K, Rudström H, et al. Ocular injuries associated with orbital fractures. Craniomaxillofac Trauma Reconstr. 2014;7(2):103-107.
- Lima V, Burt B, Leibovitch I, et al. Orbital compartment syndrome: the ophthalmic surgical emergency. Surv Ophthalmol. 2009;54(4):441-449.
- Jordan DR, Allen LH, White J, et al. Intervention within days for some orbital floor fractures: the white-eyed blowout fracture. Ophthalmic Plast Reconstr Surg. 1998;14(6):379-390.
- Higuera S, Lee EI, Cole P, Hollier LH Jr, Stal S. Nasal trauma and the deviated nose. Plast Reconstr Surg. 2007;120(7 Suppl 2):64S-75S.
- Rohrich RJ, Adams WP Jr. Nasal fracture management: minimizing secondary nasal deformities. Plast Reconstr Surg. 2000;106(2):266-273.
- Markowitz BL, Manson PN. Naso-orbito-ethmoid fractures. Clin Plast Surg. 1989;16(1):49-62.
- Banks P. Killey and Kay’s Fractures of the Mandible. 4th ed. Oxford, UK: Wright; 2001.
- Alonso N, de Freitas RS, de Oliveira e Cruz GA. The tongue blade test in mandibular fractures. J Craniofac Surg. 2005;16(6):1021-1023.
- AO Foundation. AO CMF Surgery Reference: Mandible Fractures. AO Foundation. Accessed June 2026.
- Trott A. Wounds and Lacerations: Emergency Care and Closure. 5th ed. Philadelphia, PA: Elsevier; 2020.
- Singer AJ, Hollander JE, Quinn JV. Evaluation and management of traumatic lacerations. N Engl J Med. 1997;337(16):1142-1148.
- Lewis G, Knottenbelt JD. Parotid duct injuries associated with facial trauma. Injury. 1991;22(5):393-394.
- American Academy of Ophthalmology. Oculoplastic and Orbital Trauma Preferred Practice Pattern. San Francisco, CA: American Academy of Ophthalmology; 2024.
- VandeGriend ZP, Hashemi A, Stepan JG, et al. Appropriateness of interfacility transfer for isolated facial fractures. J Oral Maxillofac Surg. 2020;78(8):1396-1403.
Drs. Helman, Petrosoniak and Fialkov have no conflicts of interest to declare
Now test your knowledge with a quiz.



Great episode full of pearls! Thanks you for this comprehensive review :)
A minor detail I’d add, that I don’t see in the write-up is: looking for tooth fragments in lip / through and through injuries as they may become a site for infection