
This is EM Cases Episode 98: Teaching on Shift.
As if EDs weren’t chaotic enough, many of them are staffed by a revolving door of medical learners. Yet, to each of these learners, the ED doc has a critical responsibility: To teach. This is a central tenet of what we do, and has been since the days of Hippocrates teaching his two sons. To some, it comes intuitively, to others, it’s the most difficult part the job. Either way, we can all use some teaching on how to teach.
Gone are the days of see one, do one, teach one. By analogy, learning the skills of effective teaching on shift isn’t dissimilar to learning how to put in a central line. It takes thoughtful preparation, knowledge and practice. In this episode, with the help of two master educators, Amal Mattu and Rick Penciner, we cover the how, the when, and the why we teach. We discuss some quick, easy tips on how you can take your educating skills to the next level, from orienting the learner and establishing expectations at the start of the shift, to key questioning techniques to use in case presentations, to the lost art of active observation, to the One Minute Preceptor model, to giving effective end-of-shift feedback, medicine’s white whale. We end with a surprise appearance by another master educator who gives his top pearls on teaching on shift. This podcast is about how, on your next ED shift, you can make the most of every teachable moment…
Podcast: Play in new window | Download (Duration: 1:17:36 — 71.1MB)
Subscribe: Apple Podcasts
Podcast production by Anton Helman, Andrew Cameron and Rick Penciner,
Written Summary and blog post by Alexander Hart and Shaun Mehta,
edited by Anton Helman and Rick Penciner July, 2017
Cite this podcast as: Helman, A, Mattu, A, Penciner, R. Teaching on Shift. Emergency Medicine Cases. July, 2017. https://emergencymedicinecases.com/episode-99-highlights-emu-2017/. Accessed [date].
Meeting the learner
There are a few key steps that our experts recommend prior to seeing patients on shift: orienting the learner, setting expectations, diagnosing the learner and priming the learner.
Orientating the learner: Learn about your learner.
Ask your learner some background questions like what program they are from, their level of training and experience, previous clinical experiences and their special interests. What do they hope to learn from you? What areas of medicine do they find difficult or confusing? What skills do they want to practice? Explain their role in the department, patient flow, and what work needs to be done.
Setting expectations: A mutual relationship.
Discuss the learner’s responsibility during the shift and encourage them to ask questions. Tell your learners that you will act like a coach helping them to fine tune their skills. Lay out your expectations for case presentations, encouraging them to commit to a plan, clear charting and that you will be providing feedback during and at the end of the shift. Let them know that you assess them by direct observation by listening in to their interactions with patients and staff.
Diagnosing the learner: Understand and tailor their experience.
One of the most common pitfalls is to teach based on a poor understanding of the learner and their needs. Teaching at a level of understanding greater or less than that of the learner is unproductive, frustrating, or both.
Once you get a sense of your learner, you can better teach at a level appropriate for them. There are 4 types of learners:
- Unconsciously incompetent
- Consciously incompetent
- Consciously competent
- Unconsciously competent (ie. staff/attending)
Priming the learner: Prepare them for success.
Encourage your learner to review the chart before going into a patient’s room. Ask them to generate a differential diagnosis for the triage complaint. Consider starting inexperienced students with more straightforward cases.
Case presentation teaching strategies
The most important concept in being an effective teacher during case presentations is to listen more, and talk less.
Our role as teachers in the ED is to facilitate learning. Listening to our learners will prompt what we teach. We should approach teaching opportunities more like coaches and less like lecturers. Some tips for achieving this:
- Give the learner your full attention – avoid multi-tasking during case presentations
- Minimize interruptions – don’t interrupt or correct too early; the ideal presentation is one that is not interrupted too often – interruptions may confuse the learner and are often seen as criticisms of their presentation
- Inform the student of expected length for presentations up-front
- Allow the learner to arrive at the diagnosis themselves
- Encourage the learner to present in a way that “makes their case” – it is important for students to learn to present in a manner that “makes the case” for their diagnosis rather than in the same order in which they collected the data
- Taking away the chart from the learner while they present in order to force them to tell a story rather than read through a case
Focus on one teaching point for each patient.
One of the biggest pitfalls in clinical teaching is to try to teach too much.
The One Minute Preceptor model
The one minute preceptor model allows for time-efficient teaching with well-studied impacts on learning.

Adapted from Aagard, Teherani, Irby; Academic Medicine 2004
Getting all that in in 1 minute can be challenging. The key however should always be to reinforce the first skill – get a commitment! Get them to to commit themselves to an opinion about the diagnosis or about investigation or management. If you are unable to get a commitment on what the most likely diagnosis is, get the learner to commit to what needs to be ruled out and rank by deadliness:
- What will kill the patient in the next few minutes
- What will kill the patient in the next few hours
- What will kill the patient in the next few days
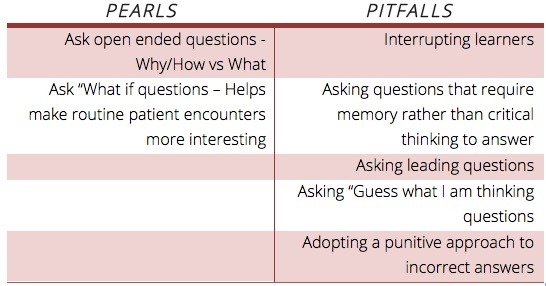
Questioning Techniques
The most important thing to remember when questioning learners is ‘wait time’: Wait 3-7 seconds for the learner to answer.
The average amount of time faculty allow a student to answer a question is about 1 second. Increasing wait times for answers will significantly increase the number of student responses. Divergent as opposed to convergent questioning is more effective in facilitating active learning. Examples include: What do you think is going on with this patient? What else could be going on? How did you reach that conclusion? What’s the evidence for that conclusion? What else could it be? What do you think we should do next? How would you explain that to the patient?
The manner in which we ask questions of our learners can have a significant impact on how much information they are able to retain from a given encounter.
Dr. Mattu’s “What if” teaching tip
If the patients aren’t interesting, make them interesting artificially by asking “ What if……?” For example, if the learner presents an otherwise healthy patient with a simple cellulitis ask the learner “what if this patient with cellulitis was an IV drug user, was febrile and appeared septic?” and “what if this the patient was on their third round of antibiotics with no improvement?”
Active Observation
It is often difficult to interact with or assess a learner beyond the case presentation. Observing full H & Ps, monitoring bedside manner and supervising procedures can be time consuming. Sampling observation is a strategy that is time efficient and can give you a broader scope of a learner’s skills. Try:
- Listening to a history through the curtain
- Watching certain parts of a procedure
- Prompting the learner to elicit a specific sign on physical exam
- Asking the learner to deliver instructions to the patient
Whiteboard teaching, sniper rounds or post-it pearls
Whiteboard teaching, sniper rounds or post-it pearls, gets your learner to write down one key learning point per patient on shift. These are a sure-fire way to maintain their engagement, promote on-shift teaching amongst your colleagues and ensure you never take a shift off when it comes to education. Your learner may also benefit from asking them to write down the 3 most important pearls they learned at the end of the shift.
Follow Dr. Mattu’s #WhitboardTeaching on Twitter
Michelle Lin’s description of post-it pearls on ALiEM

Example of Post-it Pearls care of Academic Life in EM blog
Teaching on shift procedures
When it comes to teaching procedures, we have moved beyond the see one, do one, teach one framework.
Teaching procedures is a 3 step process:
- Conceptualization – why do the procedure, risks/benefits etc
- Visualization – observe the teacher do it, watch a video, visualize in your mind before doing it
- Verbalization – verbalize what you are doing as you do it and have the learner verbalize what they are doing as they do it
Break down the procedure in to small digestible steps. It is important to correct mistakes as they are made rather than waiting until the end of the procedure both for increasing the impact of learning from that mistake and for patient safety. It is better to stop the error before it is imprinted into the motor memory.
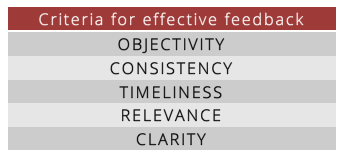
Giving feedback when teaching on shift
Giving honest and helpful feedback can be challenging, however, of all the techniques a teacher can use, feedback has the greatest effect on learning. Studies show that medical teachers over-estimate the amount of feedback given while learners feel that they don’t get enough feedback. Feedback should be giving often throughout the shift, not only at the end of the shift. The timing of the feedback is important: Time feedback as close to a performance as possible so that you and your learner can still remember the details of what happened. Give feedback that is actionable.
Our experts have a few pointers to help you give the learner effective end of shift feedback.
- Define it – feedback is information that highlights the difference between the actual and intended results.
- Frame it – have a common understanding that this information is given to improve future performance and enhance success.
- Label it – announce to your learner that you are giving them feedback.
- Take it – allow some time for your learner to give you feedback about your teaching.
When you are setting expectations at the beginning of the shift, let your learner know that you will tell them what they did well and a few things they should work on. This strategy will allow the learner to effectively retain what they received feedback on as well as better handle any negative connotations of constructive suggestions.
If in doubt, use the following template for your next feedback session focusing on behaviours and areas that the learner can control and modify rather than personality traits.
- Listen to self-evaluation first (use this self-evaluation to customize your feedback)
- Discuss and validate what was done right and they should continue doing
- Discuss what needs starting, stopping or improving
- Decide what to do next time – a ‘recognizable action’
- Provide clear instructions and support for improvement – teach ‘pearls’ and ‘general rules’
- Ask the learner to summarize the feedback and plan
Avoid the “Sacket Sandwich”
The classic teaching for giving feedback has been to sandwich constructive criticism between points of praise. This strategy is problematic because learners expect it and tend to lose the value of any ‘negative’ feedback.
![]() Update: For a detailed script of simulation style debriefing applied to everyday ED feedback and coaching. Link
Update: For a detailed script of simulation style debriefing applied to everyday ED feedback and coaching. Link
The Wrap Up
At the end of the shift wrap up the teaching by:
- Asking the learner to tell you the three most valuable pearls or pitfalls that they learned on the shift
- Encouraging the learner to follow up on cases
- Suggesting resources for them to learn more about topics they identified as needing improvement during the shift
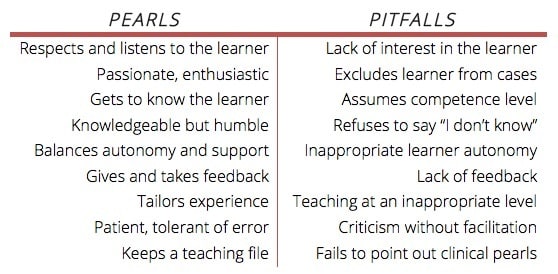
Qualities of a great teacher
The best teachers often have indefinable qualities that make them great.
The most important quality of a great teacher is enthusiasm.
Pearls and pitfalls of teaching (adapted from ED-STAT)
EM Cases Quote of the Month
“In the hurly-burly of to-day, when the competition is so keen…it is well for young people to remember that no bubble is so iridescent or floats longer than that blown by the successful teacher.”
-Sir William Osler
Drs Helman, Mattu and Penciner have no conflicts of interest to declare
References:
- Irby DM, Bown JL. Time-efficient strategies for learning and performance. The Clinical Teacher. 2004;1(1):23-28
- Kurth RJ, Irigoyen M, Schmidt HJ: A model to structure student learning in ambulatory care settings. Academic Medicine. 1997;72:601-606.
- Norcini J: The power of feedback. Medical Education. 2010;44:16-17.
- Aagard E, Teherani A, Irby DM: Effectiveness of the One-Minute Preceptor Model for Diagnosing the Patient and the Learner: Proof of Concept. Academic Medicine 2004;79(1):42-49.
- Reilly BM. Inconvenient truths about effective clinical teaching. Lancet. 2007;370(9588):705-11.
- Rogers, R. L. (2013). Practical teaching in emergency medicine. Chichester, West Sussex: Wiley.
Other FOAMed Resources on Teaching on Shift
Teaching when there is no time on EMDocs



Dr, Helman,
Thank you for your podcast series. As an ED nurse, I view it as a great resource. While I’m not involved in medical education, I liked Dr Mattu’s approach to learners where he wants them to understand what causes for a complaint might kill the patient in minutes, hours and days- it’s a line of thinking I’m adopting in my practice.
Dr Mattu also mentioned the value of a “5 minute consult” reference. After skimming back through the episode, I was unable to determine if there is a particular reference he (and you) recommends. So, which do you recommend? I’m aware of the Rosen and Barkin version- is that the best (in your opinion)?
Thank you for your time and extremely helpful podcasts,
Ben, RN
“