

Topics in this EM Quick Hits podcast
Justin Morgenstern on the lack of evidence for burn debridement (0:30)
Jesse MacLaren on ECG Cases – missed ischemia and pitfalls of “normal” computer ECG interpretations (5:20)
Arun Sayal on clinical diagnosis pitfalls of compartment syndrome (9:24)
Sarah Reid on pediatric asthma pitfalls and myths (16:15)
Andrew Petrosoniak on T-spine and L-spine fracture work-up (24:12)
Michelle Klaiman & Taryn Lloyd on motivational interviewing part 2 (32:06)
Podcast: Play in new window | Download (Duration: 39:03 — 35.8MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content & blog post by Justin Morgenstern, Jesse MacLaren, Arun Sayal, Sarah Reid,
Andrew Petrosoniak, Michelle Klaiman & Taryn Lloyd and Anton Helman
Cite this podcast as: Helman, A., Morgenstern, J., MacLaren, J., Sayal, A., Reid, S., Petrosoniak, A., Klaiman, M., Lloyd, T. EM Quick Hits 9 – Burn Blister Debridement, ECG Cases, Compartment Syndrome, Pediatric Asthma, Spinal Trauma & Motivational Interviewing. October, 2019. https://emergencymedicinecases.com/em-quick-hits-october-2019/. Accessed [date].
Is there evidence for burn blister debridement?
- There is little, if any evidence that burn blister debridement is beneficial to healing or burns despite most burn surgeons advocating for debridement of blisters more than 2cm in diameter.
- Since there is no evidence of benefit, we must consider the other impacts of debridement: the added pain it causes, and the potential problems with departmental flow as patients wait for (potentially unnecessary) procedural sedation.
Forage AV. The effects of removing the epidermis from burnt skin. Lancet (London, England). 1962; 2(7258):690-3.
Gimbel NS, et al. A study of epithelization in blistered burns. A.M.A. archives of surgery. 1957; 74(5):800-3.
Ro HS, Shin JY, Sabbagh MD, Roh SG, Chang SC, Lee NH. Effectiveness of aspiration or deroofing for blister management in patients with burns: A prospective randomized controlled trial. Medicine. 2018; 97(17):e0563.
Swain AH, Berge SA, Wakeley CJ et al. Management of blisters in minor burns. Br Med J (Clin Res Ed). 1987;295:181.
https://first10em.com/should-i-debride-burn-blisters/
Missed ischemia with “normal” ECG computer interpretation
Never trust the ECG computer interpretation, even if it says “normal,” because:
- Ischemic morphology: the computer focuses on ST segment elevation, and can miss ischemic ST-T wave morphology—including straight or convex ST segments, terminal T wave inversion, down-up T waves, hyperacute T waves, deWinter T waves, and inverted U waves
- Dynamic change: the computer interprets each ECG in isolation, and can’t compare to prior or repeat ECGs (which is critical in a dynamic process like coronary occlusion)—so it can miss subtle changes, including pseudonormalization of ST segments or T waves
- STEMI criteria: computer interpretation is based on STEMI criteria, which has limited sensitivity for identifying acute coronary occlusion—so it can miss subtle ST elevation (which may be significant in small amplitude QRS complexes), ST depression in aVL (which is very sensitive for inferior MI), and subtle signs of LAD occlusion like terminal QRS distortion.
Test your ECG interpretation skills for ischemia on ECG Cases #1 Missed Ischemia
- Schläpfer J, Wellens HJ. Computer-Interpreted Electrocardiograms: Benefits and Limitations. J Am Coll Cardiol. 2017;70(9):1183-1192.
- Hughes KE, Lewis SM, Katz L, Jones J. Safety of Computer Interpretation of Normal Triage Electrocardiograms. Acad Emerg Med. 2017;24(1):120-124.
- Litell JM, Meyers HP, Smith SW. Emergency physicians should be shown all triage ECGs, even those with a computer interpretation of “Normal”. J Electrocardiol. 2019;54:79-81.
- ECG Cases blog https://emergencymedicinecases.com/ecg-cases-computer-interpretation-ischemia/
Compartment syndrome clinical pitfalls
- Do not rely on the presence of a fracture to suspect the possibility of compartment syndrome; 30% of compartment syndromes.are due to injuries that do not involve fractures, such as high pressure injection injuries, tight casts and dressings, soft tissue injuries, burns, extravasation of IV fluids.
- Do not dismiss the possibility of compartment syndrome in the setting of an open fracture.
- Do not dismiss the possibility of compartment syndrome when pain is the only finding; of the 6 Ps (Pain, Paresthesias, Paralysis, Pulselessness, Palor, Poikilothermia), all except pain are often not present when patients initially present to the ED.
- Pain out of proportion, especially with passive stretch of the compartment, in addition to a palpable tight/tender compartment is enough to suspect the diagnosis
- Measurement of compartment pressures using a Stryker needle are inaccurate and may be misleading in the diagnosis of compartment syndrome; measurement of compartment pressure should not be a prerequisite for consulting orthopedic surgery for a suspected compartment syndrome
- Lor KKH, Yeoh NCS, Wong KP, Wee ATH. Raised compartment pressures are frequently observed with tibial shaft fractures despite the absence of compartment syndrome: A prospective cohort study. J Orthop Surg (Hong Kong). 2017;25(2):2309499017717362.
- Heckman MM, Whitesides TE, Grewe SR, Rooks MD. Compartment pressure in association with closed tibial fractures. The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am. 1994;76(9):1285-92.
- McQueen MM, Duckworth AD. The diagnosis of acute compartment syndrome: a review. Eur J Trauma Emerg Surg. 2014 Oct;40(5):521-8.
Pediatric asthma: 5 pitfalls and myths
- Diagnose asthma in preschoolers. Preschool children have the highest rate of emergency department visits and hospital admissions for asthma-like symptoms. ≥ 2 episodes (Obstruction + Reversibility) = Asthma
- Use the Pediatric Respiratory Assessment Measure (PRAM) to standardize your assessment of asthma severity.
- Give a systemic steroid to all children with moderate/severe asthma exacerbations within the first hour of treatment. Dexamethasone 0.6 mg/kg (MAX 12 mg/dose) x 2 days. Treatment with systemic steroids within first hour of presentation in ED reduces time to improvement, reduces time to discharge, reduces admission rates by 25%.
- Send children home with a prescription for an inhaled corticosteroid if they have had a moderate/severe exacerbation (i.e. they needed an oral steroid) or if they have frequent chronic symptoms (≥2 days/week and/or ≥8 days/month). A therapeutic trial of a moderate dose inhaled corticosteroid means 3 months minimum.Onset of action of inhaled corticosteroids is 1-4 weeks, so prn use is ineffective.
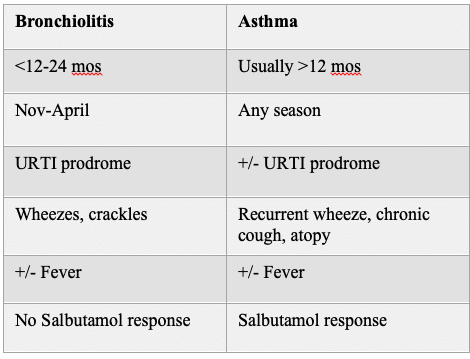
- Distinguishing asthma from bronchiolitis
- Canadian Pediatric Society Position Statement on Asthma in Preschoolers: https://www.cps.ca/documents/position/asthma-in-preschoolers
- Ducharme FM, Chalut D, Plotnick L, Savdie C, Kudirka D, Zhang X, Meng L, McGillvary D. The pediatric respiratory assessment measure: A valid clinical score for assessing acute asthma severity from toddlers to teenagers. J Pediatr. 2008 Apr; 152(4):476-80.
- Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2000;(2):CD002178.
- Keeney GE et al. Dexamethasone for acute asthma exacerbations in children: A meta-analysis. Pediatrics. 2014 Mar 1;133(3):493-9.
T-spine and L-spine fracture ED work-up
- Neurologic complications/deterioration are 8 times more likely in T-spine and L-spine fractures that are missed or delayed
- Mechanism of injury overall has not been shown to be predictive of T-spine and L-spine fractures, however the following high risk features have been found to be associated: fall from a height of >5 stairs or 3-4ft, crush injury, MVC roll-over, unenclosed vehicle crash, pedestrian struck by vehicle
- The only physical exam feature that is predictive of a T-spine or L-spine fracture is a palpable deformity; physical exam alone is insufficient to rule out a T-spine/L-spine injury; the -LR for spinous process tenderness is only 0.57 which is not enough to rule out a T/L-spine fracture in its absence.
- Threshold for imaging should be lower in patients with altered level of awareness, distracting injuries and age >60 years
- If imaging the chest and abdomen for a different indication it is reasonable to add T/L-spine reformats as the radiation and time to image is unchanged
- CT is the test of choice for suspected T/L-spine trauma; the test characteristics of x-ray for T/L spine fractures are poor
- For compression fractures found on x-ray >40% of the height of the vertebrae, follow-up CT is indicated
Bottom Line: Your decision making should incorporate whether the patient is evaluable, has any clinical exam findings, a high risk mechanism, age >60 or distracting injuries. Together, use these features to guide your decision making. It’s really the best we have!
- Inaba et al. Prospective derivation of a clinical decision rule for thoracolumbar spine evaluation after blunt trauma: An American Association for the Surgery of Trauma Multi-Institutional Trials Group Study. J Trauma Acute Care Surg 2015; 78(3): 459-467.
- Karul et al. Fractures of the thoracic spine in patients with minor trauma: Comparison of diagnostic accuracy and dose of biplane radiography and MDCT. Euro J Radiol 2013; 82: 1273-1277.
- Inaba et al. Clinical examination is insufficient to rule out thoracolumbar spine injuries. J Trauma 2011; 70 (1): 174-179.
- Vandenberg et al. Blunt thoracolumbar-spine trauma evaluation in the emergency department: a meta-analysis of diagnostic accuracy for history, physical examination, and imaging. J Emerg Med 2019; 56(2): 153-165.
Motivational interviewing part 2
Motivational interviewing uses three communication styles: asking, listening and informing.
1.Asking. Use DARN to help generate questions and illicit change talk:
Desire: “What do you want, like, wish, hope?
Ability: “What is possible? What could you do? What are you able to do?”
Reasons: “Why would you make this change? What would be some benefits? What negative outcome or risk would you like to decrease?”
Need: “How important is this change?”
2.Listening. Let the patient know you are listening, hearing and understanding them by providing short summaries. Offer them as statements rather as questions. This encourages patients to continue taking.
“You are worried alcohol is affecting your health”
“You feel trapped”
“This is really important to you”
3.Informing. While our job is often to inform, you can do so within in the framework of motivational interviewing:
- Ask for permission
- Offer several choices
- Talk about that others do
- Check in to make sure the patient understands “ What do you make of that? What does that mean for you? What more would you like to know?”
- Hall, Kate & Gibbie, Tania & Lubman, Dan. (2012). Motivational interviewing techniques: Facilitating behaviour change in the general practice setting. Australian family physician. 41. 660-7.
- Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change. New York: The Guilford Press.
- Miller, W. R., & Rollnick, S. (2008). Motivational interviewing in health care. New York: The Guilford Press.
- Rosengren, D. B. (2018). Building motivational interviewing skills: A practitioner workbook. New York: The Guilford Press.
None of the authors have any conflicts of interest to declare



Thank you Justin for your quick hit on burn blister debridement. I LOVE that you are so passionate about the evidence behind what we do. I completely agree the evidence supporting debridement of burns is not great. When evidence is lacking on a topic we generally turn to experience and expert opinion for guidance. The current opionion of burn experts is in strong support of debridement. For the majority of burns this is in fact a straight forward procedure in the ED and takes much less time than a reduction or complex lac repair (burns requiring same day transfer obviously don’t need to be debrided by us). I often just use IN fentanyl (doesn’t require monitoring) on top of po NSAIDs/acetaminophen with great results.
Thank you for this great resource. I am an EM physician in Groningen, The Netherlands. I listen to ur program while biking to and from work. It helped me in my practice a lot.