
Written by Navpreet Sahsi; edited by Hiren Patel, Matt Douglas-Vail and Anton Helman, November, 2022
Hi, we are Navpreet, Hiren and Matt, from EM cases Global Emergency Medicine. We are very excited to start this new series with our Canadian colleagues. Our goal is to review high yield core concepts in global emergency medicine, discuss global health experiences from Canadian emergency doctors and introduce ways that you can get involved in global emergency medicine.
Our first post is from one of our co-editors, Navpreet Sahsi where he shares his unique experience as one of the few Emergency Doctors practicing in the first and only Emergency Center in Bangladesh with the ICRC.
Salam! (Hello in Bengali).
I am Navpreet Sahsi, Emergency Physician at North York General Hospital in Toronto. Last winter as COVID pandemic restrictions were easing and travel became a possibility, I sought an escape from the daily grind. Having worked for medical NGOs such as Doctors Without Borders/MSF many times before, but not for several years, I yearned to return to “the field” where I felt my skills could be used to serve a population in need. This time I signed up with the International Committee of the Red Cross (ICRC) and accepted a project in Cox’s Bazar, Bangladesh.

Bangladesh is one of the most densely populated countries in the world, with a population of approximately 171 million and a landmass about the same size as New Brunswick (1). While it has seen rapid growth more recently, over 20% of the population lives below the poverty line, living on less than $5 a day (2). I worked and lived in Cox’s Bazar, a densely populated city that stretches along the Bay of Bengal. Within it lies the world’s longest sea beach, across which you’ll find luxury beach hotels and local tourist hot spots, juxtaposed with the world’s largest refugee camps. There presently exist an estimated 1 million Rohingya refugees in the camps (3). The population rapidly increased in 2017 as they fled persecution in Myanmar and the crisis remains unresolved. When visiting the camps there is a viewpoint upon which one sees a never ending expanse of shanty housing and tents stretching to the horizon. It was heartbreaking to see and will be forever etched in my mind.

Credit: UN Women/Allison Joyce
As a Canadian living in Cox’s Bazar my daily experience felt quite chaotic. Getting around can often mean pushing your way through large crowds, crammed amongst strangers where the sense of personal space was completely lost. Traffic was absolutely insane: cars would move in any and all directions with little rules or regulations. No matter where you are, or the time of day, Cox’s Bazar was a cacophony of noise, and people.

I was working with the ICRC to build capacity in the largest (and only) emergency room in Bangladesh, in Cox’s Bazar’s Sadar Hospital. Emergency Medicine does not exist in Bangladesh. Not as a concept, and certainly not in the way we think of Emergency Medicine in North America. There is no formal training program, and it is not a recognized specialty; it is almost totally unavailable, and there is little to no infrastructure to accommodate it in the field or in the hospital.
Prior to the ICRC’s intervention the “Emergency Department” was just one room with a desk and a bed, limited equipment, and staffed by a government doctor, with one or two years of postgraduate training, and no formal Emergency Medicine training. If you arrived at the hospital, you would typically fight (or bribe) your way through a large and disorganized crowd to see the doctor; there was no triage. And if you miraculously made it through, the doctor would look at you, and based on this would assign you to a floor on the hospital where you would possibly see a specialist, (if it was daytime) and if lucky, get some medical care. Pregnant patients – to the OB ward, children – to the Pediatrics ward, etc. If you were critically ill from hemorrhagic shock you certainly would not receive any interventions in the ER. The ER was too under-equipped, understaffed and undertrained to intervene.
Sadar Hospital is the only public hospital in a city holding the world’s largest refugee camps. Public hospitals are free in Bangladesh. There are many private hospitals as well, however they are largely inaccessible to the majority of the population due to high fees. It is no wonder that the ICRC saw an opportunity to intervene. The project started in 2017, and since then the one bedroom, one desk emergency room has been slowly transformed into something resembling a real Emergency Center. It now has twenty beds, with cardiac monitors, a resus area, a trauma bay and ten beds for “intermediate” patients.

The resuscitation bay

The “intermediate” ward
However, there is much more to an emergency room than infrastructure. In North America, the transformation of Emergency Medicine had its origins the 1960’s. It has taken decades to evolve and become the specialized training that we know today. In 2022, Emergency Medicine in Bangladesh more closely mirrors those early days of the 1960’s. Creating a new medical culture in a country lacking resources does not come quickly or easily.
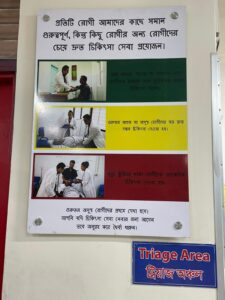
Initial steps in developing an Emergency Department in Bangladesh
The first task was to institute triage. This was a challenge, as it needed to be implemented in a hospital and country where it was a completely new concept. Using a validated tool in low resource settings, the Intra-agency Integrated Triage Tool (IITT) was slowly introduced over months and both patients and staff were trained its principles (4). As one can imagine, in a country where money and power often dictate care, this was not accepted easily at first. It took months of education to change patient perspective, hospital structure and flow. The second step was to train staff using the ICRC’s standard course in Basic Emergency Care. (BEC). Through this course, doctors and nurses were taught basic systemic approaches to the assessment and management of critically ill patients. Emphasis was on rapid intervention and standardized management of time-sensitive presentations such as shock, altered mental status, etc. As a result, Sadar hospital presents a model for formalized structure and standardized emergency care for the country. It has gained national recognition and attention from the government who hope to replicate the model and bring it to other parts of the country.
 Although this model seems promising, and definitely demonstrates progress in the right direction, as we know, emergency care is a lot more intricate and complicated than just providing structure and training. The famous saying “build it and they will come” holds true for Sadar Hospital, the only public hospital providing emergency care in a city overcome by refugee camps.
Although this model seems promising, and definitely demonstrates progress in the right direction, as we know, emergency care is a lot more intricate and complicated than just providing structure and training. The famous saying “build it and they will come” holds true for Sadar Hospital, the only public hospital providing emergency care in a city overcome by refugee camps.
The emergency center now sees an average of 300-400 patients per day, over half of which would be classified as high acuity or CTAS 1 or 2. There is only funding for two government doctors during the day – they are overworked and underpaid and as such they are still dependent on ICRC support. The ICRC funds a third clinician as well as a foreign “expert”, which in this case was me.
How does Emergency Medicine in Bangladesh compare to North America?
Well, take your busiest acute shift in North America and multiply it by twenty and you can begin to imagine what a day in Bangladesh is like. It is often very chaotic and the acuity is unreal. In one day in the ED, I would see more critically ill patients than I would see in an entire year back home.
It is interesting to see what a challenged public health system can shape the demographics of critically ill patients. The majority of acute patients were children, often infants or neonates born at home, obstetric emergencies (eclampsia, PPH, deliveries), and seldom were there drug or psychiatric related illness. Interestingly, the large majority of toxicology cases were organophosphate ingestions. Severe chronic illness is rare as people do not live long enough to develop them, and the majority of the burden of illness is trauma related. Head traumas, chest traumas, limb amputations – you name it. Mostly related to MVCs, but of all sorts.
My biggest frustration, which was also a common frustration amongst my colleagues, was the lack of around-the-clock care. Given that this was a public hospital there is little financial incentive for specialists to see public patients after work hours (which are about 8-2 pm). Specialists often leave the hospital to work in private settings and were very hard to reach. If your patient needs emergency surgery at 3 pm you will have to wait until the next morning. Imagine resuscitating patients in the ED only to see them left to die time and time again. Often our only option was to send them to the “tertiary” care public hospital, which was about 8-9 hours away and in an unstaffed, ill-equipped “ambulance” without a siren.
How did I try and see the silver lining in the midst of the massive challenges of Global EM?
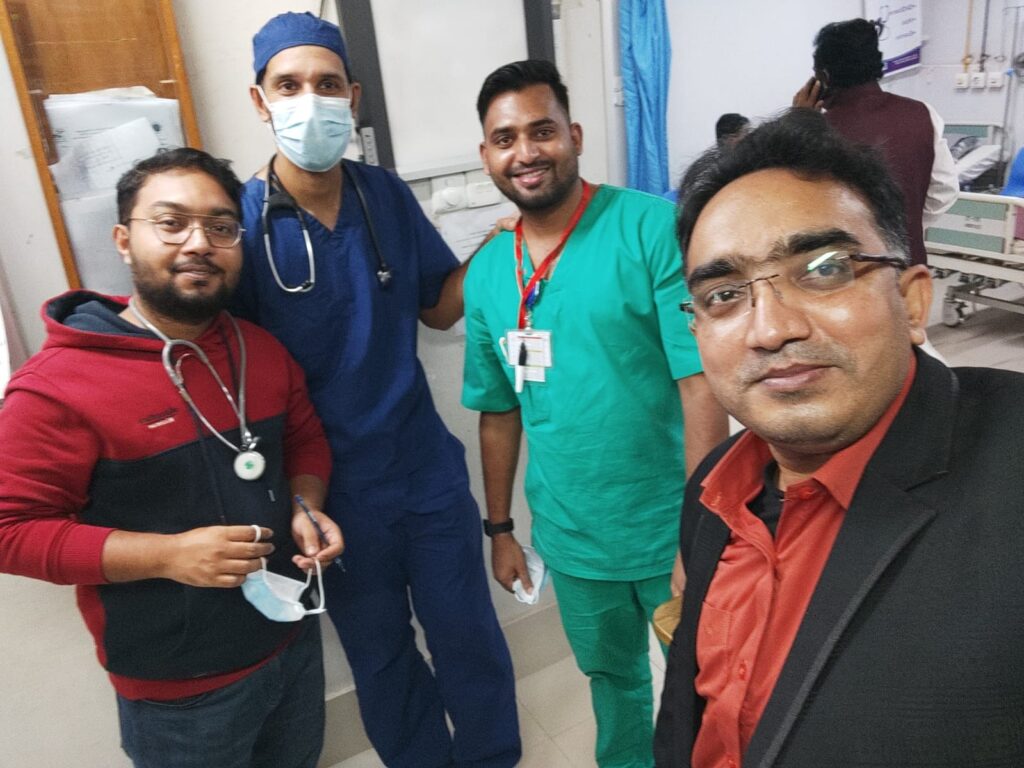
I mostly tried to teach my colleagues to do what EM doctors have done everywhere: work together to help the most vulnerable and hold the health care system up on our back by providing the best care we can to everyone, at all times of day, regardless of caste, religion, race, gender, or income level. I tried to do the best to manage the cases I saw with what I had, teach what I could, was creative when I had no equipment and advocated when they had no voice. Sometimes we saved lives and many times, I saw miracles. I drilled burr holes in unconscious patients to see them wake up and watched patients recover from almost certain death. I felt that my primary responsibility was simple: to be present with my colleagues and provide support and encouragement; to remind them that the job they were doing and the difference they were making was incredible, even if it did not always feel like it.

The “burr hole” – 13 year old boy, with full neurologic recovery post epidural hemorrhage drainage.
At the end of the day, did I feel I made a difference working as an Emergency Physician in Bangladesh? Does practicing Global EM make a difference?
The short answer is “yes”. Sure, the context is complex and you can not be certain that the short time you spend working in Global EM is making a sustainable impact. Nonetheless, you hope that the few things you taught, the few people you inspired, and the few protocols you put into place were some small steps towards changing the status quo.
I found my time in Bangladesh with the ICRC a nice reprieve from my work in Canada. The COVID pandemic had left me feeling drained and uninspired. Being fully engrossed in challenging and meaningful work in a foreign context helped rekindle my love of Emergency Medicine. We have so much to offer. It brought me great pride to contribute my Emergency Medicine skills and knowledge to the furthering of health care across the globe. In the three months I spent there I learned the challenges of trying to bring Emergency Medicine to a part of the world where it did not exist before, the difficulties of caring for critically ill patients in a limited resource setting, and was reminded of the complexities and joys of working in a new and foreign context. I am back at home now in Toronto, and every day I reflect on how fortunate I am to live in a country where emergency care is not something I have to fight for – that emergency care is top notch, accessible to all, and a right. I hope this soon becomes a reality as well for the people of Bangladesh.
Disclaimer. This blog post is a personal report of my own experiences and certainly does not represent the entirety of a complex medical situation in a very diverse country or the work of the ICRC.
References
- Macrotrends: Bangladesh Population 2022 (n.d). https://www.macrotrends.net/countries/BGD/bangladesh/population
- Asian Development Bank – Poverty Data: Bangladesh (n.d.) https://www.adb.org/countries/bangladesh/poverty
- OCHA: Rohingya refugee crisis (n.d.) https://www.unocha.org/rohingya-refugee-crisis
- Michell et al. Validation of the Interagency Integrated Triage Tool in a resource-limited, urban emergency department in Papua New Guinea: a pilot study. The Lancet. VOLUME 13, 100194, AUGUST 01, 2021



Leave A Comment