

Hot on the heels of Dr. Scott Weingart’s latest publication in the Annal of EM on Preoxygenation & Delayed Sequence Intubation, we have Dr. Weingart, perhaps the world’s most influential critical care educator, and Dr. Walter Himmel, ‘The Walking Encyclopedia of EM’ discussing how the community ED doc can use preoxygenation, apneic oxygenation and delayed sequence intubation to help improve airway management knowledge and skills. Whether you work in a rural setting or a big urban community hospital, Dr. Himmel and Dr. Weingart explain how these concepts and skills are easily adaptable to your work environment. We introduce the Triple 15 Rule for preoxygenation as a memory aid that will help you the next time you’re faced with a critically ill patient who’s oxygen saturation isn’t good enough on a non-rebreather.
Podcast: Play in new window | Download (Duration: 46:52 — 43.0MB)
Subscribe: Apple Podcasts
Written Summary & Blog post prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman November 2014
Cite this podcast as: Helman, A, Weingart, S, Himmel, W. Preoxygenation and Delayed Sequence Intubation. Emergency Medicine Cases. November, 2014. https://emergencymedicinecases.com/episode-54-weingart-himmel-sessions-preoxygenation-delayed-sequence-intubation/. Accessed [date].
Preoxygenation Strategies
Preoxygenation prior to intubation is required to de-nitrogenate the patient’s lungs and to prevent desaturation during the apneic period after induction and paralysis, and during intubation.
Traditionally with Rapid Sequence Intubation (RSI), the patient is pre-oxygenated for 3 minutes of tidal volume or 8 vital capacity breaths with a non-rebreather. This only supplies an FIO2 of approximately 60%.
Consider adding nasal prongs with 15L of supplemental oxygen to 15L of O2 through the non-breather to increase the FiO2 closer to 100%.
Elevate the head of the bed to 20-30 degrees to optimize gas exchange. This also helps improve visualization during intubation. If the patient is in spinal precautions, use the reverse trendelenberg position.
If the patient is still hypoxic with these maneuvers (O2 saturation <93%), consider adding positive pressure during preoxygenation. This can be done either with:
- A bag-valve-mask with a PEEP valve (see image), using a good mask seal over nasal prongs, or
- Placing the patient on CPAP, also leaving the nasal prongs on. Use up to a maximum of 15cm H2O to prevent opening the lower esophageal sphincter

Bag-valve-mask with PEEP valve attached
The Triple 15 Rule For Pre-oxygenation
Memory Aid Pearl: The Triple 15 Rule for preoxygenation – an easy way to remember how to maximize oxygen delivery during the pre-intubation phase
- 15L O2 by nasal prongs, plus
- 15L O2 by non-rebreather, and if oxygen saturation <95% then
- 15cm H2O of CPAP while maintaining nasal prongs (1)
Apneic Oxygenation
Apneic oxygenation: provides ongoing maximal oxygenation during the apneic period, immediately after induction and paralysis, and before intubation of the trachea with ventilation. Apneic oxygenation has been shown to increase the frequency and duration of higher oxygenation saturations during intubation (2,3).
Indications for Apneic Oxygenation:
- Patient who requires intubation, but is not predicted to crash imminently AND
- O2 saturation < 93%
Method to provide apneic oxygenation: leave nasal prongs at 15L/min on the patient during the apneic period. If the patient required positive pressure ventilation for preoxygenation, they will require CPAP for the apneic period as well. This is done by leaving the bag-mask-valve with the PEEP valve or the NIPPV CPAP mask on the patient, using a good mask seal.
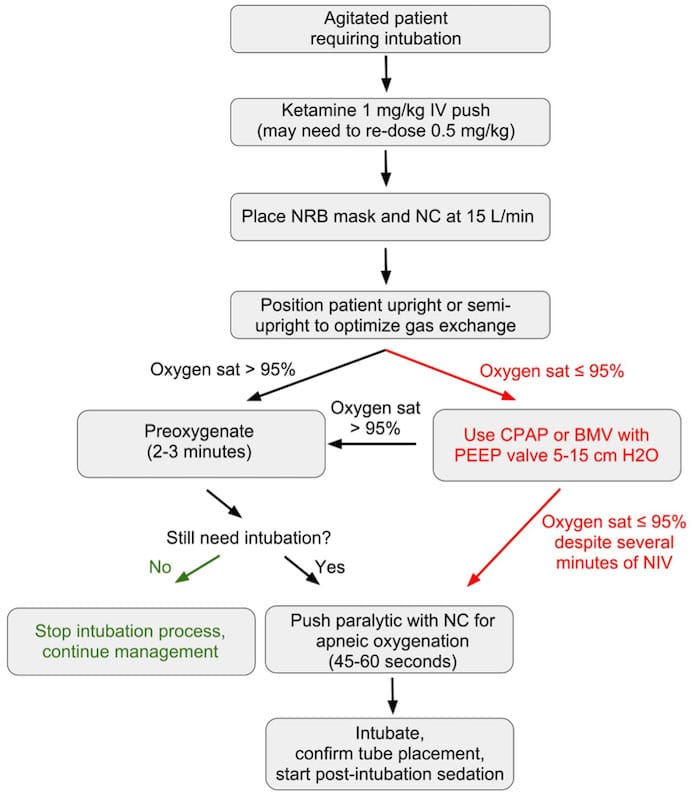
Delayed Sequence Intubation (DSI)
When to use DSI: Recommended by Dr. Weingart for the altered patient who is not cooperating with your attempts at securing the airway. For example, a patient with agitated delirium from hypoxia, hypercapnia, or the underlying medical condition.
DSI is Procedural Sedation With the Procedure Being Pre-oxygenation: DSI uses a dissociative dose of ketamine (1.0-1.5mg/kg IV) in a critically ill adult patient. Ketamine allows the clinician to provide pre-oxygenation to the patient as described as above. DSI allows calm, deliberate securing of the airway in an otherwise uncontrollable patient and as such can be conceptualized as procedural sedation for airway intubation, with the procedure being pre-oxygenation.
Once the patient is dissociated:
- Place the patient on oxygen with 15L nasal prongs and either 15cm H2O via BVM plus peep valve or via CPAP
- When the O2 saturation is >95% allow the patient to breathe for 3 minutes
- Then administer the paralytic if required and leave the mask and nasal prongs on while the paralytic takes effect
- When ready for intubation, remove the face mask, leaving the nasal prongs in place and intubate (See the DSI Algorithm in Figure 1)
A recent multicentered study was conducted on 62 patients who required DSI for preoxygenation secondary to delirium (4).
- The primary outcome in this study was oxygenation saturation after maximal attempts at preoxygenation before DSI vs. saturation prior to intubation with DSI
- No complications were observed in patients receiving DSI.
- All patients increased their oxygen saturations post-DSI, with 91% of patients increasing their O2 saturation post-DSI to greater than 93%
- 2 patients avoided intubation post-DSI
![]() Update 2023: A randomized controlled trial including 200 critically injured patients requiring definitive airway management found that the use of delayed sequence intubation (dissociative dose of ketamine followed by 3 minutes of preoxygenation) compared to conventional rapid sequence intubation found that DSI was associated with significantly lower peri-intubation hypoxia (8% vs 35%, P=0.001), higher first-attempt success rate (83% vs 69%, P=0.01), with no incidence of hemodynamic instability or statistically significant difference in airway related adverse events. Abstract
Update 2023: A randomized controlled trial including 200 critically injured patients requiring definitive airway management found that the use of delayed sequence intubation (dissociative dose of ketamine followed by 3 minutes of preoxygenation) compared to conventional rapid sequence intubation found that DSI was associated with significantly lower peri-intubation hypoxia (8% vs 35%, P=0.001), higher first-attempt success rate (83% vs 69%, P=0.01), with no incidence of hemodynamic instability or statistically significant difference in airway related adverse events. Abstract
Delayed Sequence Intubation Algorithm
With permission Michelle Lin Academic Life in EM
More Pre-oxygenation concepts, innovations and pearls
Minh Le Cong on novel approach to pre-oxygenation at PHARM blog
Article on Safety of high flow nasal cannula
Weingart’s podcast on Oxygen Physiology
More on Delayed Sequence Intubation
Weingart’s deep dive into Delayed Sequence Intubation at EMcrit.
The Bottom Line’s analysis of Weingart’s latest article on DSI
![]() More on airway management on EM Cases:
More on airway management on EM Cases:
Episode 8: Emergency Airway Controversies
Episode 55: Fluids in Sepsis, Post-intubation Analgesia and Sedation
Dr. Helman, Dr. Weingart & Dr. Himmel have no conflicts of interest to declare.
![]() Update 2021: Multi-center ED and ICU randomized control trial assessing “first pass” intubation success rate with either bougie first (n=566) or endotracheal tube (ETT) and stylet (n=546). No difference between both groups in first pass success rate across mix of providers (residents, ED attendings, and ICU). Abstract
Update 2021: Multi-center ED and ICU randomized control trial assessing “first pass” intubation success rate with either bougie first (n=566) or endotracheal tube (ETT) and stylet (n=546). No difference between both groups in first pass success rate across mix of providers (residents, ED attendings, and ICU). Abstract
Key References
- Weingart, SD & Levitan, RM. 2012. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med, 59(3): 165-75. Full article
- Ramachandran, SK, Cosnowski, A, Shanks, A & Turner, CR. 2010. Apneic oxygenation during prolonged laryngoscopy in obese patients: A randomized, controlled trial of nasal oxygen administration. J Clin Anesth, 22(3): 164-8. Full article
- Christodoulou, C, Mullen, T, Tran, T, Rohald, P, Hiebert, B & Sharma, S. 2013. Apneic oxygenation via nasal prongs at 10L/min prevents hypoxemia during elective tracheal intubation. Chest, 144(4- Meeting Abstracts): 890A.
- Weingart, SD, Trueger, NS, Wong, N, Scofi, J, Singh, N & Rudolph, SS. In Press. Delayed Sequence Intubation: A prospective observational study. Ann Emerg Med. Full pdf


{kind=link}
[…] study. Ann Emerg Med. 2015; 65: (4), 349-355. EMCrit’s Everything About DSI Chart’s with DSI Algorithims and Podcast Links EMRAP June 2014’s highlight on DSI Feel free to bring up any additional sources […]