
We are amidst a paradigm shift in the emergency management of acute ischemic stroke. The traditional way of categorizing ischemic strokes as ‘minor’ vs ‘major’ is no longer relevant to what we do in the ED. It’s now about ‘disabling’ vs ‘non-disabling’ strokes. And this is no small change. This categorization dictates urgency of ED work-up and treatments, imaging choices, treatment decisions and goals of care. In this Part 1 or our 2-part main episodes EM Cases podcast series on management of ischemic stroke with Dr. Walter Himmel and Dr. Katie Lin, we answer questions like: How can we best rapidly determine if an ischemic stroke is disabling or non-disabling at the bedside? In what ways are ‘wake up strokes’ managed uniquely and what’s the latest thinking on their pathophysiology? How should we best prioritize imaging depending on timing, geography and resources? How do we best predict large vessel occlusion amenable to endovascular therapy (EVT) at the bedside? How can we efficiently establish goals of care at the bedside to inform our emergency decision making around strokes? Which is better for thrombolysis in ischemic stroke – Tenecteplase or Alteplase? How have contraindications to IV thrombolysis changed over the last decade? When should we consider bridge therapy with EVT after IV thrombolysis? What are 4 key items the ED physician should have ready for the stroke neurologist on the first call? and many more…
Podcast: Play in new window | Download (Duration: 1:36:12 — 88.1MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Anton Helman October, 2025
Cite this podcast as: Helman, A. Himmel, W. Lin, K. A Paradigm Shift in Ischemic Stroke Management Part 1: Disabling Strokes. Emergency Medicine Cases. October, 2025. https://emergencymedicinecases.com/ischemic-stroke-management-disabling-strokes. Accessed July 25, 2026
Major vs Minor Stroke – An impractical categorization of stroke
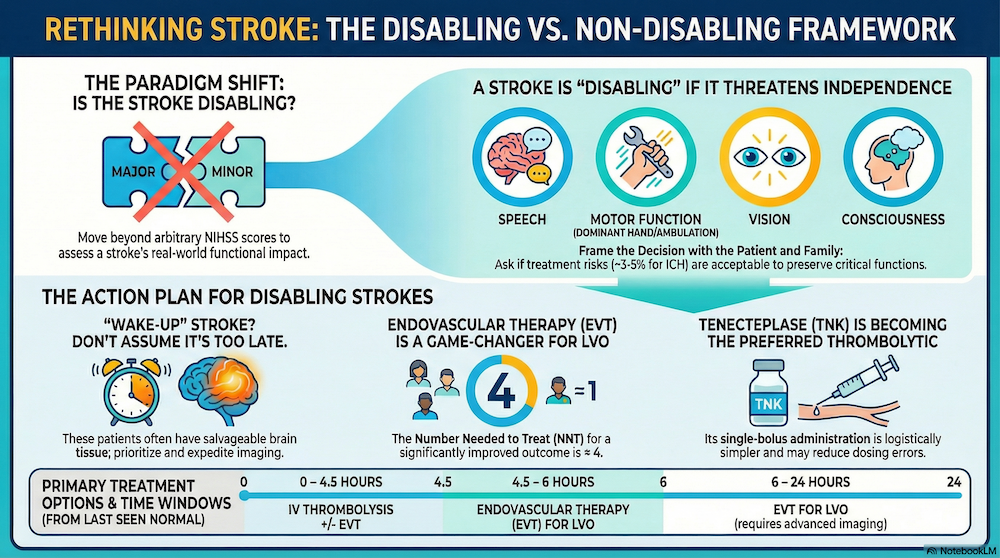
The historical “major (NIHSS ≥5) vs minor (NIHSS <5)” dichotomy is convenient for research stratification but problematic clinically: so-called “minor” presentations (e.g., isolated aphasia, dense hemianopia, disabling distal limb weakness of the dominant hand) frequently carry marked functional morbidity and should not be excluded from reperfusion solely on the basis of a low NIHSS. The contemporary approach reframes categorization around disability and patient-centred outcomes rather than an arbitrary score threshold.
NIHSS is a descriptor, not a decision tool. A low score can still be functionally catastrophic and should not exclude reperfusion.
Pitfall: One pitfall in the decision to employ IV thrombolytics and/or endovascular therapy (EVT) is to assume that a minor stroke (NIHSS <5) is not eligible for such therapies. Many patients who have an NIHSS <5 have disabling stroke that do fulfill criteria for these aggressive, time dependent therapies.
Disabling vs Non-disabling – The practical categorization of ischemic stroke
Reframe the first decision point as disabling vs non-disabling. A structured conversation around values helps determine whether a deficit is “disabling” for this patient. At the bedside, determine whether the deficit is disabling for this patient—i.e., likely to compromise independent living, employment, or meaningful communication. Cortical signs (aphasia/dysphasia, neglect, gaze deviation, hemianopia) combined with significant motor deficits imply a high pretest probability of large-vessel occlusion (LVO) and generally warrant aggressive reperfusion pathways when imaging and contraindication screening align with benefit. A patient-centred frame improves both selection for reperfusion and shared decision-making. Classify the presentation as disabling when it threatens independence or meaningful quality of life (speech/language, vision, ambulation, dominant-hand function, or level of consciousness), and nondisabling when deficits are unlikely to impact these domains if untreated. This “disability” lens operationalizes risk-benefit conversations around things patients value (home, work, communication), rather than a numerical threshold.
-
Core principle: Focuses on deficits that disrupt independence and meaningful activities, e.g., speech, vision, motor, consciousness.
-
Features typically considered disabling:
-
- Speech: Major speech deficit (severe aphasia or dysarthria compromising functional communication)
- Motor: Dense motor loss (especially dominant hand/arm, profound leg weakness)
- Vison: Amaurosis fugax, cortical blindness, dense hemianopia.
- Consciousness/Brainstem: depressed level of consciousness, locked-in syndrome from basilar occlusion.
-
Patient and family context:
-
- What is disabling varies with occupation, age, lifestyle.
- Shared decision-making is vital for subtle deficits.
-
Implementation: ED teams must weigh patient’s premorbid status, functional demands, and goals of care.
Bedside script (shared decision-making): “There are time-sensitive treatments that can help, but they carry bleeding risks (~3–5% symptomatic ICH with IV thrombolysis). Given your deficits and what matters to you, are these risks acceptable to try to preserve speech/hand/ambulation?”
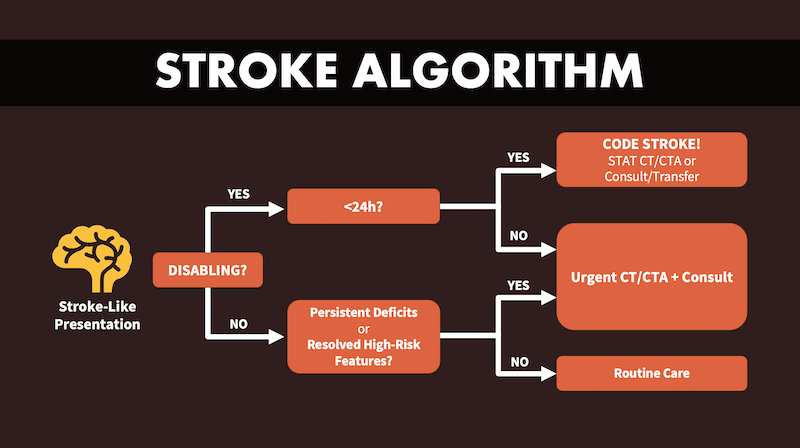
Below is Dr. Lin’s basic ischemic stroke algorithm based on the ‘disabling’ vs ‘non-disabling’ categorizations of stroke to be used as a framework for these 2 EM Cases episodes on ED management of ischemic stroke.
The Importance of Time Windows in Disabling Ischemic Stroke Management
- 0–4.5 h: May be eligible for IV thrombolysis (per local protocol); a subset also proceeds to EVT when CTA confirms large vessel occlusion (LVO) – see ‘bridge therapy’ below.
- 4.5–6 h: IV thrombolysis generally excluded; EVT remains indicated when CTA demonstrates large vessel occlusion (LVO)—no additional imaging beyond CTA is required for selection in this interval.
- 6–24 h (late window): Selection hinges on advanced imaging beyond CTA to demonstrate a small infarct core with a robust penumbra (e.g., favorable CTP, multiphase CTA collaterals, or MRI mismatch).
The Significance of ‘Last Seen Normal’ in Ischemic Stroke Management
- Definition: Last time patient was at neurologic baseline (not just symptom onset).
- Utility: Determines upper time boundary for treatment eligibility.
- Application: Especially critical in unwitnessed and “wake-up” strokes.
- Acute therapies: IV thrombolysis usually offered up to 4.5 hours, EVT up to 24 hours, all measured from “last seen normal.”
- Evidence: Late window trials (DAWN, DEFUSE3) justify aggressive intervention ≤24 hours with favorable imaging.
“Last seen normal” (LSN) anchors onset time when symptoms are unwitnessed; however, LSN should not be conflated with tissue viability. Patients presenting close to 24 h from LSN may still be candidates for late-window endovascular therapy (EVT) if imaging reveals a small infarct core with a substantial penumbra. Practically, LSN documents chronology; selection for therapy is driven by imaging-demonstrated salvageable tissue.
“Wake Up” Strokes – Where urgent imaging is paramount
A wake up stroke occurs when precise onset is unknown, but “last seen normal” is when patient went to sleep. Most wake-up strokes occur just before awakening due to physiologic changes (cortisol/BP spikes), a time at which there is likely to be more salvagable tissue that can be saved by EVT than if the time of the stroke occurred upon falling asleep. Imaging may be more likely to reveal salvageable tissue, making many wake-up stroke patients candidates for EVT. Many patients treated in the extended (≤24 h) reperfusion window in landmark thrombectomy trials (Dawn, Extended IA, Diffuse 3) were wake-up strokes; physiology (diurnal BP/cortisol surge) suggests many such events occur shortly before waking. Unknown onset should trigger, not throttle, reperfusion work-up. Do not exclude patients from EVT on time grounds for wake up strokes; instead, expedite imaging for all suspected wake-up strokes.
Pitfall: Do not exclude wake up stroke patients from EVT on time grounds alone; instead, expedite imaging for all suspected wake-up strokes, as many of these strokes occur close to the time of awakening.
Treat wake up strokes as time-critical like any stroke: Non-contrast CT to exclude hemorrhage + CTA head/neck to assess for LVO; add advanced imaging (CTP, multiphase CTA, or MRI DWI–FLAIR mismatch) when beyond standard IV thrombolysis windows or onset is uncertain. Consider IV thrombolytics (TNK or tPA per local protocol) when advanced imaging shows salvageable tissue (e.g., DWI–FLAIR mismatch or favorable CTP profile) and there are no contraindications. If CTA shows LVO, proceed down your EVT pathway. In unknown/late windows, use CTP/multiphase CTA/MRI to confirm a small core with salvageable penumbra. Bridging lysis is still reasonable when eligible (anatomy may preclude rapid catheter access, and early recanalization can occur while mobilizing the suite).
Clinical Determination of Large Vessel Occlusion – The scores are not reliable!
Look for dramatic arm weakness plus cortical signs (aphasia/dysphasia, neglect, gaze deviation, hemianopia). This constellation implies high LVO probability → CTA ASAP to determine eligability for EVT and rapid transfer if needed. Clinical LVO tools (e.g., VAN, ACT-FAST (see blelow), Cincinnati, LAMS) are reasonably sensitive (~80–90%) for pre-imaging triage, but lack specificity; when a disabling cortical syndrome is present, pursue vascular imaging even if a scale is “negative”.
Pitfall: A “negative” FAST or VAN or Cincinnati score does not rule out a LVO stroke that may be eligable for EVT. Prioritize CTA for any disabling focal deficit whenever feasible.
Establishing Goals of Care and Determining Premorbid Status in Ischemic Stroke Management
Acute stroke decisions are time-critical; pair rapid medical assessment with a focused values discussion:
Dr. Lin’s 4 part approach to establishing goals of care:
- Signpost the urgency/time-sensitivity and importance of the conversation.
- Summarize what’s happening and the options (IV Thrombolysis/EVT or not), including best/worst-case outcomes and bleeding risk for both options.
- Align recommendations with what matters most to the patient (include 1. home independence, 2. return to work, 3. acceptable long term disability).
- Give your simplified recommendation.
Two-question premorbid screen:
- Where does the patient live? (independent home vs assisted vs long-term care)
- How do they mobilize? (independent vs aid vs bed-bound)
This rapidly informs whether aggressive therapy aligns with baseline quality of life.
Rapid, structured values clarification should occur in parallel with medical work-up. Discuss realistic best-/worst-case outcomes, bleeding risk, and likelihood of returning to independent living, home residence, and work—factors that most influence stroke survivors and families.
Systemic Thrombolytics in Ischemic Stroke Management
Indications for IV Thrombolysis in Ischemic Stroke Management
- Age: 18 years or older.
- Disabling: Symptoms suggestive of an acute ischemic stroke that are deemed to be disabling, regardless of whether there has been some early improvement. Disabling symptoms are specifically referenced as an inclusion criterion (e.g., aphasia, dominant‐hand weakness, dense hemianopia, etc.). When in doubt, our experts advise erring on the side of treating if the patient is in window, has no contraindications, and the deficit is disabling — a normal CTA does not rule out eligibility.
- Time Window: Ability to initiate treatment within 4.5 hours from the time the patient was last seen normal. Unknown onset / wake-up stroke: still consider IVT if imaging selection and local stroke protocol support it; wake-up patients are often more likely to be treatable—expedite imaging rather than exclude on the basis of the clock.
- Plain CT Head: Diagnostic imaging (typically non-contrast CT) ruling out intracranial hemorrhage.
- Absence of Contraindications: Absence of absolute exclusion criteria, including but not limited to: recent head trauma, previous intracerebral hemorrhage, active internal bleeding, recent major surgery, or severe uncontrolled hypertension. Blood pressure can be made safe for lysis: Able to reduce/maintain BP to <180/110 before thrombolysis and <180/105 after; avoid hypotension. Note that age >80 and prior stroke + diabetes are no longer absolute exclusions; warfarin acceptable if INR <1.7; UFH off ≥4 h with normal PTT; LMWH >24 h; DOACs >48 h; untreated intracranial AVM remains a contraindication; judgment required for recent GI/GU bleeding and intracranial tumors (e.g., meningioma generally acceptable).
Pitfall: A common pitfall is assuming that a normal CTA deems the patient ineligible for IV thrombolysis. It is age of patient, disability, time and absence of thrombolysis contraindications that dictates eligibility for IV thrombolysis, not the findings on CTA.
The Evidence for Systemic Thrombolytics in Ischemic Stroke Management
- Most evidence supports admin ≤4.5hr from onset (window opened from 3hr in 2008 to 4.5hr)
- Improves functional outcome (modified Rankin score, NNT ~7 for good outcome if given promptly)
- Best results ≤90min; efficacy diminishes with time but remains present ≤4.5hr
- Risks:
- Symptomatic intracerebral hemorrhage 3–5%
- Door-to-needle:
- Goal is ≤30–60 minutes
Tenectaplase (TNK) vs Alteplase (tPA) – Which one is better?
-
Tenecteplase (TNK):
-
- FDA approved (2025) and guideline-recommended
- Single-bolus dosing simplifies workflow/logistics (versus continuous 1hr infusion for TPA)
- May reduce dosing errors, improve EMS and transport process
Multiple trials—including the Canadian ACT-QUICKR—support non-inferiority of tenecteplase (TNK) to alteplase (tPA) for functional outcomes, with signals toward superior reperfusion and a favorable safety profile in some cohorts. Logistics strongly favor TNK: single-bolus administration is thought to reduce dosing errors and simplify interfacility transfer when bridging to EVT.
Given at least non-inferior efficacy and pragmatic advantages, many systems are transitioning to TNK as first-line IV thrombolytic where available; agent selection remains protocol-dependent and should be harmonized with regional stroke pathways.
Contraindications to IV Thrombolytics in Ischemic Stroke Management Update 2025
-
Absolute contraindications:
-
- Active major bleeding, intracranial mass (mets, AV malformations), recent neurosurgery, uncontrolled hypertension (>185/110 prior to administration)
- Known coagulopathy (platelets <100,000, INR ≥1.7)
-
Relative contraindications—more liberal than before:
-
- Minor GI/GU bleeds, age >80, prior stroke/diabetes no longer strict, but risk remains increased
- DOACs: Must be held ≥48hr, LMWH ≥24hr
- Oral anticoagulants: INR <1.7 required
Updates to contraindication to IV Thrombolytics for Stroke 2025
- Age >80 y: no longer a contraindication.
- Prior stroke + diabetes: no longer a contraindication.
- Warfarin: acceptable if INR <1.7.
- UFH infusion: off ≥4 h and normal PTT.
- LMWH (e.g., enoxaparin, fragmin): wait 24 h since last dose.
- DOACs: (local protocols vary; many require ~48 h if normal renal function—confirm regionally).
- Eye surgery: recent corneal and lens surgery are generally not a contraindication while retinal surgery is a contraindcation
- Small unruptured aneurysm (<10 mm) and meningioma not absolute contraindications; untreated AVM remains a contraindication; recent retinal surgery may be a concern.
These updates align TNK with historical alteplase criteria; always confirm the dynamic local checklist at the bedside.
Endovascular Therapy in Ischemic Stroke Management
The Evidence for Endovascular Therapy in Ischemic Stroke Management
EVT became standard of care for LVO with the 2015 NEJM trials (≤6 h), then expanded to up to 24 h in 2018–2019 based on late-window selection by advanced imaging (DAWN, DEFUSE 3). Across meta-analyses, NNT ≈4 for significant improved functional outcomes. Selection criteria included clinical severity, imaging confirmation (large vessel occlusion, salvageable penumbra via advanced imaging; see below).
Bridge Endovascular Therapy – when are both IV thrombolysis and EVT indicated?
RCTs and recent meta-analyses suggest that giving intravenous thrombolysis—either with alteplase (tPA) or tenecteplase (TNK)—before or during endovascular therapy (EVT) for disabling ischemic stroke results in similar functional outcomes compared to EVT alone, but there are nuanced benefits in some analyses, especially when prompt IV lysis is possible. Whether to bridge with IV thrombolysis before EVT remains under active study and there is no clear consensus on specific indications. Practical reasons to still give IV thrombolysis when eligible: EVT access failures (tortuous anatomy, dense clot) and potential for earlier recanalization while mobilizing the suite. Practice varies (US, Canada, Europe); always confirm guideline for local variant.
Summary of Key Evidence for bridge therapy in ischemic stroke
- Multiple RCTs and meta-analyses involving thousands of patients with large vessel occlusion have directly compared combination therapy (IV tPA or TNK plus EVT) versus EVT alone.
- Most data indicate no statistically significant difference in the primary endpoint of functional independence (modified Rankin Scale 0–2 at 90 days) between the two strategies.
- Some large observational studies and recent meta-analyses suggest that combination therapy may reduce disability (shift analysis), increase successful reperfusion rates, and shorten time to reperfusion, translating to higher likelihood of home discharge and better ambulation at discharge, albeit with a small increased risk of symptomatic intracranial hemorrhage.
- No significant difference in all-cause mortality, excellent outcome (mRS 0–1), or symptomatic intracranial hemorrhage has been consistently reported between groups; however, patients with faster access to thrombolysis, or in whom EVT might be delayed, may benefit more from IV therapy in addition to EVT.
- Analysis of tenecteplase (0.25 mg/kg or 0.4 mg/kg) and alteplase (0.9 mg/kg) in RCTs found higher successful reperfusion with pre-EVT tPA or TNK, but overall functional outcomes remained similar to EVT alone. Subgroup analyses stress the importance of patient and workflow selection.
The bottom line for bridge therapy in ischemic stroke
Combination therapy with IV tPA or TNK plus EVT is not inferior to EVT alone and is associated with improved reperfusion and potential functional advantages in certain patients, especially with prompt administration, but does carry a small risk increase for intracerebral hemorrhage. Clinical guidelines frequently recommend combination therapy when feasible and not delayed, particularly for patients with disabling symptoms who are eligible for both treatments
The Importance of the Penumbra in Ischemic Stroke Management
Conceptually, every stroke comprises core, penumbra, and normal tissue. Reperfusion therapies aim to salvage the penumbra; the likelihood of benefit depends on collateral perfusion and the tempo of penumbral collapse. Advanced imaging that demonstrates a small core with a large penumbra identifies patients most likely to achieve substantial functional recovery—even deep into the late window. Treatment aims to salvage hypoperfused but viable tissue; robust collaterals can keep penumbra alive into the late window, while poor collaterals collapse fast—hence the centrality of imaging-based selection.
Clinical Criteria Summary Table for Endovascular Therapy for Ischemic Stroke
| Requirement | 0–6 hr window | 6–24 hr window |
|---|---|---|
| Age | Any adult (no strict) | Some trials >18, <80/85 |
| LVO on CTA | Required | Required |
| Disabling deficit | Required | Required |
| Infarct core (ASPECTS/core volume) | ASPECTS ≥6 | ASPECTS ≥6, <50–70 mL |
| Clinical–core mismatch | Not mandatory | Mandatory |
| Multiphase CTA/collaterals | Supportive | Mandatory/strongly rec. |
| Informed consent | Best practice | Best practice |
Time-based criteria for endovascular therapy in ischemic stroke
-
0–6 hours from last seen normal:
-
EVT indicated for most eligible patients with LVO, disabling symptoms, and minimal infarct core seen on non-contrast CT.
-
Imaging: Plain CT to rule out hemorrhage, CTA for LVO; go directly to EVT center (do not delay for advanced imaging).
-
-
6–24 hours window (“extended” or “late” window):
-
EVT is considered only if advanced imaging (CT perfusion, MRI DWI/FLAIR, or multiphase CTA) shows:
-
-
-
- Small infarct core (e.g., <70 mL by RAPID or similar algorithms).
- Large viable penumbra (ischemic but salvageable tissue).
- Clinical–imaging mismatch (NIHSS relative to core size).
-
Imaging requirements for endovascular therapy in ischemic stroke
-
Non-contrast CT:
-
- Excludes intracranial hemorrhage.
- Assesses established infarct core using ASPECTS (Alberta Stroke Program Early CT Score; ≥6 preferred for benefit).
-
CT Angiogram (CTA):
-
- Confirms presence and site of LVO.
- Assesses for tandem lesions (extracranial/intracranial) and dissection.
-
Advanced imaging for late window:
-
CT perfusion or MRI DWI/FLAIR:
-
-
-
- Measures infarct core and penumbra (thresholds: DAWN used <21 mL for >80 years and high NIHSS, <31 mL for 60–79, <51 mL for <60).
- Clinical–core mismatch: e.g., NIHSS ≥10, core <31 mL.
-
Multiphase CTA:
-
Evaluates collateral flow to predict tissue at risk and possible benefit.
-
-
Relative or exclusion criteria for endovascular therapy
- Large established infarct (ASPECTS ≤5, core >70 mL): Associated with higher risk of hemorrhagic transformation and poorer outcome; EVT generally not recommended unless compelling clinical rationale.
- Minor, nondisabling symptoms: Benefit–risk does not favor EVT.
- Premorbid disability (mRS >2): Usually excluded, but individualized if new deficit prevents return to meaningful baseline function.
- Poor vascular access or life expectancy <6 months.
- Other severe comorbidities limiting benefit from intervention.
Special clinical scenarios for endovascular therapy consideration
- Basilar artery occlusion: EVT can be considered beyond 6 hr if clinical and imaging profile favorable; no strict upper time limit in some guidelines due to devastating natural history.
- Tandem occlusions (carotid + intracranial): May require acute stenting + thrombectomy; requires coordination with neurointerventional team.
- Stroke on anticoagulation: Relative contraindication; consult stroke team for individualized risk assessment.
- Rapid clinical improvement: Not typically offered EVT unless there is residual significant LVO and imaging suggests salvageable tissue.
Blood Pressure Targets in Ischemic Stroke Management
Avoid hypotension at all costs, as it accelerates penumbral infarction. For patients not receiving IV thrombolysis/EVT, early guidelines permit observation unless SBP >220 mmHg (with DBP ~110–120 mmHg), at which point gentle reductions (~10–20% over hours) are reasonable. If IVT or EVT is planned or in progress, target <180/105 mmHg while strictly avoiding overshoot hypotension.
-
Recommended agents:
-
- Labetalol, Nicardipine (titrate to avoid overshooting low BP)
- Monitor frequently after reperfusion
Imaging Decision Making in Ischemic Stroke Management
Dr. Lin’s 4 items the ED physician should have ready for the stroke neurologist on the first call:
- Last Seen Normal (LSN) time — the timestamp that starts the treatment clock.
- Exact neurologic deficits, with disability framing and severity (e.g., aphasia, dominant-hand weakness, dense hemianopia).
- Thrombolysis contraindications/bleeding risk — anticoagulation status, recent trauma, bleeding history, structural brain concerns (e.g., tumor, prior ICH).
- Goals of care & premorbid status — baseline function and whether aggressive therapy aligns with values.
Imaging algorithm:
Step 1: Noncontrast CT (rules out hemorrhage)
Step 2: CTA head/neck (identifies large vessel occlusion, tandem/distal lesions, dissection)
Step 3: Advanced imaging in 6–24hr or wake-up scenarios or unclear presentations (CT perfusion, multiphase CTA, MRI) assesses penumbra, collateral flow, infarct core size
CT and CTA Findings
In the 0–6 h window, non-contrast CT (exclude hemorrhage) plus CTA generally suffices for IVT eligibility (when otherwise indicated) and EVT selection (when LVO present). In the 6–24 h window, selection is based on advanced imaging (e.g., CTP, multiphase CTA collateral assessment, or MRI DWI–FLAIR mismatch) to demonstrate salvageable tissue. Order the right CTA: a stroke-protocol multiphase CTA (now) is distinct from a carotid/stenosis-oriented CTA (later). Make sure your requisition triggers the stroke pathway, not “see-you-tomorrow” imaging.
Pitfall After Clean CT/CTA
A “perfectly normal” NCCT/CTA does not exclude ischemic stroke—particularly lacunar or early small-core presentations. If the clinical exam indicates a disabling stroke and the time window is treatable, do not withhold IVT thrombolsysis on the basis of a “clean” initial scan; escalate to advanced imaging or MRI and treat the patient, not the first read. Also consider stroke mimics. Early or subtle LVOs can be missed on initial reads, especially with small cores or distal occlusions. If clinical probability remains high (e.g., disabling cortical syndrome), treat the patient, not the preliminary report—escalate communication with radiology and consider repeat or advanced imaging to reconcile discordant data.
Pearls & Pitfalls in the ED Management of Acute Ischemic Stroke
- Don’t anchor on NIHSS—low score can still be disabling (e.g., aphasia).
- Wake-up ≠ too late—they may be more likely eligible near 24 h than witnessed late-presenters; expedite imaging.
- Order the right CTA—stroke-protocol multiphase, not a delayed carotid CTA meant for stenosis.
- “Clean” CT/CTA does not exclude stroke—prioritize clinical phenotype; consider lacunar and escalate imaging.
- Protect the penumbra—avoid hypotension; if treating, keep SBP <180 (DBP thresholds as above); if not treating, intervene only for very high pressures initially.
- Collaterals determine tempo—good collaterals extend the window; poor collaterals collapse penumbra fast. Let imaging guide urgency.
Key take home points for management of disabling ischemic stroke
- Categorize strokes as disabling vs nondisabling to guide action; abandon major/minor NIHSS binary; focus on disability/functional impact
- Disabling symptoms and “last seen normal” are key triggers for acute pathway activation
- Early—≤4.5hr—IV thrombolysis; late—≤24hr—EVT for select patients via advanced imaging
- Wake-up strokes may be eligible—never exclude based on overnight onset; rapid imaging guides decision
- Clinical scoring for LVO triage is quite sensitive—use when imaging/transfer delayed
- Goals-of-care and premorbid status determination are critical for therapy appropriateness; acute intervention never exceeds baseline function
- TNK is at least non-inferior to tPA, with major logistical advantages.
- Contraindications for thrombolysis have relaxed; updated checklists and consultation recommended
- Blood pressure management: target <180/105 when giving IV thrombolysis/EVT, permissive hypertension otherwise; protect the penumbra: avoid hypotension
- Imaging drives clinical pathway—advanced scans required for ambiguous/late-onset cases
References
Core Guidelines and Consensus Statements
- Powers WJ et al. 2023 AHA/ASA Guideline for the Early Management of Patients with Acute Ischemic Stroke. Stroke. 2023;54:e362–e471.
- Smith EE, Schwamm LH, et al. Canadian Stroke Best Practice Recommendations: Acute Stroke Management, 7th Edition (2022 Update). Int J Stroke. 2022;17:832–886.
- Berge E et al. European Stroke Organisation (ESO) Guidelines on Intravenous Thrombolysis for Acute Ischaemic Stroke. Eur Stroke J. 2021;6:I–LXII.
- Campbell BCV et al. ESO–ESMINT Guidelines on Mechanical Thrombectomy in Acute Ischaemic Stroke. Eur Stroke J. 2019;4:6–12.
- Australian and New Zealand Stroke Guidelines Working Group. Clinical Guidelines for Stroke Management 2023. Stroke Foundation; 2023.
Conceptual Framework: Disabling vs Nondisabling
- Demaerschalk BM, Kleindorfer DO, et al. Minor Stroke and TIA: Not Necessarily Benign—Functional Outcomes and Clinical Implications. Neurology. 2020;94:443–455.
- Khatri P, Kleindorfer DO, et al. Defining “Disabling Deficit” in TPA Decision-Making: Insights from the National Institute of Neurological Disorders and Stroke Trials. Stroke. 2020;51:1340–1347.
- Meretoja A, Churilov L, et al. Functional Disability, NIHSS and Decision to Thrombolyze: The Need to Move Beyond Score-Based Dichotomies. Stroke. 2018;49:239–246.
- Lin MP, Edlow JA, et al. Clinical Emphasis on Disability Rather Than NIHSS Thresholds in Acute Stroke Decision-Making. Emerg Med Clin North Am. 2022;40(1):139–157.
- Kim JT, Fonarow GC, et al. Treatment and Outcomes in Patients With Minor Stroke Receiving Intravenous Thrombolysis. JAMA Neurol. 2025;82(3):212–223.
Wake-Up and Unknown-Onset Stroke
- Thomalla G, Simonsen CZ, et al. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset (WAKE-UP Trial). N Engl J Med. 2018;379:611–622.
- Ma H, Campbell BCV, Parsons MW, et al. EXTEND Trial: Thrombolysis Beyond 4.5 Hours Using Perfusion Imaging Selection. N Engl J Med. 2019;380:1795–1803.
- Muir KW et al. Tenecteplase Reperfusion Therapy for Wake-Up and Unknown-Onset Stroke: TASTE Trial. Lancet Neurol. 2023;22:250–261.
- Jovin TG, Saver JL, et al. Wake-Up and Unwitnessed Stroke Patients in Late-Window Thrombectomy Trials: DAWN and DEFUSE-3 Subanalyses. Stroke. 2021;52:1341–1348.
Endovascular Therapy (EVT)
- Goyal M, Menon BK, et al. Meta-Analysis of Randomized Trials of Endovascular Therapy for Acute Ischemic Stroke. Lancet. 2016;387:1723–1731.
- Nogueira RG, Jadhav AP, et al. DAWN Trial—Thrombectomy 6 to 24 Hours After Stroke with Mismatch Between Deficit and Infarct. N Engl J Med. 2018;378:11–21.
- Albers GW, Marks MP, et al. DEFUSE 3 Trial—Thrombectomy for Stroke at 6 to 16 Hours with Perfusion Imaging Selection. N Engl J Med. 2018;378:708–718.
- Jovin TG, Hill MD, et al. ESCAPE-NA1: Neuroprotection and EVT Outcomes. N Engl J Med. 2020;382:711–722.
- Campbell BCV, Hill MD, et al. Tenecteplase Before Thrombectomy for Ischemic Stroke (EXTEND-IA TNK Trials). N Engl J Med. 2020;382:1111–1122.
- Mistry EA, Murthy SB, et al. Endovascular Therapy for Basilar Artery Occlusion: Systematic Review and Meta-Analysis. Stroke. 2025;56:148–159.
Tenecteplase vs Alteplase
- Menon BK, Campbell BCV, et al. ACT (Acute Cerebral Thrombolysis) and DIRECT-TNK Trials: Tenecteplase versus Alteplase for Acute Ischemic Stroke. N Engl J Med. 2025;392:315–327.
- Coutts SB et al. Canadian ACT-QUICKR Trial: Workflow Efficiency and Outcomes with Tenecteplase in Real-World Stroke Systems. Stroke. 2024;55:2602–2613.
- Parsons MW et al. Tenecteplase Versus Alteplase in Ischaemic Stroke: Updated Meta-analysis of Randomised Trials. Lancet Neurol. 2024;23:145–156.
- Berge E, Whiteley WN, et al. ESO Position Statement on Tenecteplase for Ischemic Stroke. Eur Stroke J. 2024;9:78–88.
Imaging and Collaterals
- Campbell BCV, Christensen S, et al. Imaging Selection and Reperfusion Decision Making in Extended Time Windows. Stroke. 2021;52:218–226.
- Menon BK, d’Esterre CD, et al. Multiphase CTA for Collateral Grading and Patient Selection in Late-Window Stroke. Radiology. 2020;296:190–200.
- Saver JL, Goyal M, et al. ASPECTS and Core–Penumbra Mismatch in EVT Cohorts. JAMA Neurol. 2019;76:561–569.
Drs. Helman, Dr. Himmel and Dr. Lin have no conflicts of interest to declare
Now test your knowledge with a quiz.



Question; —– NOAC with in 48 is absolute CI ? will you still consider it …. Also if you dont have CTP will you consider stat MRI more for thrombolysis versus EVT ? — in some hospital for wake up stroke we start the last well known from the time patient woke up ???
Also question how do you manage carotid stenosis ( when do you think this need immediate stenting ??)
When will you startt he patient on AC after TNK — if patient found to be in new A fib?
Do you do dual antiplatelet on all post TNK patients?
Thanks
Great questions! We’ll be covering antiplatelet agents, DOACs and carotid stenosis in part 2 – episode 209 – stay tuned!
We appreciate such detailed updated explanations about ischemic stroke which has made us understand better the goals of care and core principles while managing a stroke patient.
Disabling vs non-disabling is the way we’ve been thinking about stroke at our ED.
The PRISMS and ARAMIS trials really bear mentioning when using the framework of disabling vs non-disabling:
-PRISMS showed that ASA was non-inferior to IVT for non-disabling stroke
-ARAMIS showed that DAPT was non-inferior to IVT for non-disabling strokes
This also is helpful when thinking about low NIHSS strokes especially posterior circulation stroke that typically respond to vestibular therapy. Highly recommend reading some of Kevin Kerber’s publications.
Thanks for your comments Greg. I agree! We’ll be covering non-disabling strokes in the next episode – 209.
Hi !
Thank you for a well constructed episode with lots of good communication gems, as always being mindful of both tertiary centers as well as rural and a good introduction to this way of seeing stroke care. I agree that this is the way to go, IF the evidence for minor stroke was better
I worry still that the foundation upon which this proposed new paradigm lies, is not well supported in the litterature . For strokes NIHSS >5 I guess the NINDS2 and ECASS III trials along with the metaanalysis by Donaldson et al, gives value to Walter Himmels NNT 10 for major improvement and NNT 7 for “some” improvement . As you mention Justin Morgenstern, Ken Milne, Ryan Radecki, Britt Long and others in the Jerome Hoffman school of thought on this topic probably will not agree, but it’s debatable.
when it comes to “minor strokes” I don’t know that there’s ever been a signal towards benefit outside of maybe subgroup analysis and so the paradigm of “disabling Vs not” for this group rest upon a bioplausible, but never in studies proven foundation. The IVT for minor stroke doesn’t care whether it’s disabling or not – but maybe the argument is whether a patient with disabling minor stroke have more to loose and therefore is willing to risk it ?
It might be pedantic , but the reason why I think it’s important is the discussion with the patient and the information that we provide them especially when the stroke is “minor” but disabling as these are the hardest conversations and I worry that the extrapolation from “major strokes” (NINDS / ECASS NNTs) might not apply here
Ref
– Britt Long et al 2025, Intravenous Thrombolysis for Minor Acute Ischemic Stroke
– PRISMS study , Kathri et al 2018 Effect of Alteplase vs Aspirin on Functional Outcome for Patients With Acute Ischemic Stroke and Minor Nondisabling Neurologic Deficits
– First10em https://first10em.com/thrombolytics-for-stoke/amp/
– https://lowninstitute.org/will-it-take-50-100-years-to-get-the-right-answer-about-tpa-for-stroke/amp/
– Milne Vs Lang: CJEM Debate Series: #TPA should be the initial treatment in eligible patients presenting with an acute ischemic stroke
– Tempo 2 trial – Zhang et al Thrombolysis With Tenecteplase for Minor Disabling Stroke Secondary Analysis of the TEMPO-2 Randomized Clinical Trial
Hi Peter,
Thanks for the thoughtful and important question!
I’ll take a moment to weigh in here since we didn’t have the time to dig in during the episode itself, but I think it’s a crucial question to address. Also welcome Walter and others’ to share their thoughts/perspectives, too!
In all honesty, this is a question that I grappled with for years as I was going through my stroke training. And it was such a big topic with so many strongly dissenting opinions, that I hesitated to tackle it head on during my training years and early transition-to-staffhood career, as I wasn’t sure I could do it justice.
I also fully agree that the “disabling minor stroke (NIHSS <5” is one of the hardest decisions/conversations to have in the clinical environment.
But here are my reflections, and the reason why I stand behind the utility of thrombolysis (with either alteplase or Tenecteplase) as an acute stroke treatment in disabling stroke presentations (whether major or minor on the NIHSS scale):
• The trials on “thrombolysis in minor stroke” that have come out in recent years (including ARAMIS, TEMPO-2, etc) all focus on NON-disabling minor strokes, and there are no dedicated trials on thrombolysis in DISABLING minor strokes, so as Peter pointed out, we can only extrapolate from other datasets, including the original landmark trials (NINDS/ECAS-3) and also a body of observational trial and registry data that we have accumulated over the past 20 years in the interim. Although there are no dedicated trials looking at this patient subset, we do have much more safety and outcome data now than we did 20 years ago thanks to the creation of stroke registries that track ALL acute treatments in some jurisdictions (the Alberta-based QuICR registry is an example of one of the largest stroke registry datasets that tracks both thrombolysis and EVT outcomes for all reperfusion treatment cases).
• I am not a trialist/primary investigator, so I can’t comment on the logistical feasibility of us ever getting another landmark RCT looking at thrombolysis vs standard medical therapy in disabling stroke patients, but I can state with confidence that our understanding of patient selection for treatment has come a very long way in the past 20 years since NINDS/ECASS-3 were first published. Not only is neuroimaging better/more advanced (eg. improved resolution overall for CT/CTA, but also advanced imaging such as multiphase CTA, CT perfusion, and fast stroke MRI protocols), but our understanding of how to appropriately select patients based on imaging and case features has come a long way as well. For many years now, the stroke neurology world has shifted more heavily towards imaging-based treatment selection (rather than purely time-based treatment), since we know that benefit vs risk of any reperfusion therapy (whether thrombolysis or EVT) are heavily impacted by: 1) overall established infarct/core size, 2) clot characteristics for reperfusion success (size, length, location, and hardness/composition of clot), and 3) the quality of collateral blood supply (every patient infarcts at a different rate, even with the same clot, due to variations in individual collateral blood flow/anatomy).
• Notable observational and registry data supports the role that thrombolysis plays in early recanalization, and that is the primary mechanism by which we limit or stop permanent ischemic damage (ie. limit the size of infarct core growth over time). We see a time-dependent impact on neurologic outcomes (eg. mRS) as well as mortality and symptomatic ICH (sICH) outcomes. The earlier that recanalization is achieved by any means, the better patient outcomes are and the lower the risk of sICH. The observational/registry data we have accumulated over the past 20 years since NINDS/ECASS-3 supports that early thrombolysis is better than medical therapy or antiplatelet therapy alone for early recanalization, 90-day neurologic outcomes, and mortality (see ref list).
• Thrombolytic bridging RCT’s in the stroke literature (eg. studies looking at thrombolysis before EVT in patients with large vessel occlusions, LVO) have shown better outcomes (90-day MRS and mortality) among patients who receive thrombolytic treatment before EVT. Given the overwhelming data in support of EVT efficacy for LVO, I find this bridging data highly compelling to support that patient selection is really the key driver for thrombolytic advantage. In these favourably selected patients who proceed to EVT, even with the large clinical effect size and NNT=4 of EVT itself on stroke outcomes, nonetheless we STILL see benefit from thrombolytic therapy in these patients. I suspect this may be the closest we get to modern thrombolytic RCT data using patient selection as a key driver. I have not seen the thrombolytic skeptics address this point yet.
• There have also been RCT studies published more recently on thrombolytic use in the late window period (up to 24 hours), but focusing on patient selection as a key inclusion criteria, and demonstrating that with appropriate patient selection, even these late-window thrombolytic patients receive benefit. Again, this highlights for me that the key driver of treatment success is actually appropriate patient selection.
• Additional data also shows that sICH risk with thrombolysis is NOT the same from patient to patient, and varies based on 1) infarct/core size, and 2) clot characteristics (length/location/composition). So a patient with a favourable CT (ASPECTs score 8-10) will have a much lower overall sICH risk than the standard 3-5% that is quoted from the NINDS/ECASS-3 studies (data would suggest as low as 0.5% or less for some small posterior circulation and lacunar strokes or strokes with favourable ASPECTS score of 10). Conversely, patients with unfavourable imaging features likely have a much higher sICH risk than the standard 3-5%. But it is challenging and nuanced to put all those pieces together, and impractical to build system-level protocols on this. So I think the collaboration between front-line clinicians and accessible stroke expertise is crucial for ensuring proper patient selection and consent based on individual case-by-case features.
• Not all centers with CT-capability have angiography (CTA) to visualize the clot, so with a hyperacute disabling stroke presentation with a favourable non-contrast CT, we cannot always know at the time of thrombolytic treatment decision-making whether the patient has a small vessel occlusion that would NOT be amenable to EVT (eg. a lacunar syndrome), so we may miss an intervenable window if we do not act quickly. And even with LVO candidates, if there is significant transport time involved to get to an EVT-capable centre, up to 15-30% of EVT cases are unsuccessful in the end (eg. unable to access the clot due to anatomy, unable to clear the clot due to clot composition/density, complications during the procedure, etc), so again you may miss an intervenable window when the patient may have had a better chance to receive early reperfusion.
• And finally, qualitative studies exploring patient perspectives cannot be forgotten here. Patients themselves, when asked what they would choose between a chance at reducing or reversing disabling symptoms versus the quoted increased risk of potential sICH and/or death, overwhelmingly choose the risks of treatment for that better chance at quality of life on the other side of stroke.
All that to say: between the thrombolytic bridging to EVT RCT data, late window thrombolysis RCT data, stroke registry data, and qualitative patient-focused survey data, I think that patient selection is at the heart of modern stroke treatment with both thrombolysis and EVT. I think that is the true game-changer of acute stroke treatment outcomes over the past 20 years. Truly understanding the severity of disability for the individual patient (eg. complete aphasia is not the same as moderate slurred speech; complete hemiparesis is not the same as facial droop with mild to moderate arm weakness, etc) and having access to collaborative stroke expertise to appropriately select for treatment eligibility are key. And if I were ever faced with disabling enough symptoms myself (irrespective of NIHSS severity score) and was eligible for treatment, I would choose thrombolysis.
Thanks again for tuning in and for the thoughtful discourse!
References below (I do have more, but didn’t want to go overboard):
Refs:
• Al-Ajlan et al. Golden Hour Intravenous Thrombolysis for Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Ann Neurol. 2024 Sep;96(3):582-590
• Ghaith et al. Intravenous thrombolysis before mechanical thrombectomy for acute ischemic stroke due to large vessel occlusion; should we cross that bridge? A systematic review and meta-analysis of 36,123 patients. Neurol Sci. 2022 Nov;43(11):6243-6269
• Kaesmacher et al. Time to Treatment with Intravenous Thrombolysis Before Thrombectomy and Functional Outcomes in Acute Ischemic Stroke: A Meta-Analysis. JAMA 2024;331(9): 764-777.
• Seners et al. Incidence and Predictors of Early Recanalization After Intravenous Thrombolysis: A Systematic Review and Meta-Analysis. Stroke. 2016 Sep;47(9):2409-12.
• Terreros et al. Early recanalization in large-vessel occlusion stroke patients transferred for endovascular treatment. Neurointerv Surg. 2022 May;14(5):480-484
• Zhu et al. Prediction of recanalization in acute stroke patients receiving intravenous and endovascular revascularization therapy. Int J Stroke. 2015 Jan;10(1):28-36
• Seners et al. Post-Thrombolysis Recanalization in Stroke Referrals for Thrombectomy: Incidence, Predictors, and Prediction Scores. Stroke 2018 Dec;49(12):2975-2982
• Broocks et al. Investigating Neurologic Improvement After IV Thrombolysis: The Effect of Time from Stroke Onset vs Imaging-Based Tissue Clock. Neurology 2023 Oct;101(17):e1678-1686
• Ebinger et al. Association between dispatch of mobile stroke units and functional outcomes among patients with acute ischemic stroke in Berlin. JAMA 2021 Feb;325(5):454-466
• Denier et al. Thrombolysis in stroke patients with isolated aphasia. Cerebrovasc Dis 2016;41(3-4):163-9
• Campbell et al. Extending thrombolysis to 4.5-9h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data. Lancet 2019;394(10193):139-147
• Ciccone et al. Thrombolysis for acute ischemic stroke: the patient’s point of view. Cerebrovasc Dis. 2001;12(4):335-40
Hi Dr. Lin,
Thanks so much for taking the time to write a follow-up to the episode. I appreciated the importance of understanding disability beyond the NIHSS.
I wanted to add one perspective to the discussion, coming from the angle I’ve been exploring in my own work recently. While I agree completely that some patients with minor scores can have meaningful or even life-changing deficits, I still struggle with the fact that we simply don’t have randomized data identifying which specific minor-stroke patients actually benefit from thrombolysis.
As you pointed out, the recent RCTs — PRISMS, ARAMIS, TEMPO-2 — all enrolled “non-disabling” patients. But even outside of the minor-stroke space, the overall thrombolysis literature is surprisingly inconsistent. Across the broader IVT trials there are positive, negative, and even harmful studies, and the two “landmark” positive alteplase trials have been criticized for serious baseline imbalances and fragility. Even the trials to extend the time window using imaging criteria aren’t uniformly positive and often have confidence intervals that approach one. When a therapy’s foundational evidence is mixed, I get nervous about extrapolating benefit to a new population without randomized data to support it. (You specifically note a benefit in trials of thrombectomy patients randomized to IVT vs thrombectomy alone; however, these trials are not uniformly positive and the NIHSS of these patients is usually around 16 so this doesn’t move the needle for me on patients with minor strokes.)
That’s really the heart of my hesitation. I don’t doubt that some patients with minor strokes and specific deficits may benefit — I actually suspect they exist — but right now we don’t know who they are. And because most minor-stroke patients start with low modified Rankin scores, it’s inherently harder to demonstrate functional improvement in this group. Without RCTs targeting the “disabling minor stroke” population specifically, we’re left making assumptions, and assumptions in stroke care have burned us before.
At the same time, the resource implications keep growing. Over the last decade, stroke codes have surged, imaging has skyrocketed, and more and more low-NIHSS patients are being funneled into hyperacute pathways. If IVT isn’t actually helping the majority of these patients, it’s worth reconsidering the threshold for treating them until we can more precisely identify true beneficiaries.
So I completely agree with you that patient selection is key — I just think we’re overdue for randomized trials that help us figure out which patients with “minor” scores but potentially disabling symptoms truly benefit from thrombolytics. Until then, I lean toward a more conservative, evidence-based approach, while still acknowledging that gray areas will always exist. A reoccurring theme in the history of medicine is one where we broadly adopt therapies based on flawed evidence then have to backtrack once we realize that these therapies don’t work.
Really appreciate the conversation and the thoughtful dialogue. These are exactly the kinds of discussions that move the field forward.
Warmly,
Rich Childers
Yes yes minor non disabling stroke..
What when that stroke progresses to disableling stroke and you are out of the windows by then?
And yes it happens, and this i saw patients leaving disabled thst got no agressive tberapy