
This is EM Cases Episode 90 – Low and Slow Poisoning.
One of the things we need to think about whenever we see a patient who’s going low and slow with hypotension and bradycardia is an overdose. B-blockers, calcium channel blockers (CCB) and digoxin are some of the most frequently prescribed cardiovascular drugs. And inevitably we’re going to be faced with both intentional and unintentional overdoses from these drugs in the ED. On this EM Cases podcast the Medical Director of The Ontario Poison Control Centre and Emergency Physician at St. Michael’s Hospital, Dr. Margaret Thompson, along with Dr. Emily Austin, Emergency Physician and Toxicologist at St. Michael’s Hospital, help us to recognize these overdoses early and manage them appropriately.
Podcast: Play in new window | Download (Duration: 1:36:19 — 88.2MB)
Subscribe: Apple Podcasts
Written Summary and blog post written by Keerat Grewal & Anton Helman, edited by Anton Helman January, 2017
Cite this podcast as: Helman, A, Thompson, M, Austin, E. Low and Slow Poisoning. Emergency Medicine Cases. January, 2017. https://emergencymedicinecases.com/aortic-dissection-em-cases-course/. Accessed [date].
Differential Diagnosis of Low and Slow
Non-toxicological causes:
- MI with cardiogenic shock
- Hyperkalemia
- Myxedema coma
- Spinal cord injury
- Hypothermia
Toxicological causes:
- Calcium channel blockers
- Beta-blockers
- Digoxin
- Opiates
- Alpha-2 antagonists (e.g., clonidine)
- Sodium channel blockers (e.g., TCA, carbamazepine, flexeril, antipsychotics, propranolol, cocaine)
Management of Seizures in the Toxicology Patient
There are several modifications of the usual algorithm for treating adult seizures when it comes to the poisoned patient.
Avoid Sodium Channel Blockers
Benzodiazepines are the first line treatment for treating seizures in patients with an overdose. In toxicological seizures, do not treat with antiepileptic drugs that have sodium channel blockade (i.e., phenytoin, fosphenytoin) because many poisons block sodium channels and additional sodium channel blockade may result in cardiac instability. If seizures persist, even after large doses of benzodiazepines, consider advancing to phenobarbital or propofol.
Bicarbonate
In patients with an overdose who are seizing and have evidence of sodium channel blockade (wide QRS on EKG), give sodium bicarbonate.
Naloxone
Consider naloxone in patients who may have an opioid overdose and are seizing. Some opioids can cause seizures (i.e., meperidine). Opioids may also cause hypoperfusion, which can lead to seizures.
General Approach to the Management of Beta Blocker and Calcium Channel Blocker Overdoses
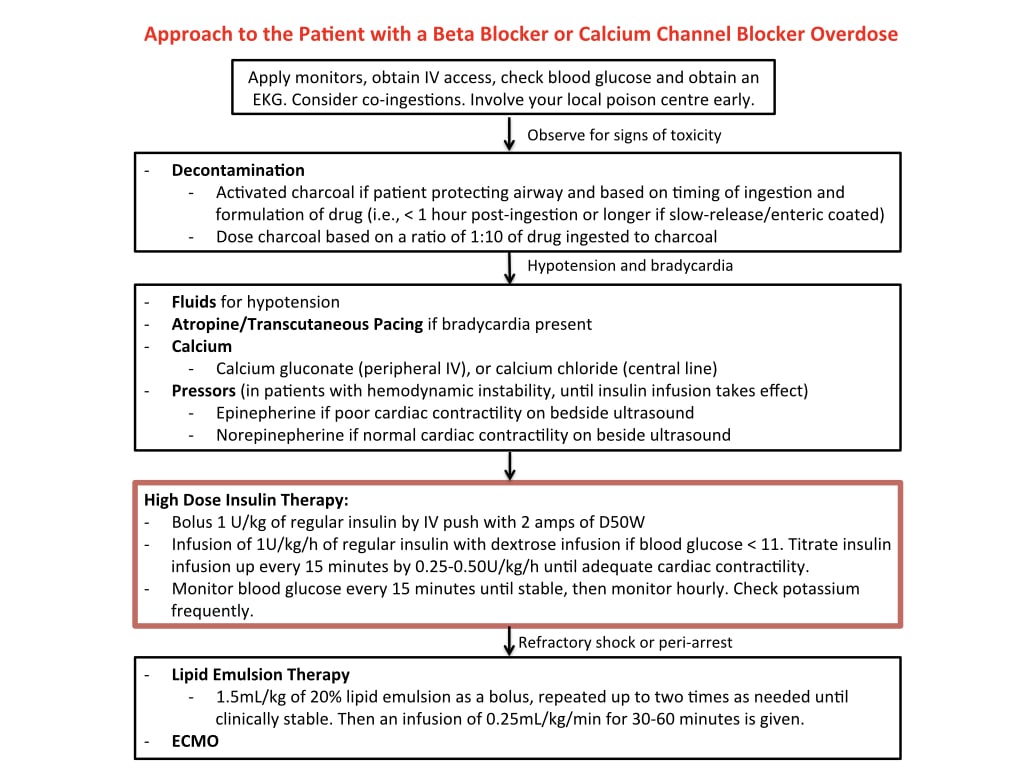
A) Fluids
Establish two IVs and give the patient a fluid bolus of normal saline (1-2 liters) to start.
B) Decontamination
Activated charcoal
Consider decontamination with a dose of activated charcoal. The dose of activated charcoal is determined by the dose of the drug ingested in a 10:1 ratio of charcoal to drug. For example, a single 240mg tablet of Diltiazem requires only 2.4g of activated charcoal.
Factors to consider in the decision to give activated charcoal:
- Does the drug bind to charcoal?
Charcoal does not bind lithium or iron, therefore, should not be given for overdoses of these drugs.
- Was the drug ingested within one hour?
For most drugs, activated charcoal is indicated within one hour of ingestion only.
- Is the drug likely to stay in the stomach for a prolonged time (beyond the one hour post-ingestion)?
Some drugs will stay in the stomach or upper intestinal tract for a prolonged period of time. In overdoses that involve drugs with these properties, charcoal should still be considered even if the ingestion occurred more than one hour ago. Examples of such drugs would include medications that are extended release formulations, enteric-coated medications, opioids and anticholinergic medications that delay gastric emptying, ASA, and theophylline.
- Is the patient protecting their airway?
Aspiration pneumonitis is the most common complication of activated charcoal administration. If you suspect that a patient not be able to protect their airway because of altered level of awareness or anticipated seizure, avoid the use of activated charcoal.
Gastric lavage should only be considered for a massive life-threatening ingestion if it can be undertaken within 60 minutes of ingestion, and if the size of the tablets taken is smaller than that of the lavage tube (36-40f). Remember that these patients will need their airway secured prior to placement of the lavage tube. There is no evidence to suggest that gastric lavage reduces mortality from overdose.
Whole bowel irrigation
There is no evidence that whole bowel irrigation improves outcomes in overdoses.
Consider whole bowel irrigation in 3 situations:
- Large drugs not bound by charcoal: iron, lithium, potassium
- Body packers
- Massive overdoses of extended release medications
Go to Episode 5 for a discussion on body packer management
C) Atropine
Consider a trial of 0.5mg IV atropine in patients with bradycardia.
What about cardiac pacing? In the overdose patient, transcutaneous pacing is unlikely to be successful, but may be attempted. If transcutaneous pacing is unsuccessful, it is generally agreed that transvenous pacing should be avoided in the patient with a slow and low poisoning as it may precipitate dysrhythmias in the overdose patient with an ‘irritable’ heart.
C) Calcium
Calcium Gluconate 3amps IV push or Calcium Chloride 1amp IV push if a central line is established followed by infusion if an effect is seen.
C) High Dose Insulin
High dose Regular Insulin 1 U/kg plus 2 amps D50W IV push
Follow with 1 U/kg/hr insulin drip with 0.5 g/kg/hr dextrose if serum glucose <11
Titrate up q15 mins by 0.25-0.5U/kg/hr until cardiac contractility is adequate based on POCUS findings and vital signs
B-blocker poisoning usually requires more insulin than CCB poisoning
Monitor serum glucose q15mins, then q1h once the glucose has stabilized Monitor serum potassium
Insulin takes about 30-45 minutes to work – so it needs be to started early
One of the biggest pitfalls in the management of B-blocker overdoses is not giving enough insulin. Patients may require up to 8-10U/kg/hr!
D) Vasopressors
Norepinepherine or epinephrine may be required for hemodynamic support until the insulin takes effect. The choice of medication will depend on cardiac contractility on point of care ultrasound (POCUS). Epinepherine is favored over norepinephrine in patients with evidence of myocardial depression on POCUS. Norepinepherine is favored in patients with normal contractility on POCUS.
E) Glucagon
Glucagon may be considered as a last resort. Our experts do not recommend the routine use of glucagon in beta blocker overdoses. It can worsen hypotension and bradycardia as well as cause vomiting which increases the risk of aspiration.
F) Lipid emulsion therapy
Lipid emulsion therapy (intralipid) is a management option for patients who have overdosed on a lipid soluble drug (e.g., lidocaine/bupivacaine, calcium channel blockers, amitriptyline, seroquel, buproprion) who are in refractory shock or peri-arrest.
There are downsides to lipid therapy including complications such as pancreatitis and pulmonary fat emboli. Electrolytes, blood gases etc. cannot be measured in lipemic serum.
Intralipid treatment should be reserved for lipophilic drug poisoning with:
- Hypotension or
- Dysrhythmias causing hemodynamic instability (not responsive to sodium bicarbonate or lidocaine) or
- Seizures unresponsive to usual treatments
There is no role for lipid emulsion therapy
- as prophylaxis
- in isolated altered mental status or coma
- as 1st line therapy
How do you give lipid emulsion therapy?
Draw up 100mL from a 500mL bag of lipid emulsion and give as an IV bolus, then run the remaining 400mL over 30mins.
G) ECMO for low and slow poisoning
Consider ECMO for calcium channel blocker or beta blocker poisoned patients in refractory shock despite adequate doses of calcium, insulin and vasopressors.
H) Monitoring
Monitor patients carefully for hypoglycemia (glucose q15 mins for first hour then q1h), hypokalemia and volume overload.
Note that nadolol, acebutolol and sotalol are dialyzable.
Beta Blocker Low and Slow Poisoning
ECG Findings in Beta Blocker Overdoses
Bradycardia is the most common ECG finding in beta blocker overdoses. You may see a sinus bradycardia, or any type of heart block (including a complete heart block). A junctional rhythm may be seen.
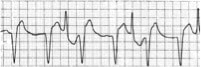
In propranolol overdose, there may be a wide QRS and a tall R wave in aVR due to its sodium channel blocking property. Propanolol is one of the most dangerous beta blockers in overdose. It has significant sodium channel blockade and is lipophilic, therefore, it crosses the blood brain barrier and causes depressed level of consciousness, seizures, and respiratory depression.
In sotolol overdose, the QTc may be prolonged because of its potassium channel blocking properties.
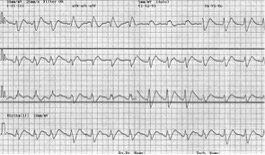
ECG features of propanolol overdose (image from www.lifeinthefastlane.com)
Differentiating Between Calcium Channel Blocker and Beta Blocker Overdoses
There are two key features that may help differentiate a calcium channel blocker overdose from a beta blocker overdose: Blood glucose and level of consciousness. Calcium channel blocker overdoses tend to cause hyperglycemia, compared to a normal-to-low blood glucose in beta blocker overdoses. Beta blocker overdoses tend to cause a depressed level of consciousness, and calcium channel blocker overdoses, a normal level of consciousness.
Digoxin Poisoning
Chronic digoxin poisoning has a higher mortality, more vague symptomatology, and more low and slow compared to acute digoxin poisoning. Ventricular dysrhythmias are more classically associated with acute digoxin poisoning, though can be seen in chronically poisoned patients as well.
The classic patient with digoxin toxicity is the older patient on their usual dose of digoxin who develops vague symptoms such as ‘weak and dizzy’, altered LOA, nausea and visual symptoms along with low and slow vitals.
Classic triggers for digoxin toxicity in the patient taking their usual daily dose:
- Volume depletion (digoxin is excreted renally)
- Recent medication change (there are many drug-drug interactions with digoxin)
The ECG and Digoxin
First, one must distinguish between digoxin effect and digoxin toxicity.
Digoxin effect: ECG characteristics normally seen in a non-toxic patient taking therapeutic doses of digoxin, displays scooped ST segments, otherwise known as ‘The Salvador Dali Moustache’ after the great surrealist painter.
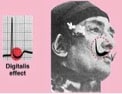
Care of Life in the Fast Lane blog
Digoxin toxicity can cause almost any dysrhythmia except rapid atrial fibrillation. As acute digoxin toxicity often causes hyperkalemia, ECG findings may reflect those of hyperkalemia. (Go to Episode 86 Emergency Management of Hyperkalemia for ECG examples)
Classic digoxin toxicity ECG findings are a result of myocardial irritability or blockade at the AV node and include:
Myocardial irritability:
- Slow atrial fibrillation
- Bidirectional ventricular tachycardia
- Frequent PVCs
AV blockade:
- Junctional rhythm
- AV dissociation
- Heart block
Bidirectional ventricular tachycardia of digoxin poisoning
Pitfalls in Interpreting Digoxin Levels
False positives
- Digoxin levels will always be falsely elevated if taken within 6 hours of ingestion, so you must wait >6 hours to draw the first digoxin level.
- After DigiFab is given, digoxin levels will always be falsely elevated
False negatives
Chronic digoxin toxicity can present with digoxin levels in the therapeutic range, and acute ingestion of nondigoxin cardiac glycosides (e.g. foxglove or oleander)
Treatment of the low and slow digoxin poisoned patient
- Fluid bolus
- Trial of atropine 0.5mg IV
- DigiFab
There is little role for pacing in the slow and low digoxin toxic patient because of increased myocardial irritability and the risk of deterioration into a malignant dysrhythmia.
Transcutaneous pacing may be considered in the unstable slow and low digoxin toxic patient if there is a delay to administration of DigiFab when atropine has failed.
For acute digoxin poisoning with ventricular dysrhythmias, consider IV lidocaine and/or IV esmolol.
Indications for DigiFab antidote
The indications for DigiFab include the following in the setting of suspected digoxin poisoning:
- Hyperkalemia (K >5)
- History of 10mg digoxin ingestion in an adult or 4mg in a child
- Renal Failure
- Ventricular or unstable atrial dysrhythmias
- High digoxin serum level
- Multiple drug ingestions
Dosing DigiFab – a new regimen
In cardiac arrest due to digoxin poisoning give 10 vials of DigiFab and repeat in 15 mins prn x 1 for a total of 20 vials
In chronic digoxin poisoning give 1 vial and repeat prn based on clinical condition, ECG and serum potassium (usually requires approximately 5 vials total)
In acute digoxin poisoning give 2 vials and repeat prn based on clinical condition, ECG and serum potassium (usually requires approximately 10 vials total)
Is calcium safe in hyperkalemic digoxin toxic patients?
Chronic digoxin toxicity typically causes hypokalemia. If a chronic digoxin toxic patient is hyperkalemic it is likely due to acute renal failure and those patients giving calcium is likely safe (unlikely to cause ‘stone heart’).
Acute digoxin toxicity typically causes hyperkalemia due to blockage of Na-K ATPase. These patients do not need anything to stabilize their cardiac membranes or shift potassium. These patients need DigiFab.
Dr. Thompson, Dr. Austin and Dr. Helman have no conflicts of interest to declare
References
St-onge M, Anseeuw K, Cantrell FL, et al. Experts Consensus Recommendations for the Management of Calcium Channel Blocker Poisoning in Adults. Crit Care Med. 2016.
St-onge M, Dubé PA, Gosselin S, et al. Treatment for calcium channel blocker poisoning: a systematic review. Clin Toxicol (Phila). 2014;52(9):926-44.
Levine M, Nikkanen H, Pallin DJ. The effects of intravenous calcium in patients with digoxin toxicity. J Emerg Med. 2011 Jan;40(1):41-6. doi: 10.1016/j.jemermed.2008.09.027. Epub 2009 Feb 6.
Ip D, Syed H, Cohen M. Digoxin specific antibody fragments (Digibind) in digoxin toxicity. BMJ. 2009 Sep 3;339:b2884.
Treatment of Calcium-Channel-Blocker Intoxication with Insulin Infusion NEJM 344:1721-1722. High Dose Insulin Reverses Calcium Channel Blocker Inhibition of Glucose Uptake in an Adipocyte Model Acad Emerg Med 2007: 14:5;195.
The role of insulin and glucose (hyperinsulinemia/euglycemia therapy in acute calcium channel antagonist and beta blocker poisoning. Toxicol Rev. 2004;23(4): 215- 22.
Assessment of hyperglycemia after calcium channel blocker overdoses involving diltiazem or verapamil. Crit Care Med 2007 Sep;35(9):2071-5.
Other FOAMed Resources on slow and low poisoning
The Poison Review on evidence of treatments in CCB overdose
The Poison Review on Lipid Emulsion Therapy for CCB overdose
The Poison Review on Pressors or High Dose Insulin for CCB overdose
The Poison Review on Review of High Dose Insulin for CCB overdose
EMCrit’s take on CCB overdose
Digoxin Tocixicity Management review on Life in the Fast Lane
Now test your knowledge with a quiz.



Excellent session, we do not see much digoxin toxicity as we once did, historically was taught that any tachycardia with block should make you think of digoxin toxicity. With cocaine and TCAD, the bradycardia’s presence depend on the clinical presentation, both can present with tachycardia due to SNS or anticholingeric effects but as the sodium channel blockade begins to take effect, you begin to see the low and slow.
Thank you all for the fabulous explanation , it was really informative talk.superb job
RE: CCB OD: What has been your dosing experience on HIET for obese patients? Is there a max IV bolus and infusion dose in obese patients?
Just want to point out a tiny error…
Clonidine is a-2 AGONIST. a2 is the sympathetic inhibitory pathway – inhibit the inhibitor and you get “excitation” or up regulation of adrenergic/dopaminergic/seratonergic neurotransmitters (however temporary because of negative feedback and other complicated pharm stuff for which I don’t have to mental fortitude to approach at this time).
Thanks as always for the great content! You make our Resident Education so much more enjoyable!