
In this ECG Cases blog we explore 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. Can you identify which ones had acute coronary occlusion?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. November 2019
8 patients presented with potentially ischemic symptoms. Which had acute coronary occlusions?
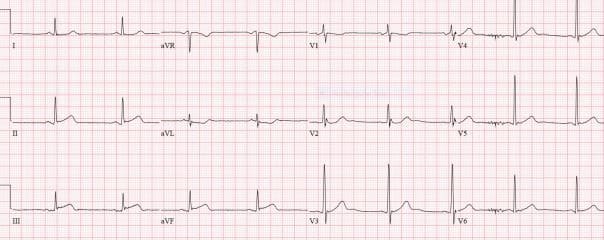
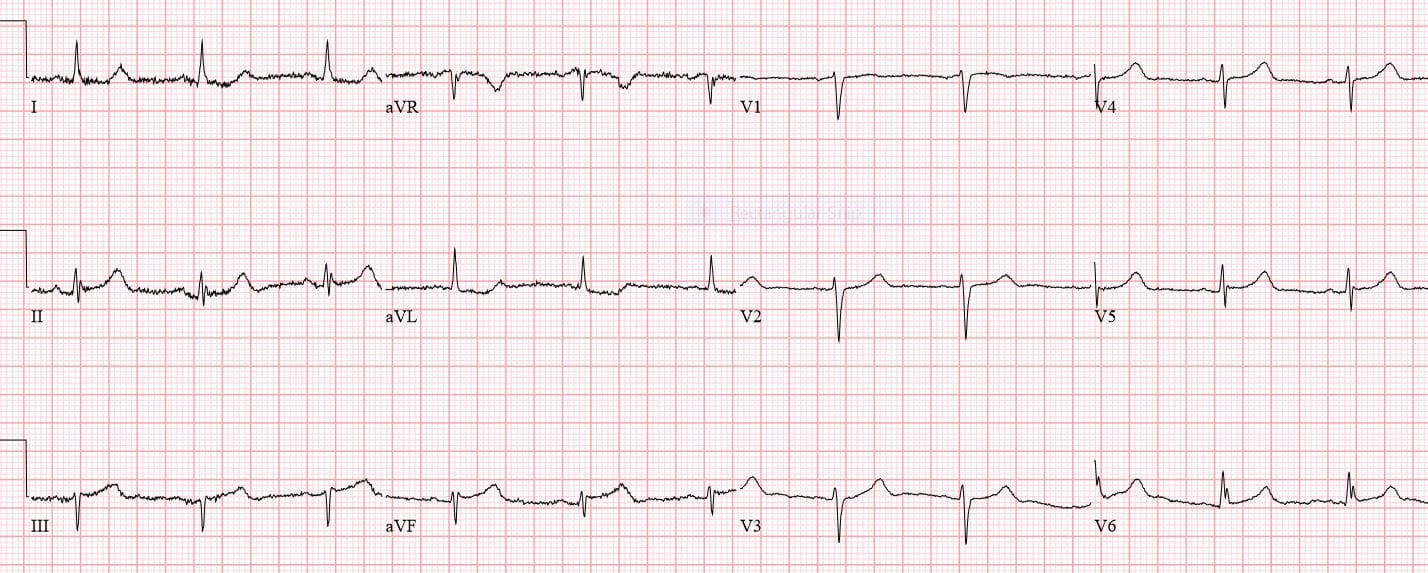
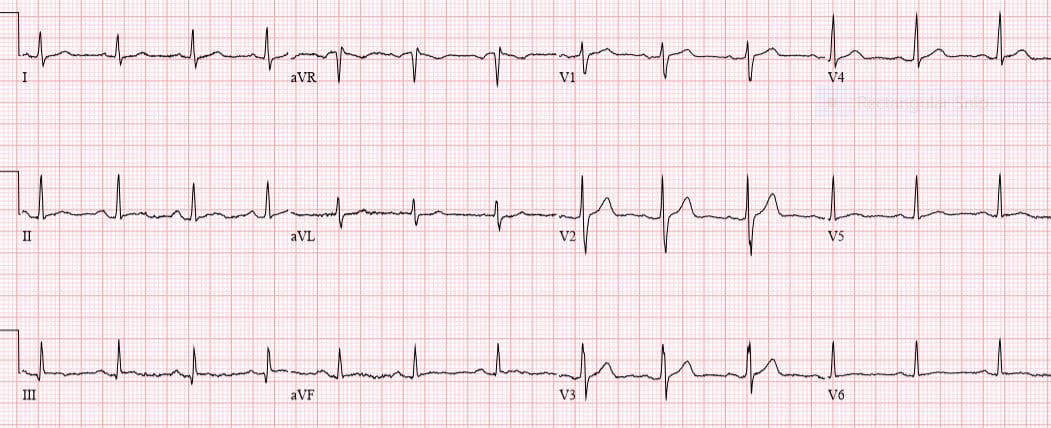
Patient 1: 50yo with indigestion, machine “nonspecific”
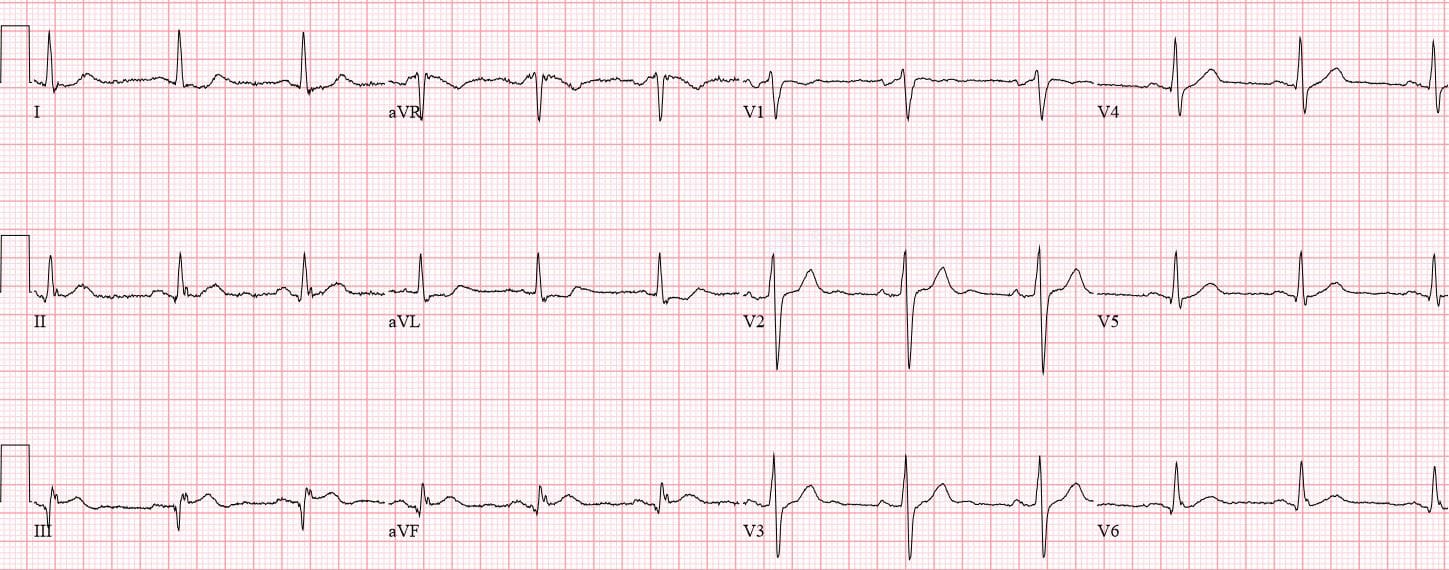
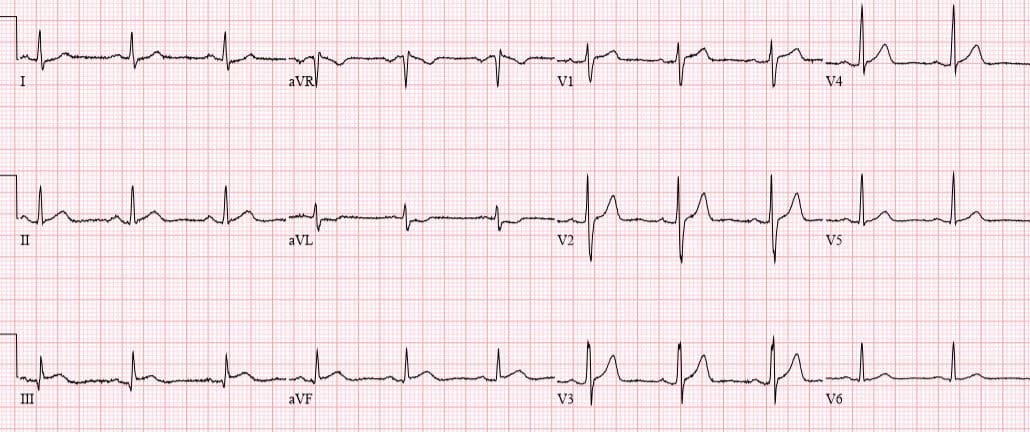
Patient 2: 45yo smoker with 90 minutes of chest pain
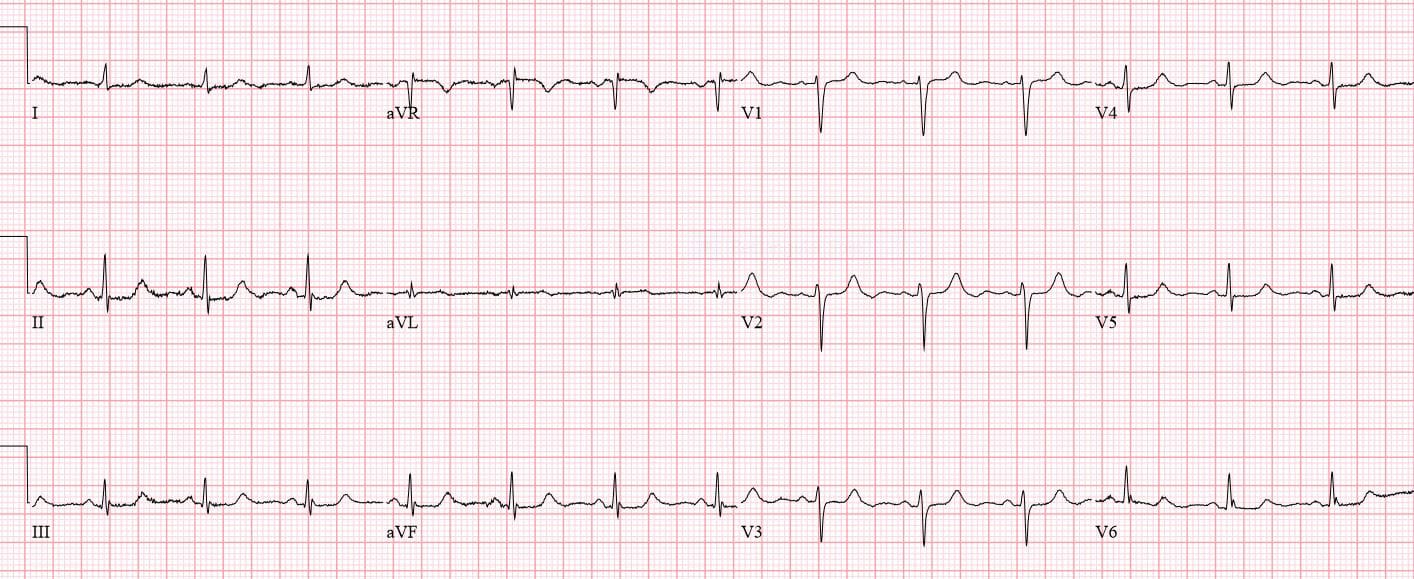
Patient 3: 50yo with palpitations and SOB. Old ECG then new ECG, machine “STEMI”


Patient 4: 75yo dialysis patient with 2hrs chest pain. Old then new ECG
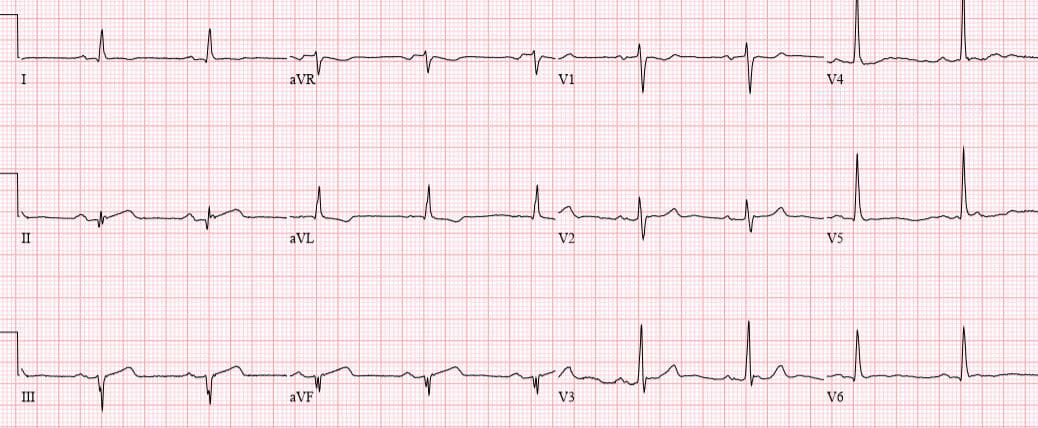
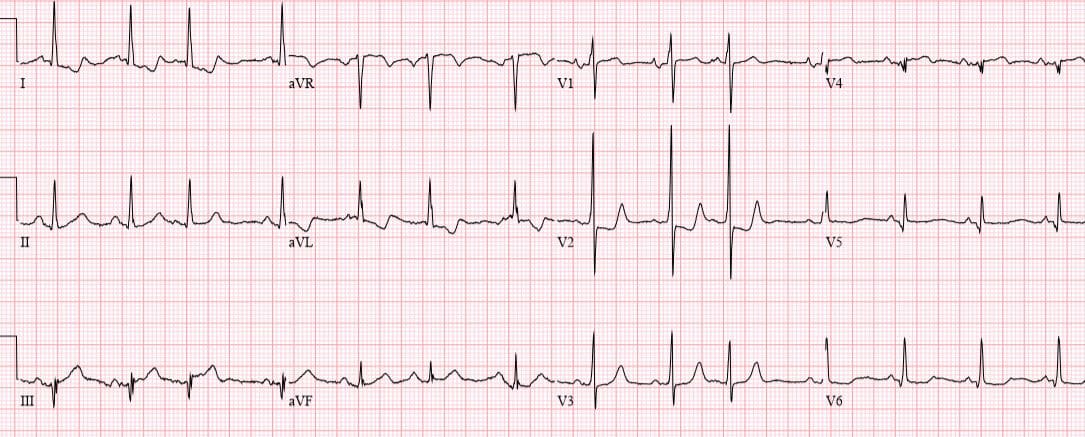
Patient 5: 35yo with chest pain, ECG “nonspecific”
Patient 6: 50yo chest pain, SOB. ECG “STEMI”

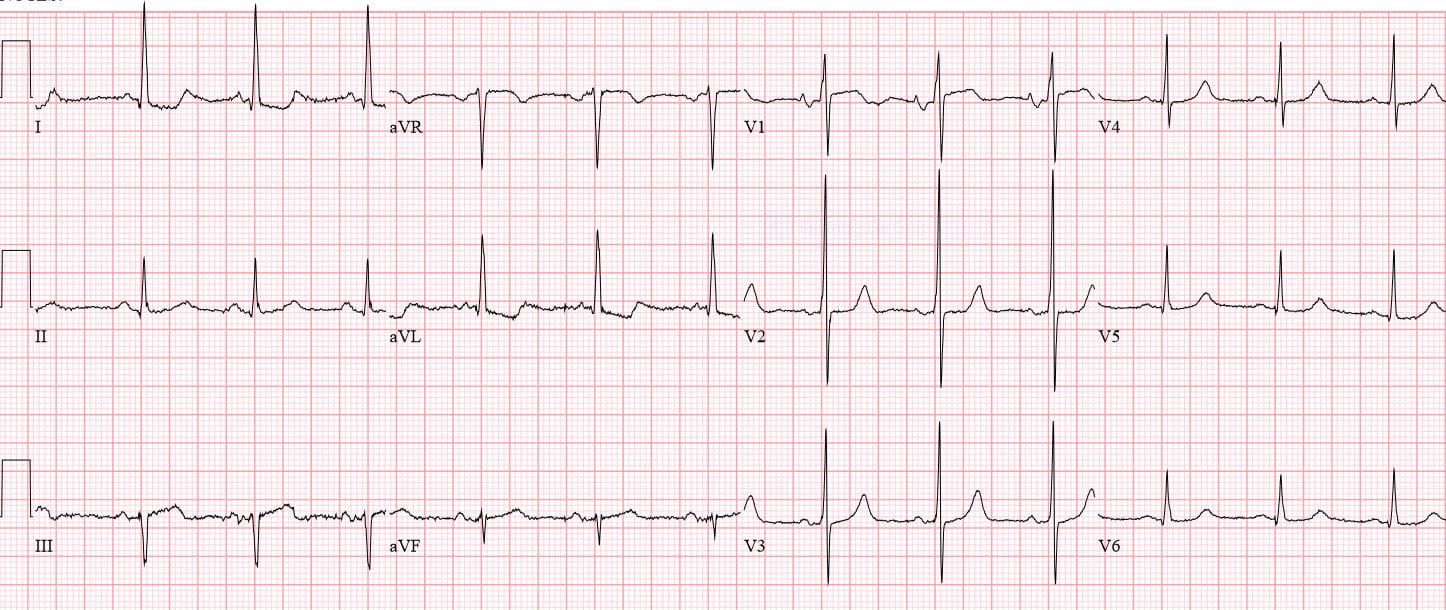
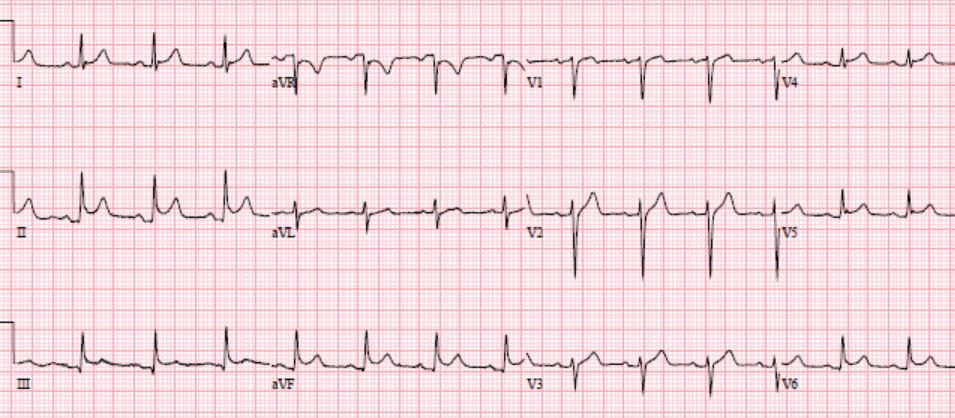
Patient 7: 75yo with acute chest pain, ECG “STEMI”

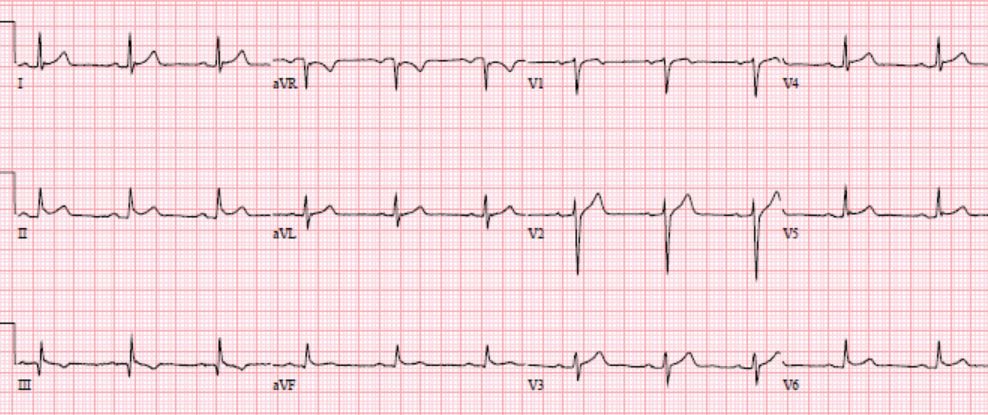
Patient 8: 85yo CP, machine “LVH”
Inferior MI
According to STEMI guidelines, patients with inferior MI only qualify for emergent reperfusion if they have at least 1mm of ST elevation in two contiguous inferior leads. But the problems with this threshold, and a solution, were recognized more than 25 years ago.
In 1993 a study of 107 patients with inferior MI, only 61% of patients had 1mm of ST elevation in all three leads, and this only rose to 87% if the threshold was dropped to 1mm of ST elevation in one inferior lead–meaning that 13% of inferior MI had no significant ST elevation in any lead. But 0.5mm ST depression in aVL was 97% sensitive for identifying inferior MI, including the 7.5% of patients for which it was initially the only abnormality.[1] aVL is the only lead reciprocal to the inferior wall and is very sensitive for inferior MI, and like other reciprocal changes can precede ST elevation. It should be noted that this study excluded patients with baseline ST depression in aVL: previous inferior MI or cardiomyopathy, aberrant conduction (LVH or LBBBB), and those with inferior T wave inversion.
More recent studies have found that 18% of STEMI patients have ST elevation less than 1mm (two-thirds of involving the inferior wall), and only a quarter received reperfusion within the first hour of arrival [2]. Not only is reciprocal ST depression in aVL more sensitive than STEMI criteria for identifying inferior MI, it also excludes one of its mimics: pericarditis. In a study of 426 cases of inferior MI , of which only 87% met STEMI criteria, 99% had some ST depression (0.25mm) in aVL; and zero of 49 cases of pericarditis had any ST depression in aVL. The study excluded those with aberrant conduction (LBBB, paced rhythm, WPW), which produce can produce secondary repolarization abnormalities including ST depression in aVL . As the authors concluded,
“In addition to differentiating STEMI from pericarditis, our findings will also be useful for identifying subtle inferior STEMI–in which the STE in the inferior leads is not large enough to meet traditional STEMI criteria (1mm in 2 contiguous leads)…We recommend scrutiny of lead aVL in patients with a suspicion of acute inferior MI. Those with any depression in aVL may have subtle coronary occlusion and should be intensively evaluated with serial ECGs, immediate formal echocardiography, or angiography, instead of a more relaxed approach in which MI is only ruled out by biomarkers.”[3]
Back to the cases
Patient 1: missed inferior MI
NSR, normal conduction/axis, no hypertrophy. Subtle concave inferior STE in II/III/aVR with reciprocal ST depression in aVL, along with anterior tall R wave and relative ST depression from infero-posterior MI. Trop negative and sent home. Came back next day with the same symptoms, with a trop of 20,000 and inferior Q waves. Cath lab: RCA occlusion

Patient 2: subtle inferior MI diagnosed
NSR, normal conduction/axis/R wave, no hypertrophy. Subtle concave ST elevation III/aVF with reciprocal ST depression in aVL. POCUS: inferior wall motion abnormality. Cath lab activation: RCA occlusion. First trop 70, peak 50,000.
Patient 3: PR depression, old changes in aVL, unnecessary cath lab activation
NSR, normal conduction/axis/R wave, no hypertrophy. There is mild ST depression and T wave inversion in aVL but it is old, and what the machine called inferior ST elevation is PR depression. Cath: normal coronaries
Patient 4: dynamic inferior MI, delayed diagnosis
NSR, normal conduction, delayed R wave progression, no hypertrophy, baseline nonspecific ST depression. Compared with the old ECG there is new left axis and Q in III, mild concave ST elevation in aVF with reciprocal ST depression in aVL. Trop mildly positive and referred to cardiology as NSTEMI. Repeat ECG two hours later: obvious inferior STEMI. Cath lab: RCA occlusion.
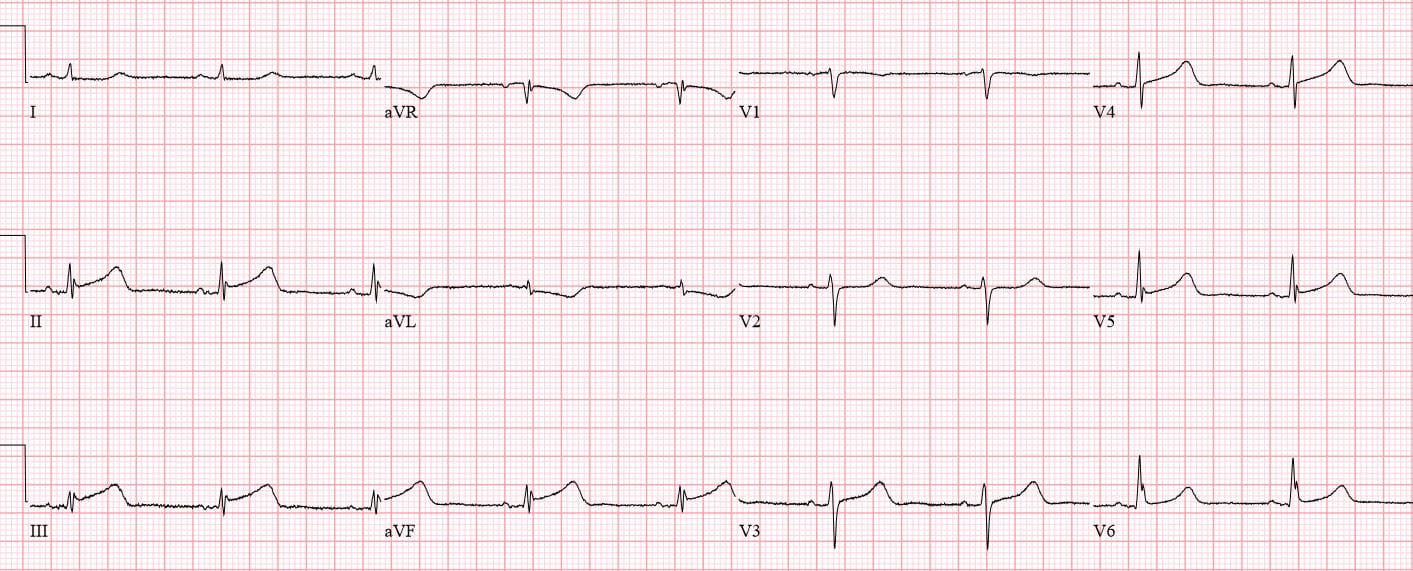
Patient 5: dynamic inferior MI, missed
NSR, normal conduction/axis/R wave, no hypertrophy. Mild concave ST elevation III/aVF with reciprocal depression in aVL. Trop 1500, referred to cardiology as NSTEMI. Repeat ECG: resolving ST elevation/reciprocal change from spontaneous reperfusion. Cath: 80% RCA occlusion
Patient 6: pericarditis
NSR, normal conduction/axis/R wave, no hypertrophy. Mild inferior concave STE with normal aVL; isolated Q wave in III can be normal. Repeat ECG no change. Six hour troponin negative and repeat ECG:
Greater inferolateral concave ST elevation, still without any reciprocal change in aVL. Admitted for echo and serial enzymes, all normal. Next day ECG normal:
Patient 7: old vs new MI

NSR, normal conduction/axis/R wave, no hypertrophy. There are inferior Q waves, convex ST elevation and terminal T wave inversion, with reciprocal ST depression in aVL, and anterior ST depression from infero-posterior MI. This could be old, but the patient had no history of an MI and these are new compared with the prior ECG. Signed off by first physicians, second physician called code STEMI:
Discharge ECG had ongoing inferior Q waves and non-concave ST segments, with ST depression and T wave inversion in aVL
Patient 8: LVH vs STEMI
NSR, normal conduction, left axis, tall anterior R wave and LVH. ST depression in aVL could be from LVH, and the ST elevation in III is minimal, but there is also pseudonormal ST segments anteriorly. Signed off by first physician and seen an hour later. 15 lead ECG:
Greater ST elevation in III, ST depression in I/AVL and V2-3. Cath lab activated: 99% RCA occlusion
Take home points
- ST depression in aVL can be secondary to prior MI or LVH but should not automatically be attributed to them
- Primary ST depression in aVL is highly sensitive for inferior MI, differentiates if from pericarditis, can be the first sign of occlusion, and can prompt a search for other signs of occlusion–including subtle ST elevation, straightening of the ST segments, hyperacute T wave, new Q waves, anterior ST depression/pseudonormalization, or ST elevation in posterior leads
- If in doubt: serial ECGs, POCUS, urgent cardiology consult
References for “Can you identify subtle inferior MI”
- Birnbaum Y, Sclarovsky S, Mager A, Strasberg B, Rechavia E. ST segment depression in a VL: a sensitive marker for acute inferior myocardial infarction. Eur Heart J. 1993;14(1):4-7.
- Marti D, Mestre JL, Salida L, et al. Incidence, angiographic features and outcomes of patients presenting with subtle ST-elevation myocardial infarction. Am Heart J 2014;168(6): 884-890
- Bischof J, Worral C, Thompson P, et al. ST depression in lead aVL differentiates inferior ST elevation myocardial infarction from pericarditis”. Am J Emerg Med. 2015;34(2):149-154.



another excellent series
thanks!
Dr. McLaren…
I just found your website and read this article. I am very impressed with your advanced ECG knowledge and also your (apparent) acceptance of the OMI Manifesto! I look forward to reading more of what you have to say. Thank you for a really great article.
Thanks! The OMI Manifesto was definitely an inspiration, and I’ll be sure to add your own website to the list of experts I learn from.
What was the outcome of the cath lab activation for patient 7? Was there RCA occlusion?