

In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. Can you identify which were early repolarization and which were anterior STEMI?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman, October 2019
The following patients presented with potentially ischemic symptoms and mild anterior ST elevation…
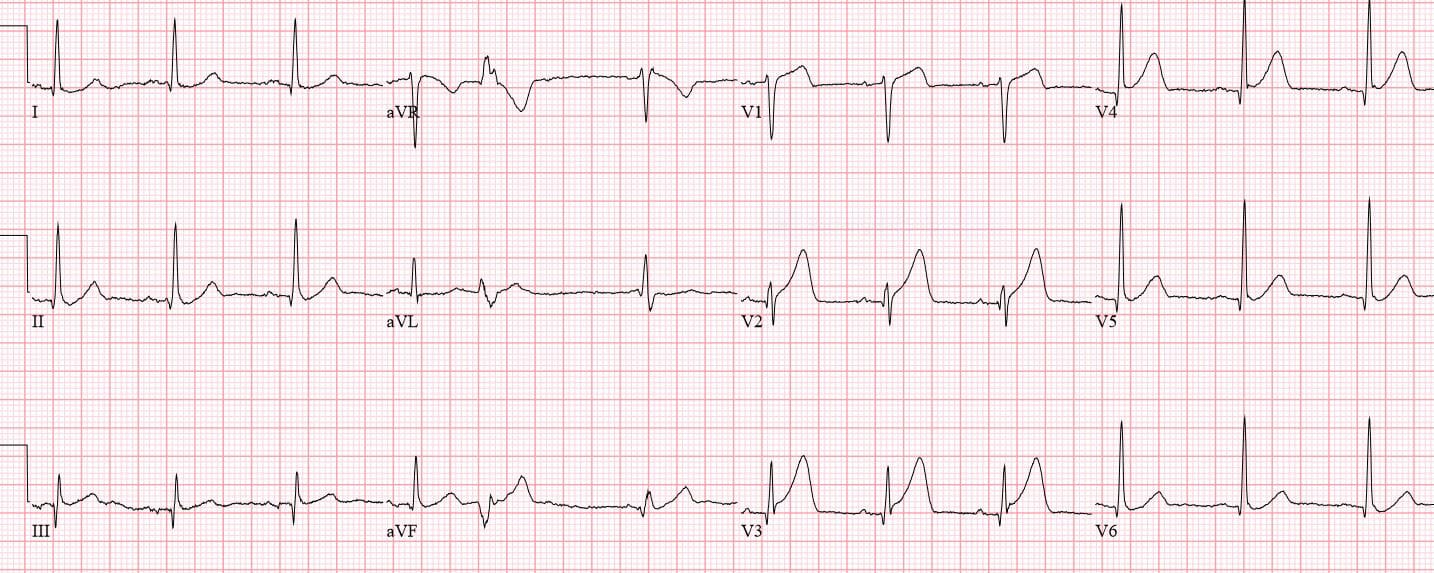
Patient 1: 30yo smoker with chest pain radiating to the arm

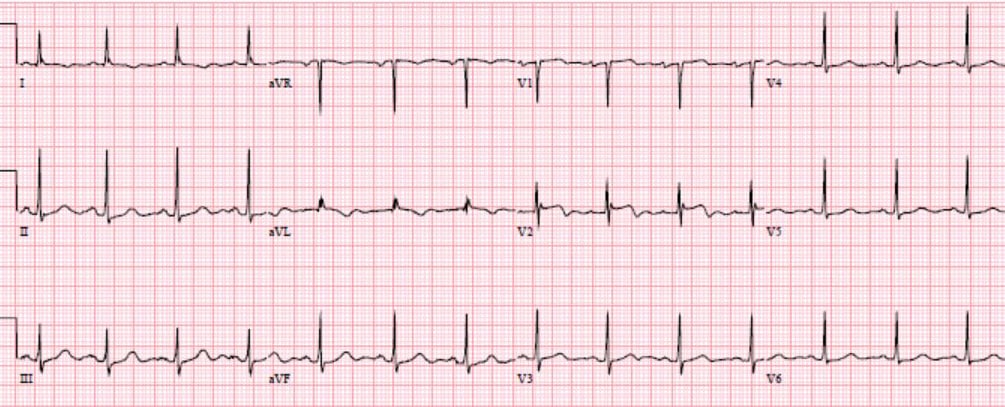
Patient 2: 55yo with chest pain and diaphoresis, computer interpretation “early repolarization”
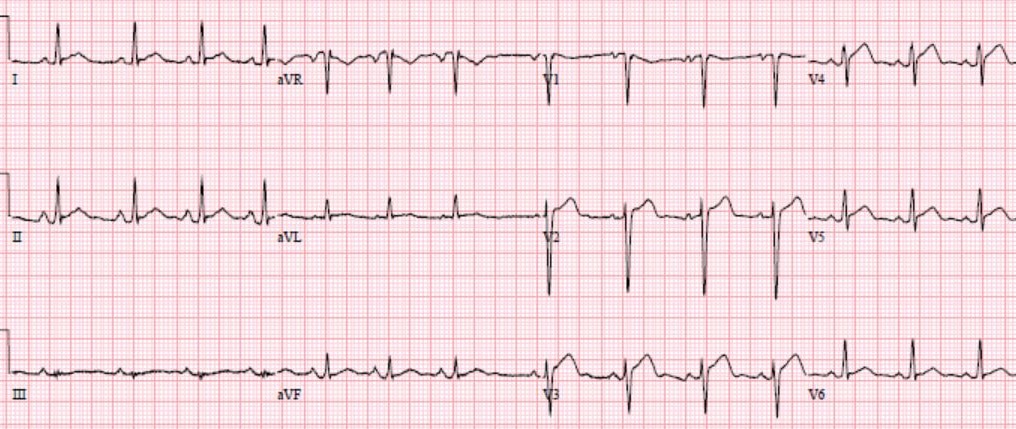
Patient 3: 70yo with 2 hours of chest pain, computer interpretation “nonspecific”

Patient 4: 60yo with 1hr CP radiating to jaw, with SOB. Computer interpretation “early repolarization”
Patient 5: 50yo with epigastric pain. Computer interpretation “pericarditis”
Patient 6: 70yo with 6hrs on/off chest tightness radiating to the arm, now constant. Old then new ECG, both labelled “normal”
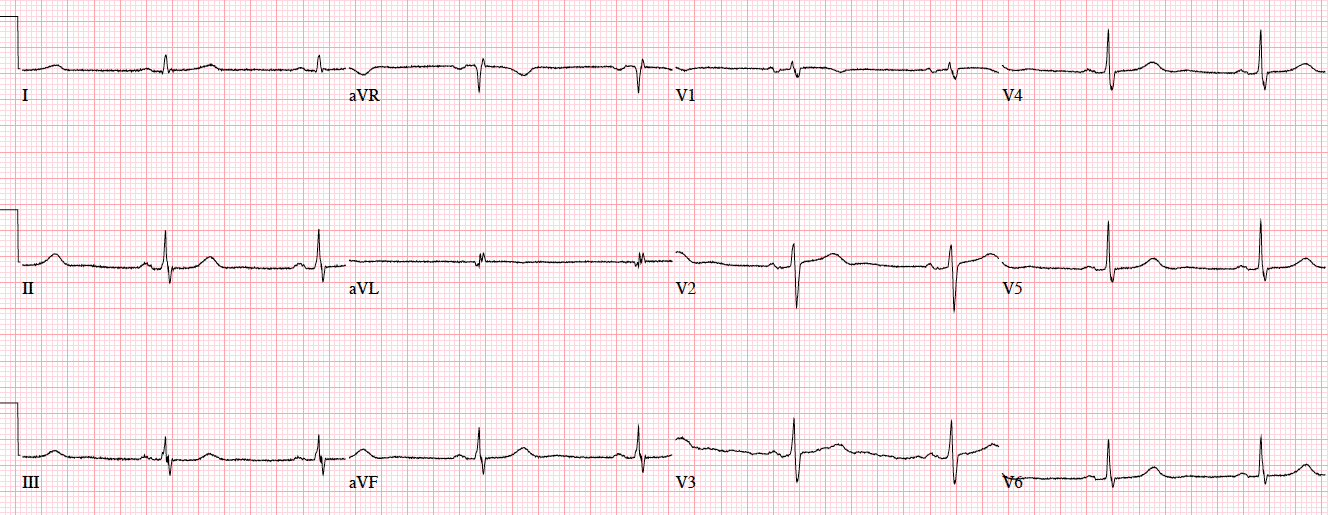
Patient 7: 60yo with syncope, weakness, “STEMI” with EMS
Early repolarization vs anterior STEMI
According to the latest guidelines, anterior STEMI is diagnosed when there is new ST elevation at the J point in two contiguous anterior leads of 1mm, except for V2-3 which need 1.5mm in women, 2mm in men 40 and older, and 2.5mm in men <40. But this is neither sensitive nor specific for the underlying pathology it is meant to diagnose: occlusion of the left anterior descending (LAD) coronary artery. Neither ST amplitude nor morphology reliably differentiate between LAD occlusion and early repolarization. As Stephen Smith explained,
“The 2 entities may be difficult to distinguish from each other for several reasons. First, upward ST-segment concavity, usually associated with normal ECG results, is also present in 30% to 40% of anterior STEMI (due to left anterior descending artery occlusion), especially early after onset of symptoms. Moreover, 30% to 40% of anterior STEMIs have borderline ST-segment elevation (absence of 2 consecutive leads with at least 2mm of ST-segment elevation), and 20% may have upward concavity and borderline ST-segment elevation. Conversely, most benign ECGs have at least 1mm of ST-segment elevation in right precordial leads.” [1]
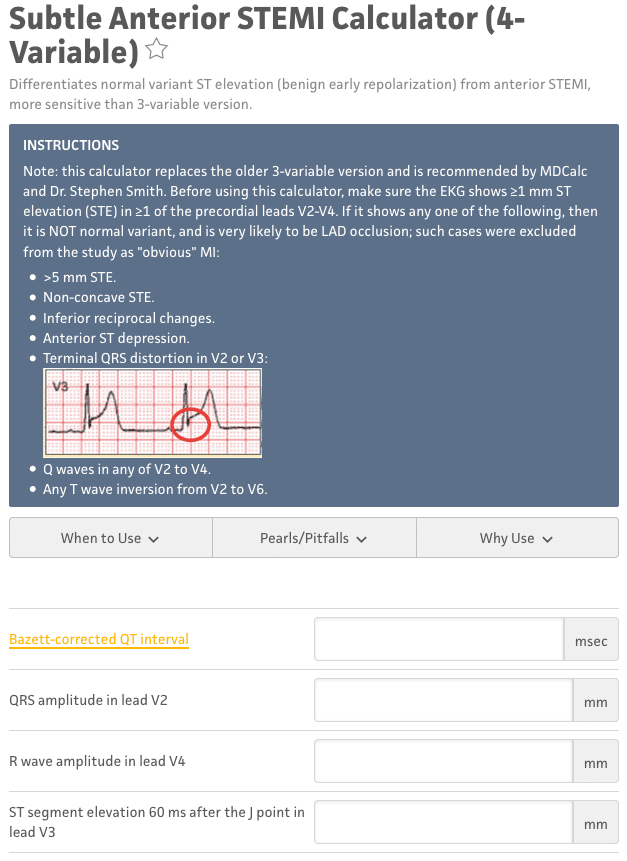
Dr. Smith has developed a formula for differentiating early repolarization from subtle LAD occlusion, in cases where there is at least 1mm of STE in at least 1 anterior lead. It examines ST elevation relative to the QRS complex (higher in early repolarization) and QT interval (shorter in early repolarization).[2] It is available on MD-calc, and begins with important BER exclusion criteria:
Back to the cases for early repolarization or anterior STEMI?
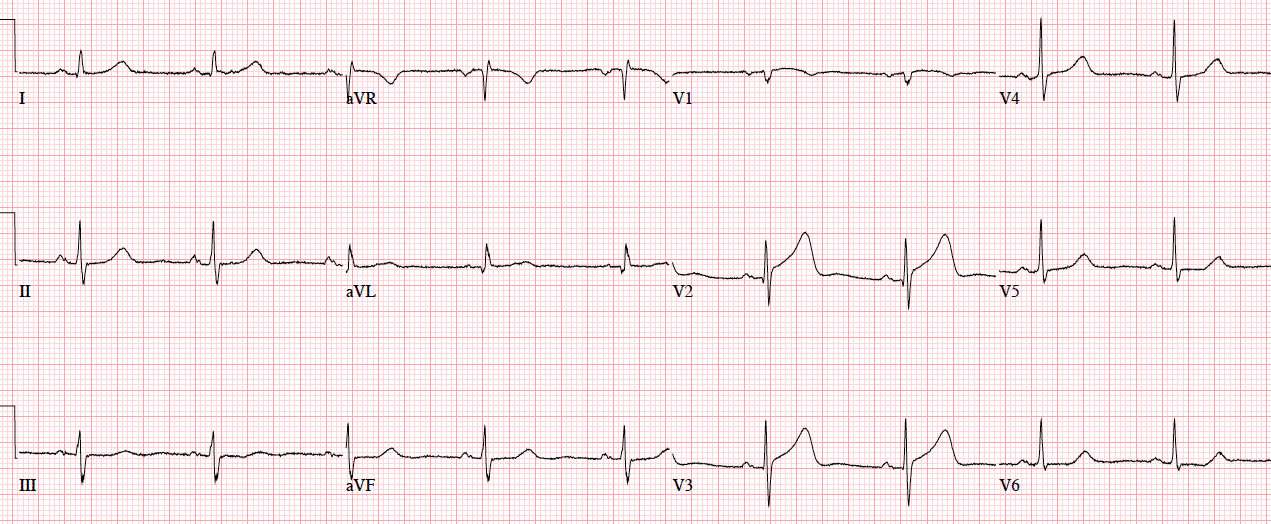
Patient 1: anterior Q wave
NSR, normal conduction/axis, no hypertrophy. Concave ST elevation V2-4 without reciprocal change, which was assumed to be from early repolarization because of the patient’s young age. But V2-3 have Q waves and total loss of R waves. (While Q waves can be seen in old MI, V3 has T/QRS > 0.36, which differentiates anterior STEMI from LV aneurysm [3]; more cases on this in a subsequent post). When trop came back at 3,000 cath lab was activated: 95% mid-LAD occlusion. Discharge ECG shows LV aneurysm morphology with T/QRS < 0.36.
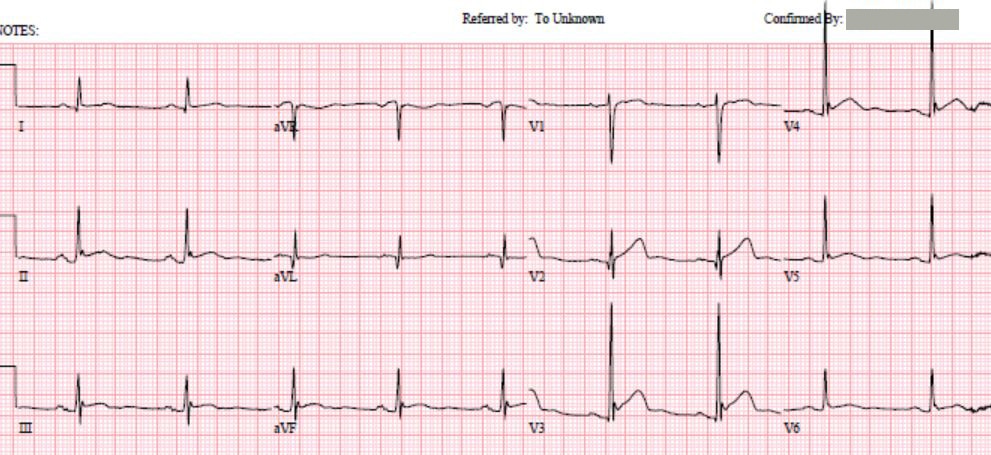
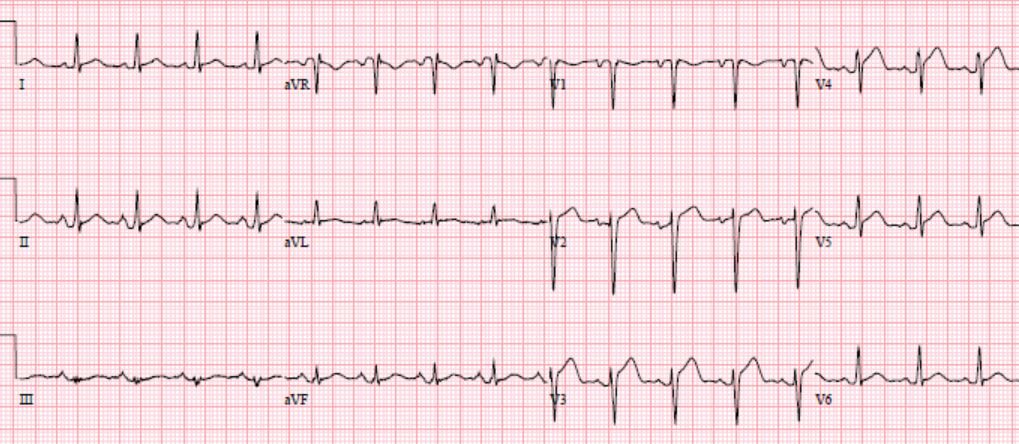
Patient 2: terminal QRS distortion
NSR with PVC, normal conduction/axis/R wave, no hypertrophy. Mild concave ST elevation v1-3 interpreted by the computer as early repolarization, but there are two exclusion criteria: Q waves in V2-3, and terminal QRS distortion in V3. There are also hyperacute T waves (larger than the preceding QRS complex) in V2-3. Physician was concerned about acute coronary occlusion so treated patient with antiplatelets and nitro. Repeat ECG still had no significant ST elevation but but pain continued despite IV nitro so cath lab was activated: 100% proximal LAD occlusion.
Patient 3: convex ST segments
NSR, normal conduction/axis/R wave, no hypertrophy. Mild ST elevation V2-4 but it is convex in V3-4, with some terminal T wave inversion. Cath lab activated: 100% LAD occlusion.
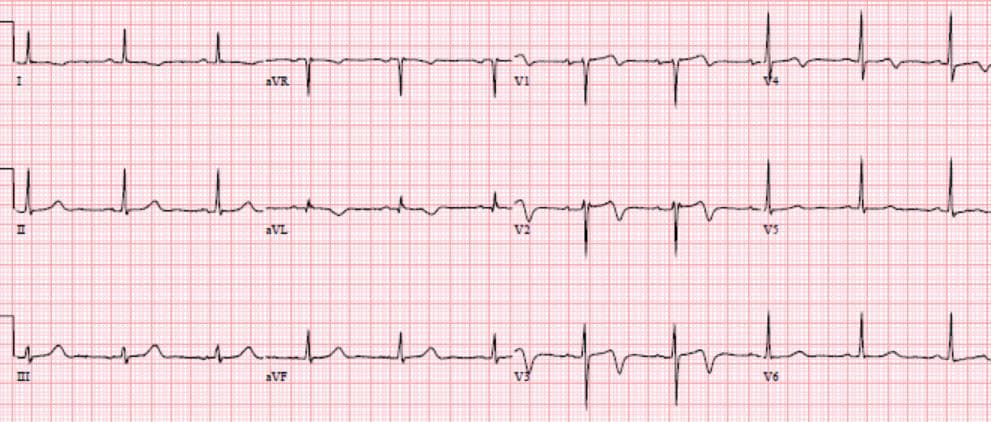
Patient 4: T wave inversion and reciprocal change
NSR, normal conduction/axis, R wave, no hypertrophy. Concave ST elevation in V2 only, and referred to cardiology as NSTEMI when trop came back at 400. But there is T wave inversion in V2 (as wellas I/aVL), and mild reciprocal ST depression inferolaterally. Cath lab: 95% LAD occlusion. Discharge ECG has reperfusion T waves anteriorly, and resolution of ST depression inferolaterally:
Patient 5: subtle LAD occlusion
NSR, normal conduction/axis. Delayed R wave progression, no hypertrophy. Mild ST elevation V2-4, which is almost straight in V3-4 with bulky T waves. Formula gives 21.7 = likely LAD occlusion. Repeat ECG had straightening of ST segments in V2, physician saw apical hypokinesis on POCUS and activated the cath lab: LAD occlusion
Patient 6: subtle LAD occlusion
NSR, normal conduction/axis/Rwave, no hypertrophy. Compared with the old ECG there’s a tiny Q wave in V2, mild ST elevation V2-3 with hyperacute T waves, and mild ST depression in V6. Smith formula 20.4 = likely anterior STEMI. When trop came back positive cath lab was activated: 100% LAD occlusion.
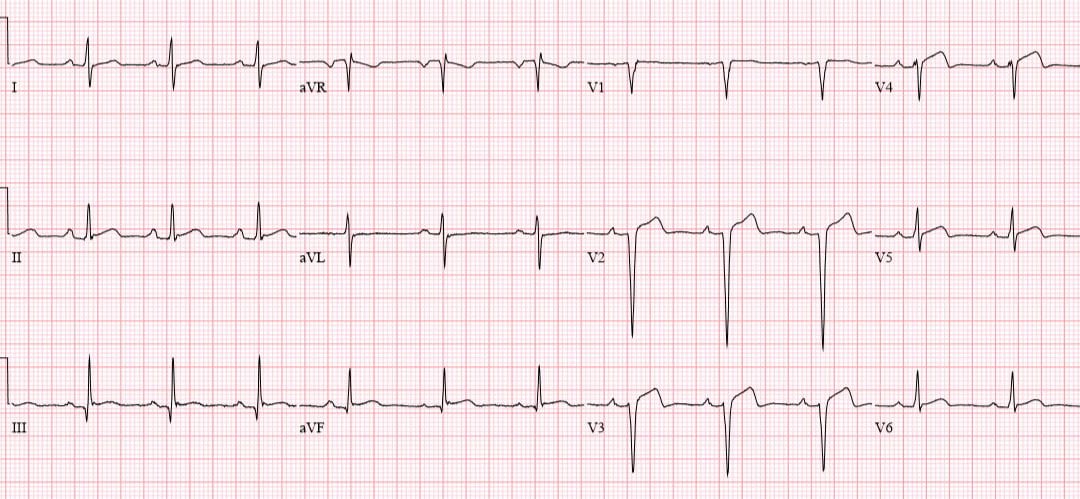
Patient 7: early repolarization
NSR, normal conduction/axis/, early R-wave, no hypertrophy. There is a tiny Q wave in V2, but no other exclusion criteria (there is no S wave in V3 but there is a J wave, so no terminal QRS distortion). Mild ST elevation V2-3, but a short QT interval and very high voltage in V4 give a Smith formula of 16.5 = likely early repolarization. Serial ECG no change and serial troponins negative.
Take home points for early repolarization or anterior STEMI?
- LAD occlusion can have mild concave ST elevation that doesn’t meet STEMI criteria and that will be missed by automated interpretation–and labelled anything from “early repolarization” or “pericarditis” to “nonspecific” or even “normal“
- Early repolarization exclusion criteria and other signs of ischemia like hyperacute T waves or dynamic changes can identify LAD occlusion
- In subtle cases the Smith formula can help differentiate between early repolarization and LAD occlusion
References for Early repolarization or anterior STEMI
- Smith SW, Khalil A, Henry TD, et al. Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardial infarction. Ann Emerg Med. 2012;60(1):45-56.e2.
- Driver BE, Khalil A, Henry T, Kazmi F, Adil A, Smith SW. A new 4-variable formula to differentiate normal variant ST segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion – Adding QRS amplitude of V2 improves the model. J Electrocardiol. 2017;50(5):561-569.
- Klein LR, Shroff GR, Beeman W, Smith SW. Electrocardiographic criteria to differentiate acute anterior ST-elevation myocardial infarction from left ventricular aneurysm. Am J Emerg Med. 2015;33(6):786-90.



Great cases – thanks!!
[…] ST/T waves: no change in ST segment amplitude but there is T wave inversion in V2 (and I/aVL) and inferior ST depression, which are exclusion criteria for early repolarization […]