
In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Which had acute coronary occlusion? Introducing the concept of Occlusion MI – a paradigm shift in ECG diagnosis of MI…
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. December 2019
Seven patients presented with potentially ischemic symptoms. Which ones had acute coronary occlusion?
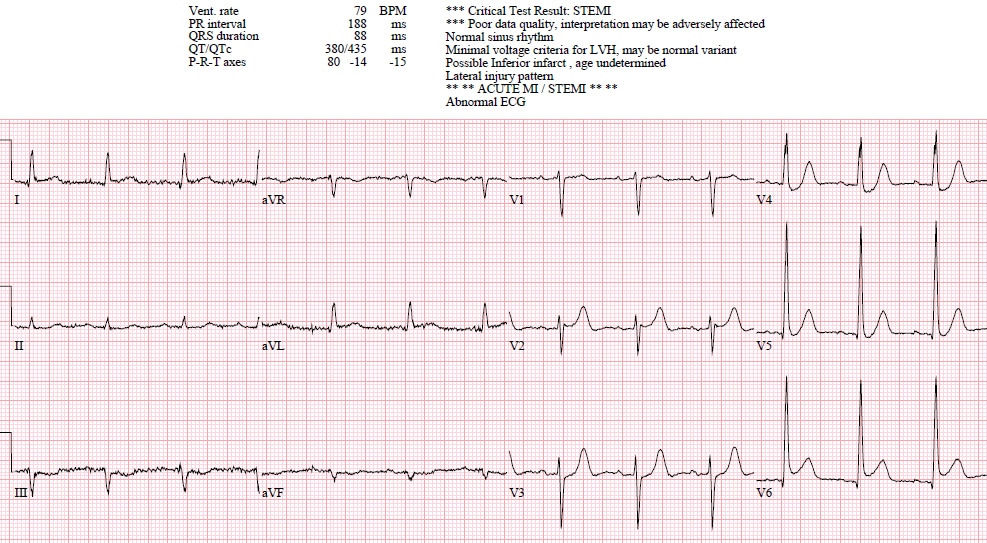
Patient 1: 50yo with one hour chest pain and nausea, serial ECGs:
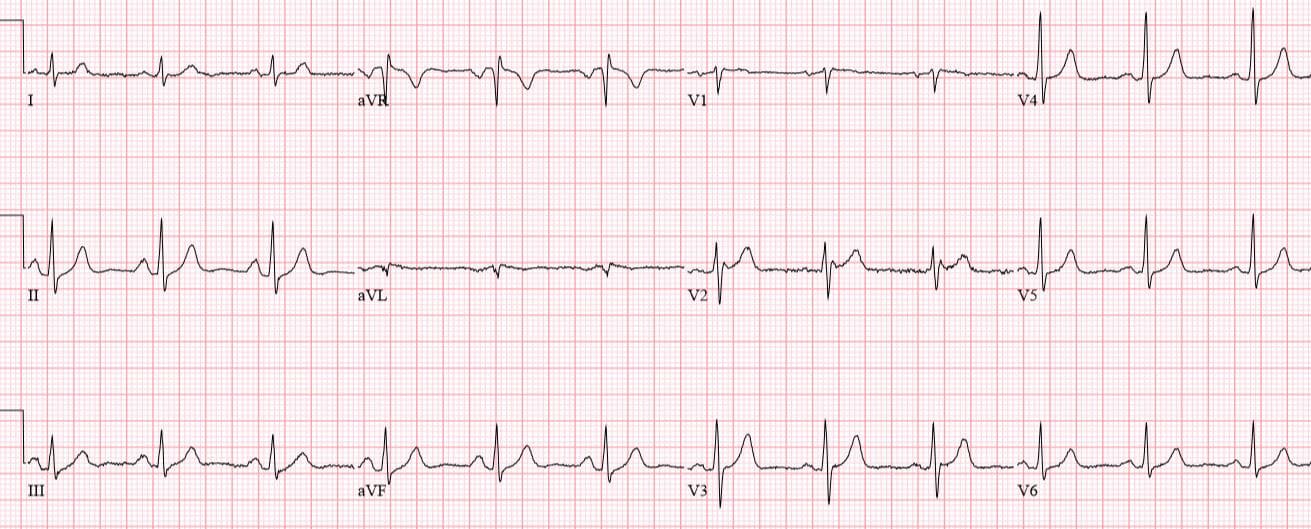
Patient 2: 70yo with 12 hours of non-exertional chest pain
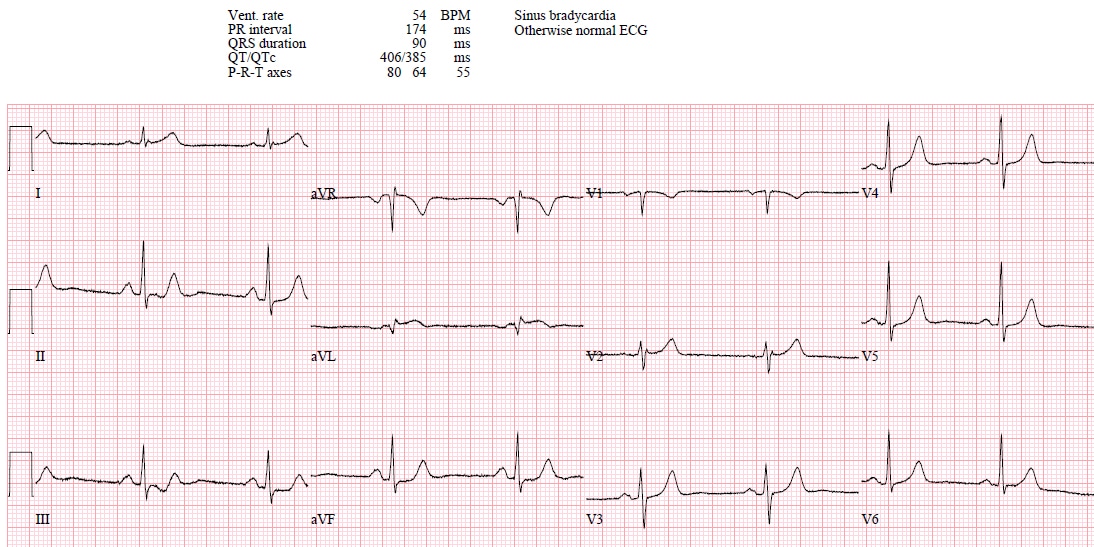
Patient 3: 40yo with one hour chest pain, shortness of breath and diaphoresis. Serial ECGs:
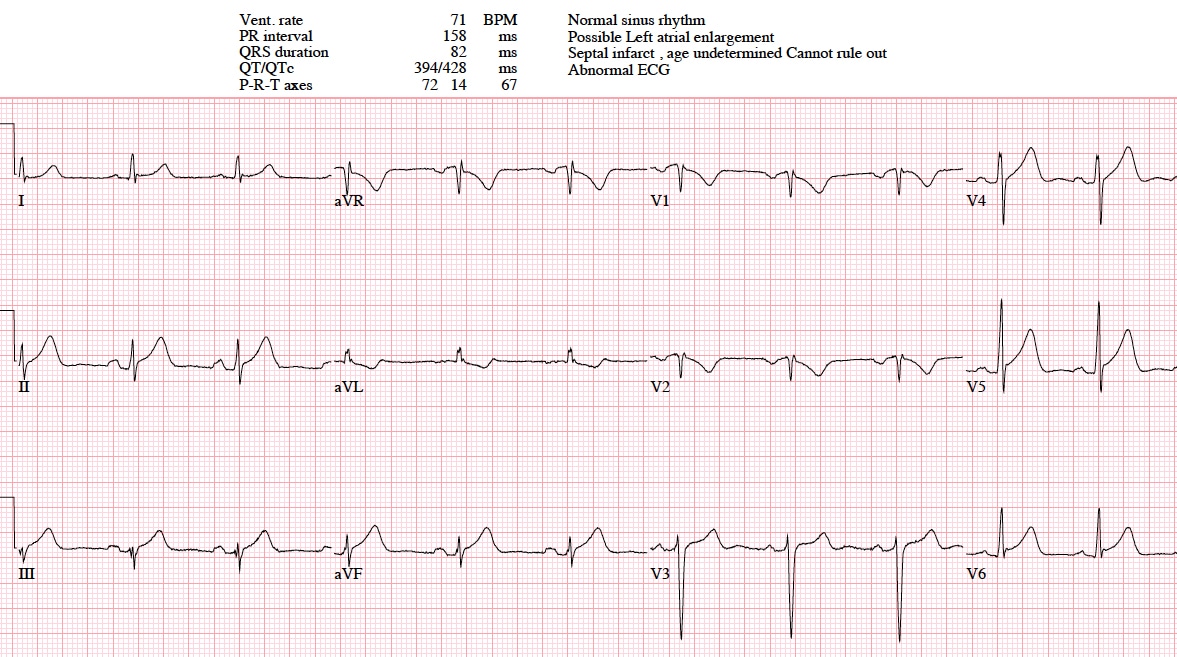
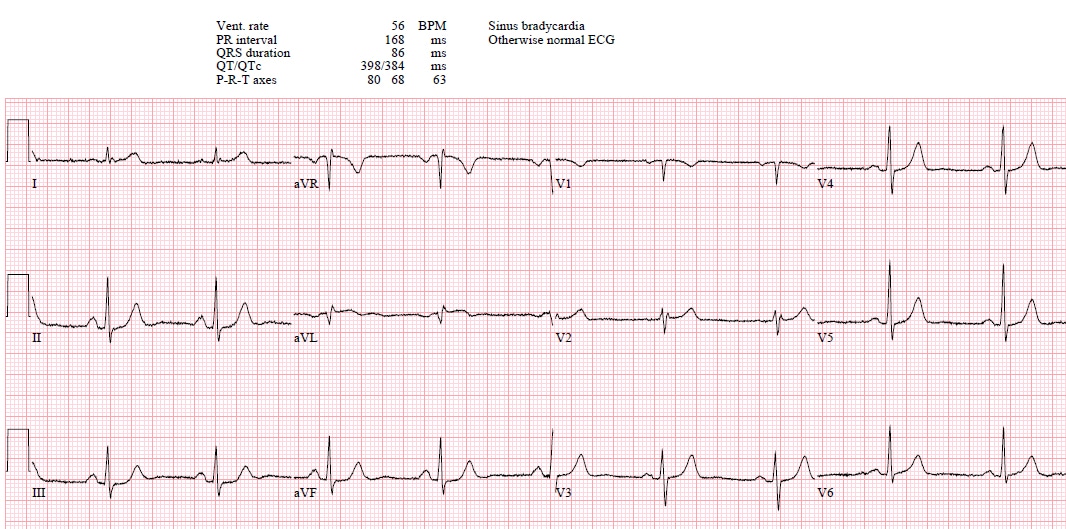
Patient 4: 55yo with one hour of chest pain. Old then new ECG
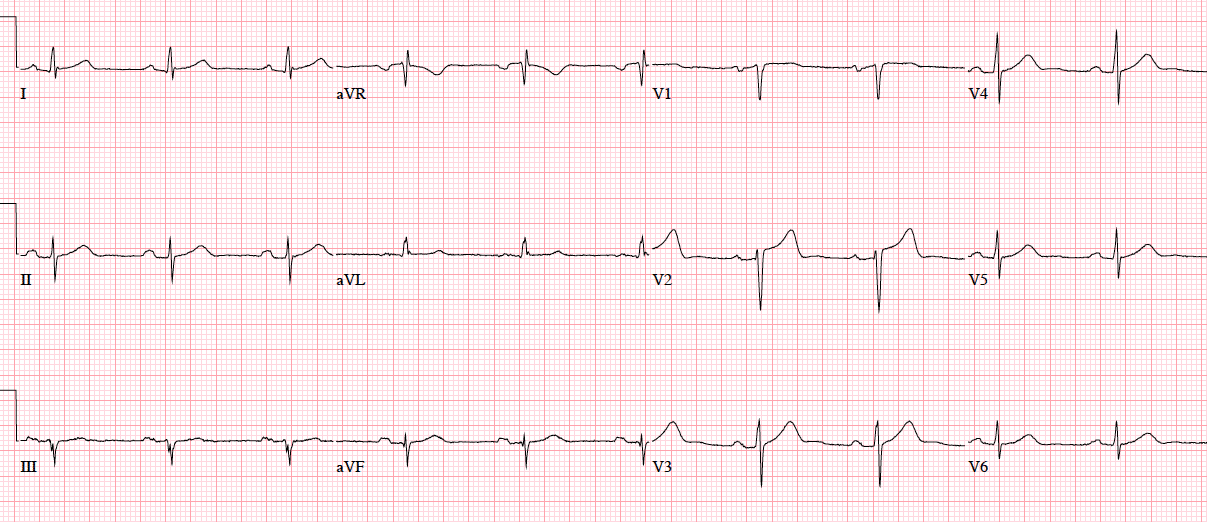
Patient 5: 85yo with one hour of chest pain radiating to the arm
Patient 6: 75yo with two days chest pain radiating to the shoulders, now constant for 90 minutes. Old ECG then serial ECGs:
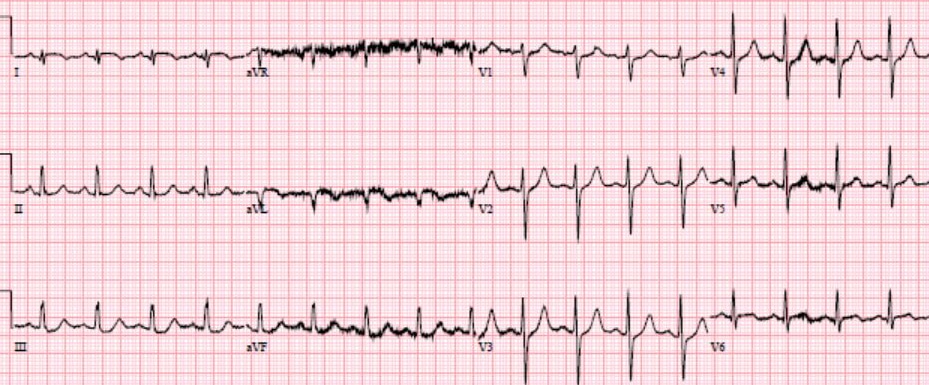
Patient 7: 40yo with 12 hours of chest pain and shortness of breath, began on exertion and refractory to nitro

Lateral STEMI vs Occlusion MI
The left ventricular lateral wall (represented by leads I, AVL, V5-6), is supplied by the diagonal branches of the left anterior descending artery and the circumflex artery and its branches. Depending on the vessel, acute coronary occlusion can be anterolateral (LAD), posterolateral +/- inferior (circumflex), or isolated lateral (LAD diagonal branch or circumflex obtuse marginal branch).
But the lateral wall is relatively electrocardiographically silent, so acute coronary occlusion can be subtle. Lateral STEMI criteria requires at least 1mm of ST elevation in at least two contiguous lateral leads; those not meeting this threshold are designated as NSTEMI and receive delayed reperfusion. But in a study of more than 500 patients with persisting ischemic symptoms and any amount of ST elevation, 18% of acute coronary occlusions had less than 1mm of ST elevation (including 35% of circumflex occlusions), though they had the same mortality rates. But two-thirds of subtle occlusions had reciprocal ST depression, indicating that other aspects of the ECG interpretation besides magnitude of ST segment elevation can help diagnosis.[1] As a database of more than 30,000 NSTEMI patients found, “Approximately one-quarter of patients with NSTEMI had an occluded culprit vessel at the time of angiography. Of these, 66% occurred in the posterolateral distribution, demonstrating the limitations of the current diagnostic approach to acute coronary syndromes, which relies heavily on STEMI/NSTEMI dichotomization for early treatment decisions.”[2]
As a consequence, a new paradigm is emerging, which uses insights from angiography and advances in ECG interpretation to identify the underlying condition that STEMI criteria fails to represent: Occlusion MI (OMI). As Pendell Meyers and Stephen Smith explain, “Twenty-five percent of patients diagnosed with NSTEMI have complete occlusion of the culprit vessel found on delayed angiogram, and a similar percentage of our cardiac catheterization lab activations turn out to be false positives. These false negatives [STEMI(−) OMI] are denied the opportunity to benefit from reperfusion therapy, while the false positives [STEMI(+) non-ACS] may receive harm from unnecessary cardiac catheterization…which has led us to propose a paradigm shift from the STEMI vs. Non-STEMI paradigm to one we call Occlusion MI vs. non-Occlusion MI (OMI vs. NOMI) paradigm.” [3]
Even when ECGs don’t meet STEMI criteria, NSTEMI guidelines also call for immediate invasive (within 2hr) reperfusion for patients with:
- refractory angina
- signs or symptoms of HR or new or worsening mitral regurgitation
- hemodynamic instability
- recurrent angina or ischemia at rest or with low-level activities despite intensive medical therapy
- sustained VT or VF [4]
Back to the cases
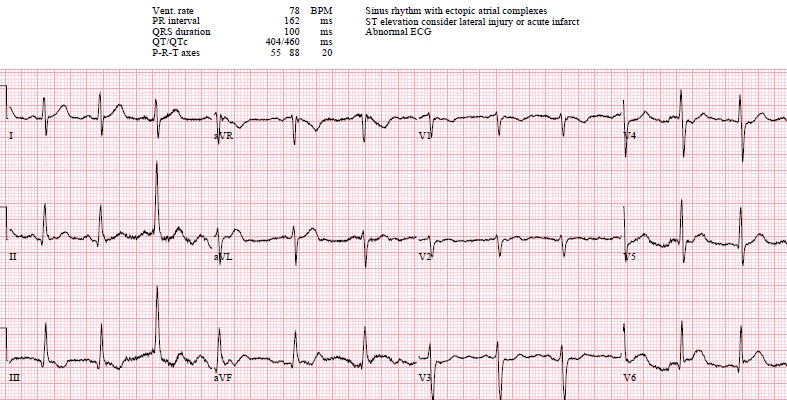
Patient 1: inferoposterolateral STEMI(+)/OMI(+)
NSR, normal conduction/axis/R wave progression, no hypertrophy. First ECG has V2 placed too high, giving inverted P/T waves, which is corrected on second ECG. There’s 1mm inferolateral ST elevation that meets STEMI criteria but which can also be seen with pericarditis. But there are also hyperacute T waves (most obviously inferiorly, where they are larger than their preceding R wave) , and dynamic reciprocal changes in aVL (which is very specific for inferior MI). STE in III also becomes convex, and there is ST depression in V2 concerning for posterior extension. Cath lab activated: circumflex occlusion. Follow-up ECG: resolution of ST elevation, hyperacute T waves, reciprocal change in AVL and ST depression in V2.
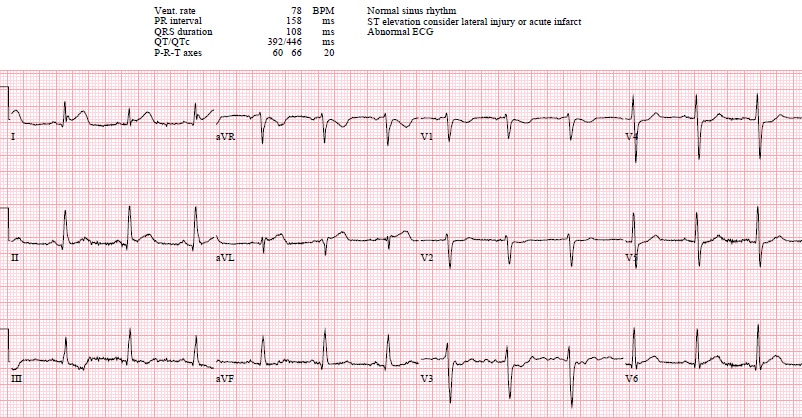
Patient 2: STEMI(-)/OMI(-), unnecessary cath lab activation
Sinus tach, normal conduction/axis/R wave, no hypertrophy. What the machine calls ST elevation is PR depression. Negative trops and normal angiogram.
Patient 3: STEMI(-), posterolateral OMI(+), false cath lab cancellation
NSR, normal conduction/axis, delayed R wave progression, no hypertrophy. There’s dynamic ischemic changes in the lateral leads: I develops ST elevation, aVL develops a Q wave and hyperacute T wave, V6 ST elevation normalizes, and there’s reciprocal changes in III and anterior ST depression in V2-3. But because the ECG did not meet STEMI criteria the Code STEMI was cancelled. When serial trops rose the cath lab was activated again: circumflex occlusion, peak trop 50,000. Follow-up ECG: normalizing ST segments and reperfusion T wave inversion in I-aVL
Patient 4: STEMI(-), posterolateral OMI(+), reciprocal changes first
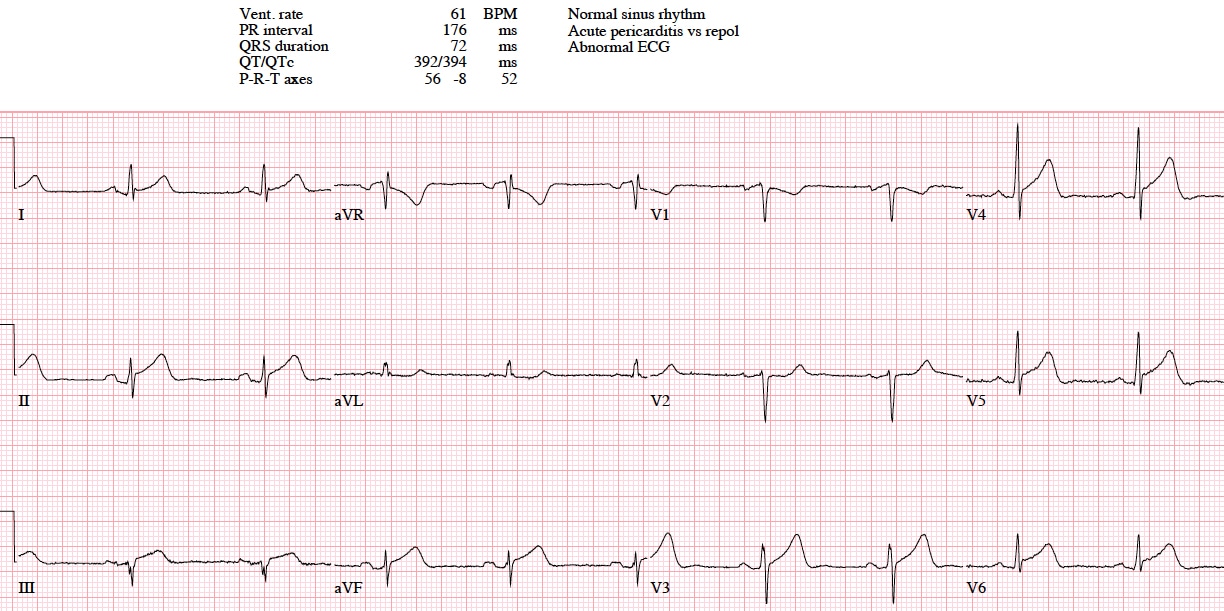
NSR, normal conduction, new left axis, new tall R wave in V2 with ST depression, new inferior ST depression–concerning for posterolateral occlusion MI with reciprocal changes presenting first. ECG signed off and patient seen 90 minutes later, repeat ECG:

Now there’s ST elevation aVL (still only one lead) and convex ST segments V4-6 with greater inferior reciprocal changes, and cath lab activated: occluded OM1 branch of circumflex. First trop negative, peak 40,000
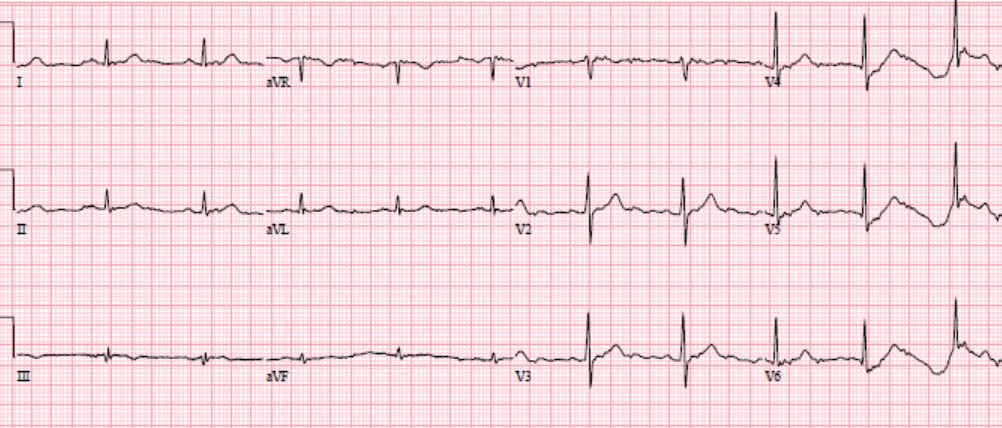
Patient 5: STEMI(-), lateral OMI(+)
NSR, normal conduction, left axis, normal R wave progression. LVH. There’s only ST elevation in V6, but there are also deWinter T waves (ST depression with peaked T waves) in V4-5, with inferior reciprocal changes. Cath lab activated: occluded first diagonal branch of LAD. First trop 120, peak 7,000. Discharge ECG: resolution of changes.
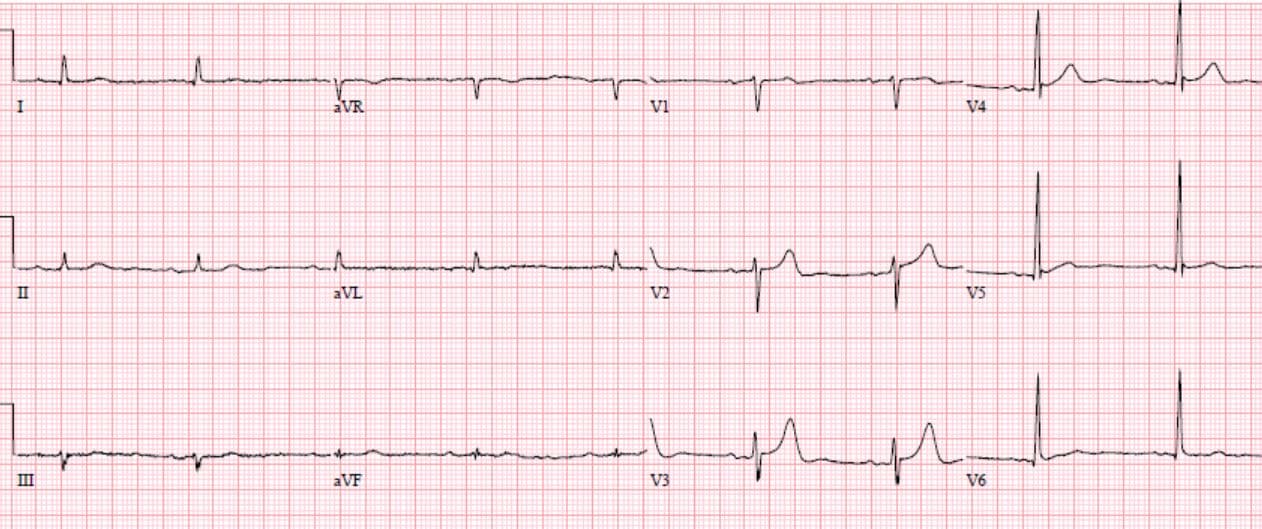
Patient 6: STEMI(-), high lateral OMI(+)
NSR, normal conduction/axis/R wave, no hypertrophy. There’s only ST elevation in aVL and it’s small. But relative to its QRS complex it is large, along with dynamic inferior reciprocal changes. Cath lab activated: occlusion of the OM1 branch of the circumflex. First trop negative, peak 14,000.
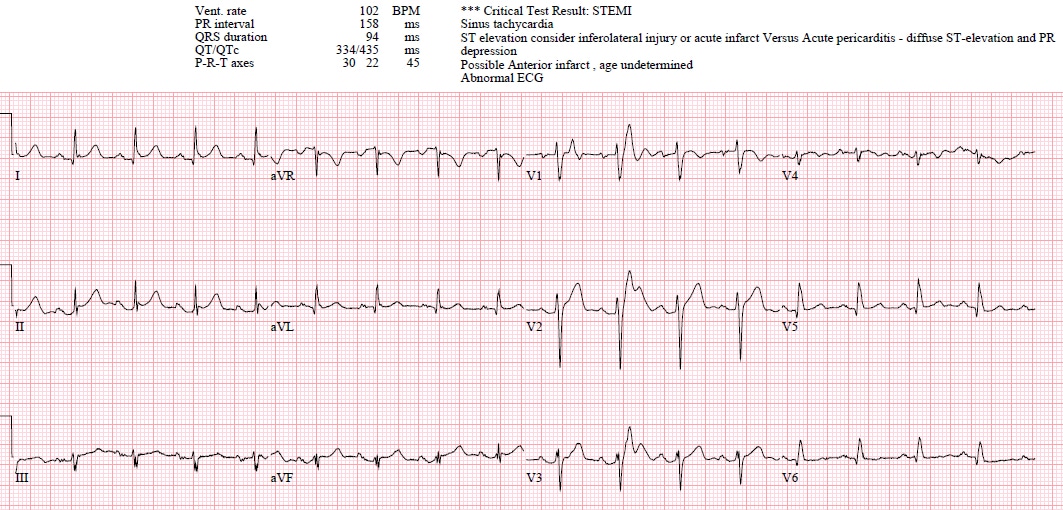
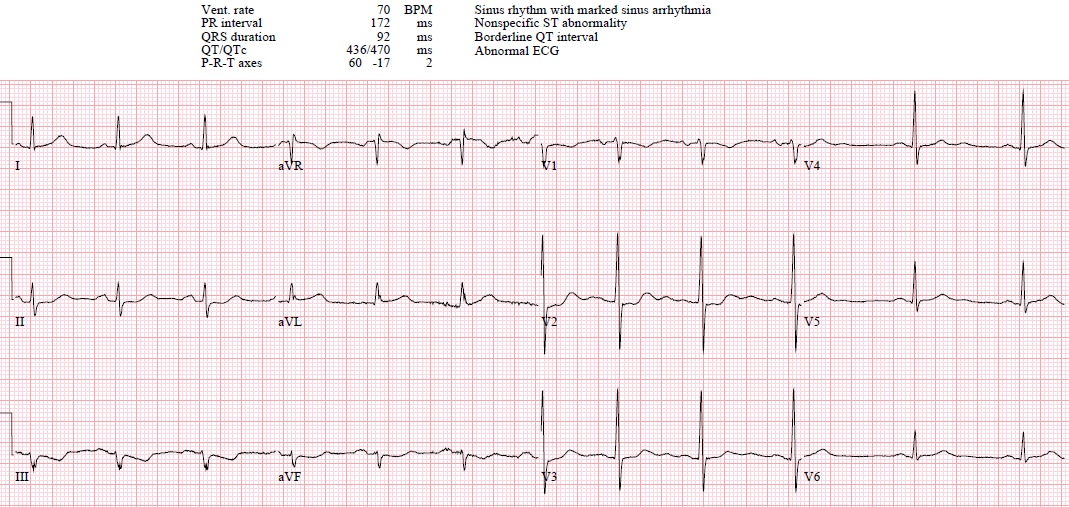
Patient 7: STEMI(-), ECG not diagnostic of occlusion clinical concern for refractory ischemia
NSR, normal conduction/axis/R wave, no hypertrophy. No significant ST changes, just convex ST segments III/aVR. But the patient had exertional and refractory chest pain. When trop came back positive cardiology was consulted stat and took patient to cath lab: circumflex occlusion
Take home
- STEMI criteria miss 25% of acute coronary occlusions, especially circumflex
- Other ECG signs of occlusion can help identify OMI, including new Q wave, dynamic ST changes, ST elevation relative to a small QRS complex, hyperacute T waves, reciprocal changes, and anterior ST depression from posterior extension
- Refractory angina is an indication for urgent reperfusion
- If in doubt: serial ECG, POCUS, stat cardiology
References for “ECG Cases 4: Lateral STEMI or OMI?”
- Marti D, Mestre JL, Salida L, et al. Incidence, angiographic features and outcomes of patients presenting with subtle ST-elevation myocardial infarction. Am Heart J 2014 Dec;168(6):884-90
- Dixon WC, Wang TY, Dai D, et al. Anatomic distribution of the culprit lesion in patients with non-ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: findings from the National Cardiovascular Data Registry. J Am Coll Cardiol. 2008;52(16):1347-8.
- Meyers HP, Smith SW. Prospective, real-world evidence showing the gap between ST elevation myocardial infarction (STEMI) and occlusion MI (OMI). Int J Cardiol. 2019;293:48-49.
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes
A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014 Dec 23;64(24):e139-e228



Fantastic as always, thanks!
Great post, love it. Examples make everything much more tangible. I think you mean “convex ST segments III/aVF” instead of “convex ST segments III/aVR” in Patient 7. Cheers!
Thanks for the feedback, and the correction!