
In the ED, we regularly care for sick patients presenting acutely with abnormal vital signs, altered mental status, and end organ dysfunction. Oftentimes, the culprit ends up being sepsis, or overdose, or organ failure. But it is important that we consider rarer endocrine presentations like decompensated hypothyroidism. In this Part 1 of our two-part podcast series on thyroid emergencies with Dr George Willis and Dr Alyssa Louis, we answer questions like: Why is the term myxedema coma a misnomer and should be abandoned? How can we differentiate between sepsis or environmental hypothermia or toxidrome from decompensated hypothyroidism at the bedside? When is it appropriate to order a TSH, a T4 and T3? What are the most important life-threatening triggers that need to be addressed in patients with decompensated hypothyroidism? Why is it important to test for cortisol levels and consider stress-dose steroids in all patients with decompensated hypothyroidism? Why is endotracheal intubation particularly dangerous in decompensated hypothyroidism? What is the best way to manage hypothermia in decompensated hypothyroidism patients? Why is the order of medications for treatment of decompensated hypothyroidism so important? and many more…
Podcast: Play in new window | Download (Duration: 1:12:13 — 66.2MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Matthew McArther, edited by Anton Helman December, 2025
Cite this podcast as: Helman, A. Louis, A. Willis, G. Decompensated Hypothyroidism Recognition and Management. Emergency Medicine Cases. December, 2025. https://emergencymedicinecases.com/decompensated-hypothyroidism. Accessed July 21, 2026
Myxedema coma is a misnomer and should be abandoned
Historically, severe hypothyroidism was called myxedema coma. Unfortunately, this is an imprecise term which does not capture all decompensated hypothyroidism presentations.
- Myxedema is not always present on exam and it may present anywhere on the body rather than the classic pretibial location
- Coma may not be present – more often, patients present with milder altered mental status such as confusion or drowsiness
For this reason, our experts advocate use of the term decompensated hypothyroidism which simply refers to a hypothyroid state causing end organ dysfunction.

Pretibial and hand myxedema (Source: Wikipedia)
Recognition of decompensated hypothyroidism: An often subtle presentation
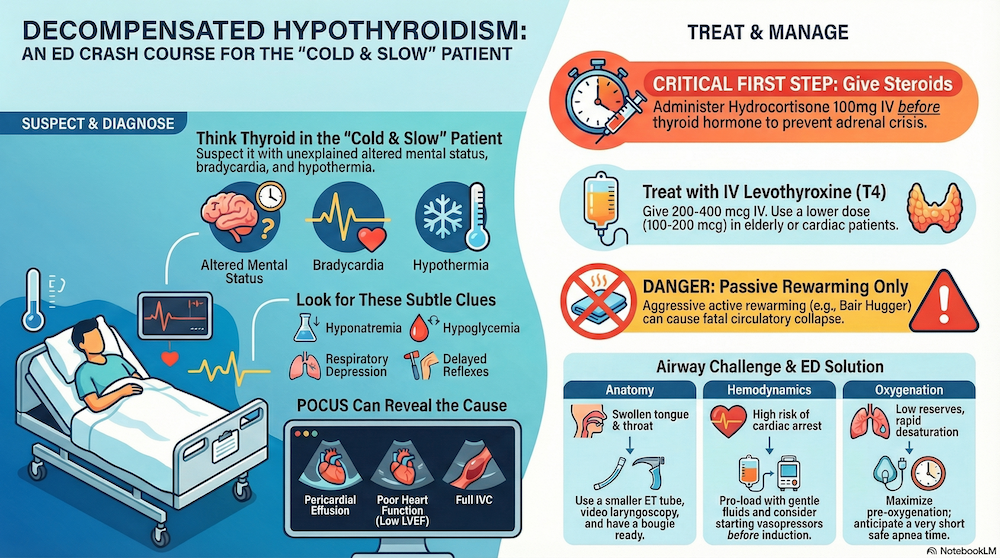
The classic clinical triad of decompensated hypothyroidism is altered mental status, bradycardia, and hypothermia and like all classic triads in medicine, this may not be present in all patients.
Common clinical manifestations/clues of hypothyroidism that should trigger a consideration for working up decompensated hypothyroidism in the ED include:
- Hypothermia
- Bradycardia
- Hypotension
- Hypoglycemia
- Hyponatremia
- Respiratory depression
- Delayed Deep Tendon Reflexes
- Unexplained AMS or sepsis without a clear source
Pearl: Test TSH and T4 in any patient with unexplained hypothermia, bradycardia, hypotension, hypoglycemia, hyponatremia, respiratory depression, or altered mental status.
Important complications of decompensated hypothyroidism that may contribute to the presentation and need to be addressed early in management in addition to the above include:
- Cardiac
- Heart failure
- Pericardial effusion/tamponade
- Dysrhthmias
- Neurologic
- Coma
- Seizures
- Resp
- Hypercapneic respiratory failure
- Pleural effusions
- Metabolic
- Adrenal insufficiency
Thyroid scoring tools
Multiple clinical scoring tools, namely the Popoveniuc Score and the Chiong Tool, have been created to assist in diagnosing decompensated hypothyroidism/myxedema coma. However, they are derived from retrospective studies with a very small number of patients, and have not been prospectively validated. For this reason, our experts recommend against their routine use. However, the components are important to review.
The Popoveniuc Score includes the following items which may help in diagnostic decision making:

Score Interpretation
| Total Score | Interpretation |
|---|---|
| ≥60 | Diagnostic / highly suggestive of myxedema coma |
| 25–59 | Supportive of diagnosis |
| <25 | Myxedema coma unlikely |
Differentiating decompensated hypothyroidism from sepsis, toxidromes, environmental hypothermia
The “cold-slow” features of decompensated hypothyroidism are nonspecific and overlap with many other more common ED presentations. However, there are often clues on history and physical that guide clinical suspicion.
How to differentiated decompensated hypothyroidism from sepsis
Septic patients may present with altered mental status, hypotension, and sometimes hypothermia. However, sepsis patients typically are tachycardic and tachypneic as apposed to bradycardic and bradypneic. Unexplained bradycardia or respiratory depression in a patient who otherwise appears septic should raise suspicion for decompensated hypothyroidism.
How to differentiate decompensated hypothyroidism from “Low and Slow” toxidrome
Often, overdose is suspected based on clinical history provided by the patient, collaterals, EMS or medication list. Consider the specific toxidromes for beta blocker / calcium channel blocker, opioid, sedative hypnotic, or cholinergic which may cause “low and slow” presentations similar to hypothyroidism.
Decompensated hypothyroidism evolves over days to weeks, often after a stressor, and is distinguished by hypothermia, dry skin, ileus/constipation, hyponatremia, and hypoventilation with hypercapnia. In contrast, “low and slow” toxidromes present more acutely and usually have normothermia, characteristic clues (pinpoint pupils and bradypnea with opioids, wet secretions/diarrhea with cholinergics, hyperglycemia with CCBs), and rapid response to antidotes. Lack of immediate improvement after naloxone, atropine, calcium, or glucagon—combined with cold, dry physiology—should push you toward empiric treatment for myxedema coma.
See EMCases Episode 90 for additional discussion of “low and slow” toxidromes.
How to differentiate decompensated hypothyroidism from environmental hypothermia
Environmental hypothermia is often suspected from clinical history. Patients with mild hypothermia (32-35 Celsius) should shiver, whereas patients with hypothyroidism in the same temperature range will not shiver. Environmental hypothermia is defined by cold exposure with relatively preserved labs and physiology, and mental status improves with rewarming alone. If the patient remains bradycardic, hypercapnic, or encephalopathic despite rewarming, or has hyponatremia and ileus, think decomensated hypothyroidism and treat empirically.
Indications to order a TSH and T4 for suspected decompensated hypothyroidism
Have a low threshold to test for decompensated hypothyroidism in any patient with unexplained hypothermia, bradycardia, hyponatremia, hypoglycemia, or altered mental status. The test of choice is TSH and T4. T3 is the metabolically active thyroid hormone, which is converted from the prohormone T4. T3 is generally not tested in the ED, however there are rare instances of decompensated hypothyroidism with a normal TSH and T4.
Consider adding TSH and T4 to your default lab panels for patients with presentations such as undifferentiated sepsis, altered mental status, or metabolic abnormalities.
ECG findings in decompensated hypothyroidism
- Decreased voltages reflecting pericardial effusion
- Bradycardia
- T wave inversions
- Prolong QTc.
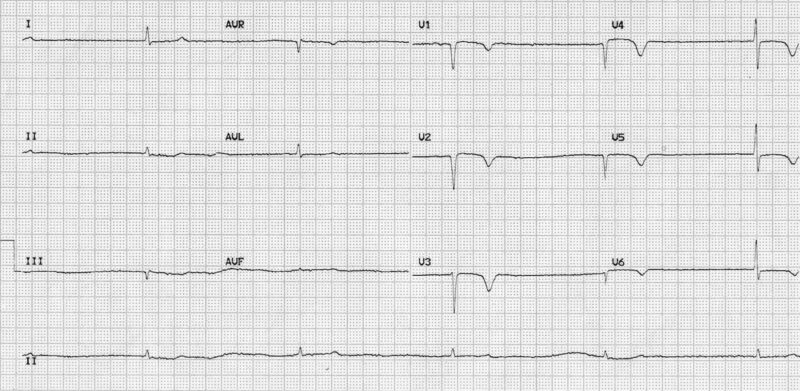
ECG of patient with decompensated hypothyroidism showing bradhycardia, low voltages and diffuse flipped T waves. Source: Life in the Fast Lane.
Triggers to identify and manage in decompensated hypothyroidism
Decompensated hypothyroidism is often precipitated by an acute trigger that tips the patient over into a decompensated state.
Be sure to investigate and manage any triggers.
- Infection (common)
- Cold exposure
- Sedatives/opioids
- Stroke
- MI
- GI bleeding
- Non-compliance or abrupt withdrawal of thyroid hormone
Pearl: For all sick patients with hypothyroidism, consider initiating empiric, broad spectrum antibiotics and a septic workup – there is often an infectious trigger which precipitated their presentation.
A review of all current medications and recent changes to medication is essential. Non-compliance with thyroid medication is the most common precipitant. Additionally, many medications can interact with thyroid function including:
- Amiodarone
- Lithium
- SSRI
- Opioids
- Neuroleptics
- Iodinated contrast
Why testing for Cortisol and considering “stress dose” steroids in decompensated hypothyroidism
Obtain a random cortisol in all patients with decompensated hypothyroidism. Give stress dose steroids (hydrocortisone 100mg IV q8H) prior to treating with levothyroxine, as treatment of the hypothyroidism could unmask or precipitate adrenal insufficiency due to shifts in metabolism.
Pitfall: neglecting to administer stress dose steroids in patients with decompensated hypothyroidism prior to levothyroxine administration is pitfall that may result in precipitated adrenal crisis.
PoCUS in decompensated thyroid disease
Here are some findings to look out for in decompensated hypothyroidism which may influence your management:
Cardiac: decreased contractility/reduced LVEF, pericardial effusion, may suggest cardiac involvement → look for tamponade physiology if effusion
IVC: often full → caution with IV fluids
Lungs: bilateral B lines → suggestive of congestive heart failure as a complication of decompensated hypothyroidism, pleural effusions
Airway management in decompensated hypothyroidism: Anticipate physiologically and anatomically difficult airway
Anticipate that decompensated hypothyroidism patients will have both physiologically and anatomically difficult airways and avoid intubation unless necessary.
Hemodynamics: Because these patients have both bradycardia and hypotension, they may have fragile hemodynamics despite a reassuring-looking shock index. They may not tolerate the reduction in preload when switched to positive pressure ventilation and are at risk of post-intubation hypotension or arrest. Consider hanging norepinephrine pre-emptively and having push dose pressors ready. Use ketamine or etomidate for induction.
Oxygenation: Maximize pre-oxygenation; these patients often have bradypnea and hypoventilation and may de-oxygenate more rapidly during induction.
Anatomy: These patients may have large and edematous tongue and oropharyngeal structures secondary to myxedema, as well as large necks with goiter. Use an ET tube ½ size smaller than usual. Consider use of bougie to navigate the myxedema.
Management of shock in decompensated hypothyroidism
- Use IV fluids cautiously as heart failure is a not uncommon complication of decompensated hypothyroidism.
- Vasopressors may be ineffective until the underlying thyroid deficiency is treated.
- Norepinephrine is the first line vasopressor.
- Vasopressin can be considered if a second pressor is needed.
- Alternatively, if bradycardia or low EF, epinephrine can be considered.
Dosing Thyroxine (T4) for decompensated hypothyroidism
It is important to administer hydrocortisone prior to levothyroxine to prevent adrenal crisis and not to wait for TSH and free T4 lab testing results before initiating treatment. Treatment should be initiated based on clinical suspicion after history, physical and basic blood tests.
The recommended dosing range is levothyroxine 200mcg-400mcg IV loading dose for decompensated hypothyroidism.
Consider doses on the lower end 100-200mcg for older patients or those with heart disease who may be at increased risk of dysrhythmia.
Pitfall: one pitfall in the dosing of levothyroxine is to give ‘standard’ doses in the older patient with impaired heart function. It is important to lower the dose in these patients to avoid precipitating a cardiac dysrhythmia.
Liothyronine (T3) replacement in decompensated hypothyroidism
Treatment with liothyronine is somewhat more controversial and has increased risk of precipitating dysrhythmias compared to levothyroxine due to its potent cardiac effects. Consider using liothyronine in addition to levothyroxine, ideally in consultation with endocrinology/ICU, if severe/refractory symptoms despite T4 replacement. The initial dose is 5-20mcg IV.
Management of hypothermia in decompensated hypothyroidism
Treating the underlying thyroid problem is more important than any specific rewarming techniques.
Aggressive active rewarming could induce peripheral vasodilation and worsen circulatory collapse in these patients.
Our experts recommend passive rewarming with increasing the temperature of the room, blankets and cautious use of warmed IV fluids rather than more aggressive active rewarming techniques.
Pitfall: attempting aggressive active rewarming with Bair Hugger device etc. can precipitate circulatory collapse in patients with decompensated hypothyroidism; rewarming should be passive only.
Key take home points for recognition and management of decompensated hypothyroidism
Decompensated hypothyroidism is a rare, high-mortality endocrine emergency. Think of it in elderly or frail patients with altered mental status, hypothermia, and bradycardia. Treat aggressively with IV levothyroxine, steroids, supportive care, and trigger management, with admision to ICU.
- Think hypothyroid in the “cold-slow” patient.
- For unexplained bradycardia, altered mental status, hypoglycemia, hyponatremia – have a low threshold to test TSH and free T4, but don’t wait for the result to treat if clinical suspicion is high and the patient is crashing.
- If intubation is necessary – anticipate an anatomically and physiologically difficult airway and preload with gentle fluids and pressors.
- Do passive rewarming only; aggressive active rewarming could precipitate hypotension.
- Test a random cortisol and give stress-dose steroids up front prior to thyroxine (hydrocortisone 100 mg IV q8h) to cover possible adrenal insufficiency.
- Give IV levothyroxine 200–400 µg once (dial it down to 100–200 µg in frail or cardiac patients).
- Consider adding liothyronine in consultation with endocrine/ICU for the moribund patient not improving—but go low and slow in patients with cardiac disease.
- Give empiric broad-spectrum antibiotics and investigate for the precipitant— often infection.
References
- Chen, D. H., Hurtado, C. R., Chang, P., Zakher, M., & Angell, T. E. (2024). Clinical features and outcomes of myxedema coma in patients hospitalized for hypothyroidism: analysis of the United States national inpatient sample. Thyroid, 34(4), 419-428.
- Chen, Y.-J., Hou, S.-K., How, C.-K., Chern, C.-H., Lo, H.-C., Yen, D. H.-T., Huang, C.-I., & Lee, C.-H. (2010). Diagnosis of unrecognized primary overt hypothyroidism in the ED. The American journal of emergency medicine, 28(8), 866-870.
- Chiong, Y. V., Bammerlin, E., & Mariash, C. N. (2015). Development of an objective tool for the diagnosis of myxedema coma. Translational Research, 166(3), 233-243.
- Dutta, P., Bhansali, A., Masoodi, S. R., Bhadada, S., Sharma, N., & Rajput, R. (2008). Predictors of outcome in myxoedema coma: a study from a tertiary care centre. Critical Care, 12, 1-8.
- Elghawy, O., Hafey, A. C., McCartney, C. R., & Steinman, J. R. (2021). Successful Treatment of Myxedema Coma Using Liothyronine in the Setting of Adrenal Crisis. Journal of the Endocrine Society, 5(Supplement_1), A612-A613.
- Jonklaas, J., Bianco, A. C., Bauer, A. J., Burman, K. D., Cappola, A. R., Celi, F. S., Cooper, D. S., Kim, B. W., Peeters, R. P., & Rosenthal, M. S. (2014). Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid, 24(12), 1670-1751.
- Popoveniuc, G., Chandra, T., Sud, A., Sharma, M., Blackman, M. R., Burman, K. D., Mete, M., Desale, S., & Wartofsky, L. (2014). A diagnostic scoring system for myxedema coma. Endocrine Practice, 20(8), 808-817.
- Ross, D. (2025). Myxedema coma. In UpToDate. Wolters Kluwer Health.
- Ueda, K., Kiyota, A., Tsuchida, M., Okazaki, M., & Ozaki, N. (2019). Successful treatment of myxedema coma with a combination of levothyroxine and liothyronine. Endocrine Journal, 66(5), 469-474.
Drs. Helman, Louis and Willis have no conflicts of interest to declare
Now test your knowledge with a quiz.



Hey!
In the podcast you mention sending a TSH and T4 simultaneously which makes sense. Where I work in Sweden we have an agreement with the lab that if we send for a TSH and it comes back abnormal they automatically check T4.
Do you think this is sufficient or is there a high risk of missing the diagnosis because of, let’s say, a normal TSH but grossly abnormal T4? I cannot imagine such a scenario physiologically but I’d like to hear your expert opinion.
Thanks!