
In this ECG Cases blog we look at 5 unstable patients with bradycardia and elucidate our BRADIcardia mnemonic. Will the ACLS algorithm work, or does systematic 12-lead ECG interpretation help improve diagnosis and treatment?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. October 2025
Five unstable patients presented with bradycardia. Will the ACLS algorithm work, or will systematic 12-lead ECG interpretation improve diagnosis and treatment?
Case 1: 90yo with weakness, BP 90
–
Case 2: 60yo with weakness and lethargy, BP 80
–
Case 3: 60yo with chest pain, BP 100
–
Case 4: 40yo with sudden collapse, GCS 7, BP 170/110
–
Case 5: 90yo, AF on beta-blocker, with few days of weakness and increasing lethargy, BP 80
–
ACLS pitfalls: unstable patients with bradycardia and the BRADIcardia mnemonic
This is the first in a series of posts on the pitfalls of ACLS arrhythmia algorithms for adults with a pulse, and how systematic approach to the 12-lead ECG can improve ECG acquisition, interpretation, and application.
ACLS was first created to treat post-MI arrhythmias en route to the CCU. In other words, patients with a known underlying cause developed a sudden arrhythmia, and the arrhythmia itself determined stability and treatment. Over the years ACLS has become the default approach to any acute arrhythmia, but this doesn’t always apply to undifferentiated patients in the emergency department. For arrhythmias in adults with a pulse, ACLS algorithms provide a good foundation: by assessing patient stability and stratifying QRS by fast vs slow (and narrow vs wide for tachycardias), they rapidly target cardiac conduction with medication or electricity. But this simplified approach relies on assumptions, which can lead to pitfalls:
- ECG acquisition: ACLS assumes the ECG has been properly acquired, but artifact can mimic arrhythmias
- ECG interpretation: ACLS uses rhythm categories based only on the QRS complex in the rhythm strip (the 1-lead ECG), without identifying the specific arrhythmia or secondary causes. The algorithms say to get a full 12-lead ECG, but not how that helps improve interpretation
- ECG application: ACLS is designed for primary arrhythmias, where the rhythm itself causes instability (ie. an electrical problem with an electrical solution), not secondary arrhythmias with a reversible underlying cause that may determine instability and require treatment. The algorithms say to find and treat the underlying cause, but not how the 12-lead ECG helps do that
For unstable patients with bradycardia, ACLS assumes the bradyarrhythmia is causing instability: a primary electrical problem that can be treated with atropine, epinephrine or pacing. But in a study of unstable bradycardia in the emergency department, only half the cases were caused by a disturbance of automaticity/conduction that might require pacing. The other half were secondary bradycardias where ACLS won’t work: atropine won’t open an occluded coronary artery, and you can’t pace the patient out of hyperkalemia.
As well as considering ACLS to stabilize primary bradycardias, we also have to look for secondary BRADIs:
- BRASH/hyperkalemia: bradycardia is a high risk feature in hyperkalemia, especially if associated with the BRASH syndrome, and requires empiric calcium
- Reduced vitals: hypoxia, hypothermia (environmental and hypothyroid), requiring normalization
- Acute coronary occlusion, especially inferior/posterior from circumflex artery (that perfuses the SA node) or right coronary artery (that perfused SA and AV nodes), requires reperfusion
- Drugs, eg beta-blocker, calcium channel blocker, digoxin – requiring withholding or reversal
- Intracranial bleed requiring surgery; Infection (eg lyme) requiring antibiotics
Back to the cases
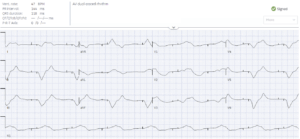
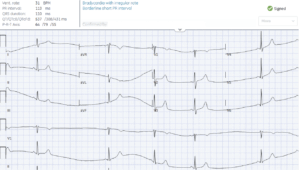
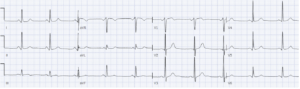
Case 1: 90yo with weakness, BP 90
- Heart rate/rhythm: AV pacing at rate of 48 with sensing and capture
- Electrical conduction: very wide QRS
- Axis: extreme
- R-wave progression: late from pacing
- Tall/small voltages: normal
- ST/T: secondary/discordant changes
= unstable bradycardia in very wide paced rhythm, rule out hyperkalemia. Treated with empiric calcium. Potassium 8 from AKI and sepsis – treated with shifting, fluids and antibiotics. Repeat ECG after treatment showed normal sinus rhythm with ventricular pacing and appropriate QRS width:
–
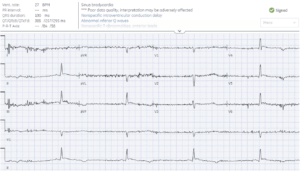
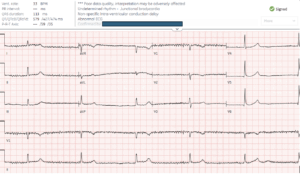
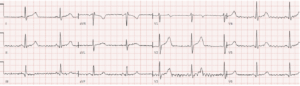
Case 2: 60yo with weakness and lethargy, BP 80
- H: sinus bradycardia with artifact
- E: normal PR/QRS, very long QT (missed by computer) caused by ST prolongation (ie small T wave at the end of a long ST)
- A: indeterminate due to artifact
- R: normal R-wave
- T: normal voltages
- S: prominent J waves (which computer thinks are T waves); mild inferolateral TWI
= unstable bradycardia secondary to hypothermia. Patient had temperature of 22 degrees Celsius, diagnosed as myxedema coma. Repeat ECG after warming, steroids, levothyroxine: normal sinus, normal QT, no J waves.
–
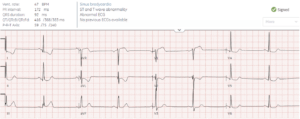
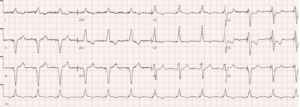
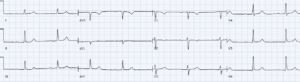
Case 3: 60yo with chest pain, BP 100
- H: sinus brady
- E: normal intervals
- A: normal axis
- R: normal R-wave
- T: normal intervals
- S: primary STD/TWI in I/aVL reciprocal to subtle STE/hyperacute T in III (inferior OMI), associated STD in V2 (posterior MI) and STE in V1 (RV MI) with reciprocal STD V5-6
= unstable bradycardia secondary to proximal RCA occlusion. Cath lab activated: RCA occlusion, peak troponin 12,000ng/L. Post-cath ECG shows normal sinus rhythm, resolution of reciprocal changes, subtle reperfusion T wave inversion in III and V2 (reciprocally tall T wave) and tall R wave in V2:
–
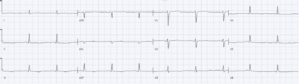
Case 4: 40yo with sudden collapse, GCS 7, BP 170/110
- H: sinus bradycardia with irregular rate
- E: short PR
- A: normal axis
- R: borderline early R-wave
- T: normal voltages
- S: no ST/T changes
= unstable bradycardia secondary to Cushing’s response. Intubated and taken for CT scan, which showed large intracerebral hemorrhage with mass effect:

Treated with hypertonic saline then emergency neurosurgery. Follow up ECG normal
–
Case 5: 90yo, AF on low dose beta-blocker, with few days of weakness and increasing lethargy, BP 80
- H: junctional bradycardia with shiver artifact, vs AF with complete AV block and junctional escape
- E: no PR, narrow QRS, normal QT
- A: normal axis
- R: normal R wave
- T: normal voltage
- S: no ST/T
= unstable bradycardia, possibly 3rd degree AV block, without obvious secondary cause. Initially stabilized by ACLS with atropine, epi and pacing. Possible secondary causes included BRASH from beta-blocker, hypotension and mild hyperkalemia at 5.8 treated with calcium and shifting; and hypothermia at 33 Celsius treated with warming and empiric antibiotics for possible sepsis. But due to possibility of AF with complete AV block, also received a permanent pacemaker. Follow up ECG showed normal sinus rhythm
–
Key take home points for ACLS dysrhthmia pitfalls part 1: unstable bradycardia
- For patients who are unstable from primary bradycardias, ACLS can provide hemodynamic support with atropine, epi and pacing
- Look for reversible causes of secondary BRADIcardias, some of which can be identified on 12-lead ECG: BRASH/hyperkalemia requiring empiric calcium, Reduced vitals requiring support (eg hypoxia, hypothermia), Acute coronary occlusion (especially inferior/posterior) requiring reperfusion, Drugs requiring withholding or reversal, and ICH requiring surgery or Infection (eg lyme) requiring antibiotics
Elevate your skills! For small group, live and highly interactive ECG courses, visit www.heartsECGcourse.com – including the new course HEARTS arrhythmia: beyond ACLS


Leave A Comment