

Topics in this EM Quick Hits podcast
Isaac Bogoch on osteomyelitis recognition, workup and management in the ED (01:31)
Anand Swaminathan on tourniquet application tips and tricks (41:29)
Andrew Tagg on managing pediatric distal radius buckle fractures & the FORCE trial (44:36)
Justin Morgenstern on Delayed Sequence Intubation (DSI): RCT Takeaways (50:43)
Brit Long on ESRD & Dialysis in the ED: altered mental status differential diagnosis considerations (57:36)
Lisa Thurgur & Victoria Myers on leadership and medical education in our EM Leadership Spotlight series (1:07:04)
Podcast: Play in new window | Download (Duration: 1:25:12 — 78.1MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Brandon Ng, edited by Anton Helman, October, 2025
Cite this podcast as: Helman, A. Swaminathan, A. Tagg, A. Morgenstern, J. Long, B. Thurgur, L. Myers, V. EM Quick Hits 68 – Osteomyelitis, Tourniquet Technique, Pediatric Distal Radius Buckle Fractures, DSI RCT, AMS in ESRD & Dialysis. Emergency Medicine Cases. October, 2025. https://emergencymedicinecases.com/em-quick-hits-october-2025/. Accessed August 6, 2026.
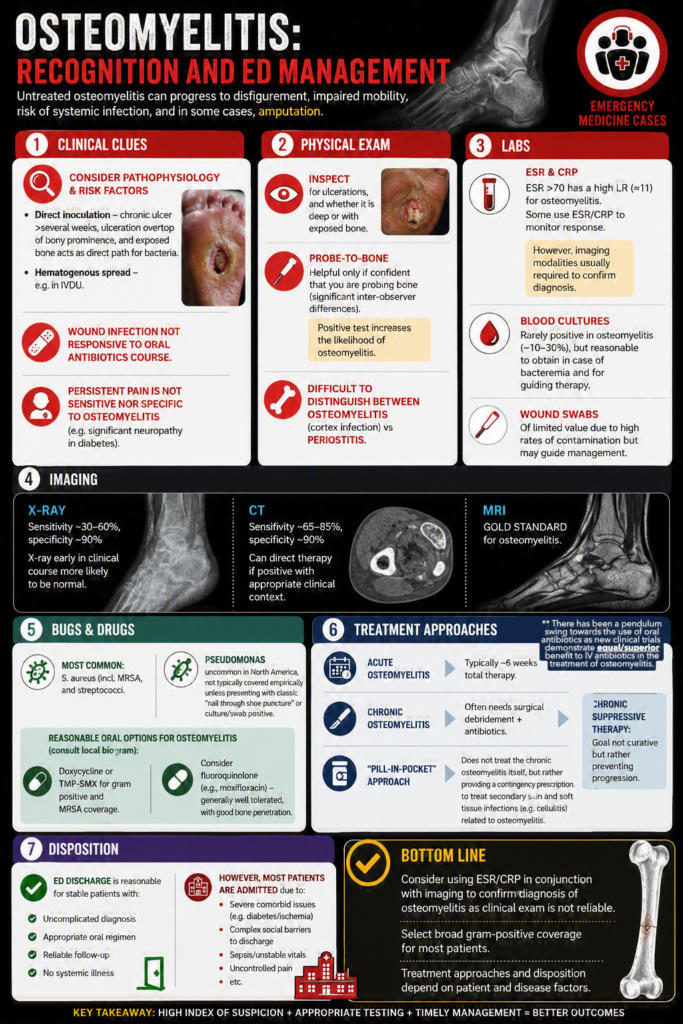
Osteomyelitis: Recognition and ED Management
Untreated osteomyelitis can progress to disfigurement, impaired mobility, risk of systemic infection, and in some cases, amputation.
Clinical clues:
- Consider pathophysiology & risk factors:
- Direct inoculation – chronic ulcer present for >several weeks, ulceration overtop of bony prominence, and exposed bone acts as direct path for bacteria.
- Hematogenous spread – e.g. in IVDU.
- Wound infection not responsive to oral antibiotics course.
- Persistent pain is not sensitive nor specific to osteomyelitis (e.g. significant neuropathy in diabetes).
Physical exam:
- Inspect for ulcerations, and whether it is deep or with exposed bone.
- Probe‑to‑bone: helpful only if confident that you are probing bone (significant inter-observer differences).
- Positive test increases the likelihood of osteomyelitis.
- Difficult to distinguish between osteomyelitis (cortex infection) vs periostitis.
Labs:
- Consider ESR & CRP: ESR >70 has a high LR (≈11) for osteomyelitis. Some use ESR/CRP to monitor response.
- However, imaging modalities usually required to confirm diagnosis.
- Blood cultures: rarely positive in osteomyelitis (~10–30%), but reasonable to obtain in case of bacteremia and for guiding therapy.
- Wound swabs of limited value due to high rates of contamination but may guide management.
Imaging:
- X‑ray: sensitivity ~30–60%, specificity ~90%; X-ray early in clinical course more likely to be normal.
- CT: sensitivity ~65–85%, specificity ~90%; can direct therapy if positive with appropriate clinical context.
- MRI: gold standard for osteomyelitis.
Bugs & drugs:
- Most common: S. aureus (incl. MRSA) and streptococci.
- Pseudomonas uncommon in North America, not typically covered empirically unless presenting with classic “nail through shoe puncture” or culture/swab positive.
- Reasonable oral options for osteomyelitis (consult local biogram):
- Doxycycline or TMP‑SMX for gram positive and MRSA coverage.
- Consider fluoroquinolone (e.g., moxifloxacin) – generally well tolerated, with good bone penetration.
Treatment approaches:
- Acute osteomyelitis: typically ~6 weeks total therapy.
- Chronic osteomyelitis: often needs surgical debridement + antibiotics.
- Chronic suppressive therapy: goal not curative but rather preventing progression.
- “Pill‑in‑pocket” approach: Does not treat the chronic osteomyelitis itself, but rather providing a contingency prescription to treat secondary skin and soft tissue infections (e.g. cellulitis) related to osteomyelitis.
Disposition:
- ED discharge is reasonable for stable patients with an uncomplicated diagnosis, appropriate oral regimen, reliable follow‑up, and no systemic illness.
- However, most patients are admitted due to severe comorbid issues (e.g. diabetes/ischemia), complex social barriers to discharge, sepsis/unstable vitals, uncontrolled pain etc.
Bottom line: Consider using ESR/CRP in conjunction with imaging to confirm diagnosis of osteomyelitis as clinical exam is not reliable. Select broad gram-positive coverage for most patients. Treatment approaches and disposition depend on patient and disease factors.
EM Cases Osteomyelitis Infographic. Made by Paul Esemu-Ezewu, edited by Sara Brade.
- Butalia S, Palda VA, Sargeant RJ, Detsky AS, Mourad O. Does this patient with diabetes have osteomyelitis of the lower extremity? JAMA. 2008 Feb 20;299(7):806-13. doi: 10.1001/jama.299.7.806. PMID: 18285592.
- Bury DC, Rogers TS, Dickman MM. Osteomyelitis: Diagnosis and Treatment. Am Fam Physician. 2021 Oct 1;104(4):395-402. PMID: 34652112.
- Doub JB. Treatment of Recurrent Severe Cellulitis with a Pill in Pocket Approach. Infect Chemother. 2022 Jun;54(2):382-387. doi: 10.3947/ic.2021.0095. Epub 2022 Jan 14. PMID: 35132835; PMCID: PMC9259910.
6 Tourniquet Technique Tips and Tricks
6 Tips on tourniquet placement
- Hemorrhage control takes priority; apply early and do not delay tourniquet placement due to fear of limb-loss.
- Location: 2–3 inches (5–6 cm) above the bleeding site.
- Avoid joints as those areas are difficult to compress with tourniquet.
- If the source of bleeding is unclear, go as high on the limb as possible.
- Tighten the Velcro first, then turn the windlass 1-2x until bleeding stops and distal pulses are absent.
- Document the exact time of application.
Management of Pediatric Distal Radius Buckle Fractures – FORCE Trial
Best of Don't Forget the Bubbles EM Quick Hits series
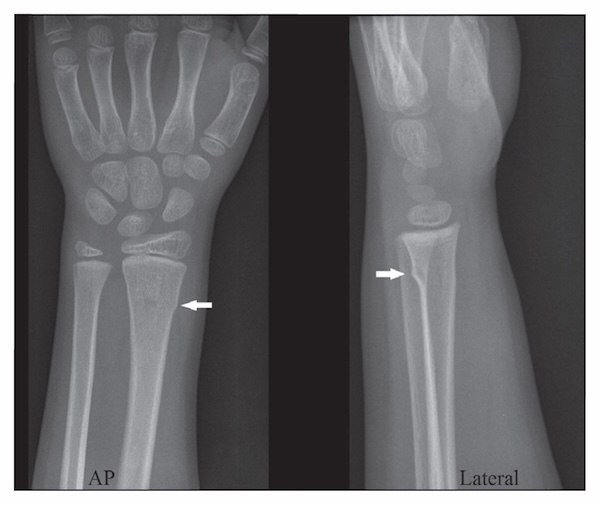
Buckle fracture = compressive cortical crumple.
- A stable fracture with negligible risk of displacement; heals well with minimal intervention
- On X-ray: No angulation, no cortical breach, away from physis & growth plate; often only visible on lateral view.
The Paper: Immobilisation of torus fractures of the wrist in children (FORCE): a randomised controlled equivalence trial in the UK by Perry et al. Lancet 2022.
P: Children aged 4-15 years with distal radius buckle fractures across 23 hospitals (n = 965).
I: Bandage (simple bandage e.g. gauze roller bandage) and discharge with no planned follow-up (n = 489).
C: Rigid immobilization (e.g. backslab) routine fractureclinic followup (n = 476).
O: Pain at 3-days post-randomisation measured using Wong-Baker FACES Scale: Equivalent at day 3 between bandage (3.21 points; SD 2.08) vs. rigid immobilization group (3.14 points; SD 2.11). No significant differences in PROMIS upper extremity scores, EQ-5DY-3L utility scores, parental satisfaction at 6 weeks, and rate of complications.
Limitations of this study:
- Buckle fracture diagnosis made by clinicians' interpretation of X-rays.
- Short follow up period (3 days, 7 days, 6 weeks) – hence unable to answer questions on long term outcomes.
- Children & parents were not blinded – which may influence satisfaction and pain ratings.
Example discussion to concerned parents:
- "This is a stable bend in the bone, not a break through it. There is nothing to push back into place, and nothing can shift."
- "We know from large studies that kids actually do better when we don't overtreat this type of injury."
- "We are treating it with comfort and time, not plaster and appointments."
- Buckle fractures are "like a dent in a pool noodle: safe, springy, and ready to bounce back."
Bottom line: For most buckle fractures, less is more. Soft support and early discharge can outperform casts and routine followup.
- Perry DC, Achten J, Knight R, Appelbe D, Dutton SJ, Dritsaki M, Mason JM, Roland DT, Messahel S, Widnall J, Costa ML; FORCE Collaborators in collaboration with PERUKI. Immobilisation of torus fractures of the wrist in children (FORCE): a randomised controlled equivalence trial in the UK. Lancet. 2022 Oct 1;400(10358):1102.
- Katy Morgan, Tessa Davis. The FORCE trial, Don't Forget the Bubbles, 2022. Available at: https://doi.org/10.31440/DFTB.49584
Delayed Sequence Intubation (DSI): RCT Takeaways

Background: DSI is sedation (commonly ketamine) to facilitate preoxygenation (e.g. with BVM, BiPAP) in the severely agitated/hypoxic patient prior to paralysis and intubation. This is the first well designed DSI RCT.
The Paper: Peri-Intubation Hypoxia After Delayed Versus Rapid Sequence Intubation in Critically Injured Patients on Arrival to Trauma Triage: A Randomized Controlled Trial by Bandyopadhyay et al. Anesth Analg 2023.
P: Critically injured patients who required definitive airway management on arrival (n = 200).
I: DSI group: administration of dissociative IV ketamine followed by 3 minutes of preoxygenation then IV succinylcholine for intubation.
C: RSI group: 3-minute preoxygenation preformed before ketamine and succinylcholine for induction and paralysis.
O: Incidence of peri-intubation hypoxia: lower in DSI (8%) vs RSI (35%, p = 0.001). First-attempt success rate higher in DSI (83%) vs RSI (69%, p = 0.02).
Limitations of this study:
- Unblinded, single centered RCT.
- Unclear definition of hypoxia (e.g. 92% or 90%).
- Unclear if adequate pre-oxygenation occurred in the trial.
- DSI was applied to all patients, rather than just those who were agitated.
Bottom line: There is limited evidence supporting the use of DSI in agitated patients. However, there is theoretically low harm and improved safety with DSI. Consider using it selectively for the agitated, hypoxic patient who cannot be preoxygenated safely.
- Bandyopadhyay A, Kumar P, Jafra A, Thakur H, Yaddanapudi LN, Jain K. Peri-Intubation Hypoxia After Delayed Versus Rapid Sequence Intubation in Critically Injured Patients on Arrival to Trauma Triage: A Randomized Controlled Trial. Anesth Analg. 2023 May 1;136(5):913-919. doi: 10.1213/ANE.0000000000006171. Epub 2023 Apr 14. PMID: 37058727.
ESRD & Dialysis in the ED: Altered mental status
This is part 2 of our 2-part EM Quick Hits series on ESRD & Dialysis. We suggest reviewing part 1 if you haven't already – https://emergencymedicinecases.com/em-quick-hits-august2025/
Beyond typical differentials for altered mental status, patients with dialysis have additional considerations:
- Structural:
- Subdural hematoma (risk 10–20× higher), ischemic/hemorrhagic stroke – patients often have uremic platelet dysfunction and anticoagulation → Low threshold for head CT.
- Consider reversing anticoagulation & managing raised ICP.
- Thrombolytics are not contraindicated in ESRD.
- Metabolic:
- Hypoglycemia (many patients with ESRD have diabetes on insulin) – check serum glucose.
- Electrolyte derangements (e.g. hyperkalemia/hypocalcemia) – extended lytes panel and ECG.
- Uremic encephalopathy (often after missed dialysis) – presentation varies from mood changes and weakness to seizure and coma.
- Infection/sepsis – patients with ESRD are often immunocompromised – cultures, broad spectrum antibiotics.
- Dialysis disequilibrium syndrome (only in hemodialysis, rare) – more common in patients starting dialysis, with presentation ranging from headache/n/v to altered mentation and seizures. Mild cases improve with reducing flow rate of dialysis. Severe cases require stopping dialysis. Consider hypertonic saline.
- Dialysis dementia (uncommon with current dialysis machines) – typically in patients on dialysis >2 years.
- Medications effects:
- Many medications require dose adjustments (e.g. antibiotics, metoclopramide, benzodiazepines, opioids).
- Opiods: Prefer fentanyl > hydromorphone/morphine for analgesia; reduce dose by 75% of standard dosing. Avoid tramadol.
- Avoid nephrotoxic or hyperkalemiaprovoking meds (e.g., TMPSMX, NSAIDs).
Bottom line: The differential diagnosis of altered mental status in patients with ESRD on dialysis is wide with several diagnoses that are specific to ESRD/dialysis. Check glucose/extended lytes/ECG, maintain a low threshold for head CT, and consider prescribed medications as causes of AMS.
- Long B, Koyfman A, Lee CM. Emergency medicine evaluation and management of the end stage renal disease patient. Am J Emerg Med. 2017 Dec;35(12):1946-1955. doi: 10.1016/j.ajem.2017.09.002. Epub 2017 Sep 5. PMID: 28893450.
EM Leadership series #3 with Dr. Lisa Thurgur
In this EM Quick Hits leadership spotlight, Victoria Myers interviews Lisa Thurgur—Emergency Physician, medical toxicologist, former uOttawa EM residency program director and passionate advocate for trainees—on what authentic leadership in EM education looks like. Dr. Thurgur describes why trying to imitate a celebrated PD predecessor didn’t work—owning her style did. She unpacks the real PD tightrope: relentlessly supporting residents while upholding professional and academic standards, recognizing that lapses often signal underlying issues needing advocacy, and building a culture of transparency, coaching and mutual respect amid competing priorities of the ED, university and postgraduate programs. Looking forward, she highlights the shift to individualized training and the rising impact of AI in clinical care and education. Her take-home pearls: seek out (and say yes to) leadership opportunities, lead as yourself because you were chosen for a reason, and remember—the PD’s #1 job is to be an advocate for residents.



Leave A Comment