
In this ECG Cases blog we review 5 cases of seemingly stably bradycardia. Which require immediate intervention, and which require a pacemaker?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. December 2025
Five patients presented with bradycardia and normal blood pressure. How does ECG interpretation change management? Despite apparent stability, which require immediate treatment and which require admission for a pacemaker?
Case 1: 50yo with diarrhea and weakness
–
Case 2: 50yo with epigastric pain

–
Case 3: 60yo weak
–
Case 4: 85yo syncope while sitting
–
Case 5: 85yo, history of AF, with weakness and normal blood pressure
–
Stable bradycardia? Or dangerous bradycardia requiring a pacemaker?
This is the second in a series of blog posts on the pitfalls of ACLS algorithms for adults with a pulse – and how a systematic approach to the 12-lead ECG can improve acquisition, interpretation, and application. The first looked at unstable bradycardia, and this will look at stable bradycardia.
The ACLS algorithm for stable bradycardia is simple: monitor and observe. But when do we need to consider immediate treatment, or admission after observation? If the patient becomes unstable do we just revert to the unstable bradycardia algorithm? There are a number of pitfalls:
ECG acquisition: artifact can mimic AF, but looking at unaffected leads and the regularity of the rhythm can help differentiate (unless its AF with a slow regular ventricular response from complete AV block)
ECG interpretation: ACLS puts all stable bradycardias in the same category: a slow QRS on the rhythm strip, ignoring atrial activity, AV blocks, and fascicular blocks. Computer interpretations often miss a second P wave, and label ‘sinus bradycardia’ what is actually normal sinus with AV block. Assessing the AV node and fascicles can anticipate deterioration, avoid ACLS medications that won’t work (or will make things worse), and identify patients requiring admission for a pacemaker no matter how stable they are.
For AV blocks, what’s clinically relevant (if there are no secondary causes) is the location of the AV block, which determines whether atropine will work or whether the patient needs a pacemaker.
- Nodal block: atropine will work for bradycardia, if needed
- First degree: long PR (ie slow AV)
- Second degree type 1: prolonging PR (i.e slow AV) before drop
- Infra-nodal block: atropine will not work, needs a pacemaker
- Second degree type 2: fixed PR (ie normal AV) then sudden drop; often with signs of infranodal disease (eg bundle branch block). By increasing conduction into a diseased system, atropine can make the block worse
- Third degree: variable PR (ie complete AV block)
ECG application: ACLS is designed for primary bradycardias from an electrical problem. But seemingly stable patients with a secondary bradycardia can harbor an acute medical emergency that might be revealed on the full 12-lead ECG. The BRADI mnemonic (BRASH/hyperkalemia, Reduced vitals, Acute coronary occlusion, Drugs, ICP/Infection) summarizes secondary bradycardias, and two stand out as causes of bradycardia that can present with a false reassurance of stability, where the initial lab test may be unreliable, where ACLS algorithms fail, and yet where the ECG can guide empiric treatment: severe hyperkalemia requiring empiric calcium (rather than waiting for serum potassium, which is often hemolyzed), and Occlusion MI requiring cath lab actitation (rather than waiting for troponin, the first of which is often normal and not predictive of the peak).
Back to the cases
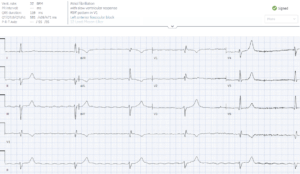
Case 1: 50yo with diarrhea and weakness
- Heart rate/rhythm: junctional bradycardia and artifact
- Electrical conduction: no PR, nonspecific wide QRS
- Axis: borderline extreme
- R-wave progression: normal
- Tall/small voltages: normal
- ST/T: diffuse peaked T waves
= bradycardia secondary to severe hyperkalemia, requires empiric calcium
Before calcium became unstable (and will not respond to atropine or pacing):

After calcium: ectopic atrial rhythm and normal axis, but still non-specific wide QRS and peaked T waves

After potassium normalization: normal ECG
–
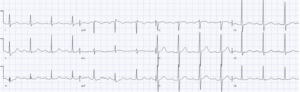
Case 2: 50yo with epigastric pain
- H: sinus bradycardia
- E: first degree AV block
- A: normal axis
- R: normal R wave
- T: normal voltages
- S: inferior hyperacute T wave with reciprocal deep TWI in aVL, and anterior STD V1-3
= bradycardia secondary to infero-posterior STEMI(-)Occlusion MI, requires cath lab activation
One hour later troponin returned at 250ng/L, and ECG repeated, now showing STEMI(+) Occlusion MI:
Cath lab activated: 99% RCA occlusion. Peak troponin 25,000 ng/L. Post-cath ECG had resolution of bradycardia and AV block, and subtle inferior reperfusion TWI:
–
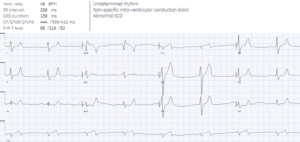
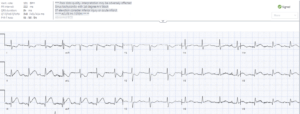
Case 3: 60yo weak
- H: normal sinus rhythm, not sinus bradycardia (see second P wave in V1)
- E: prolonged PR and second degree AV block with 2:1 conduction, LBBB
- A: left axis from LBBB
- R: delay R wave from LBBB
- T: normal voltages
- S: secondary repolarization abnormalities
= 2nd degree AV block with 2:1 conduction, plus LBBB indicating likely infranodal block, which could worsen with atropine.
Admitted to hospital and next day developed third degree AV block, which was treated with a pacemaker:
–
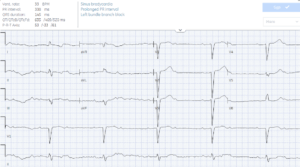
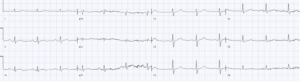
Case 4: 85yo syncope while sitting
- H: sinus bradycardia
- E: borderline PR, RBBB
- A: left axis from LAFB
- R: early R from RBBB, late S from LAFB
- T: normal voltages, borderline LVH in aVL from LAFB
- S: no changes
= syncope with bifascicular block. Admitted for pacemaker.
–
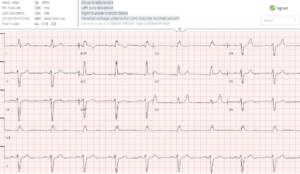
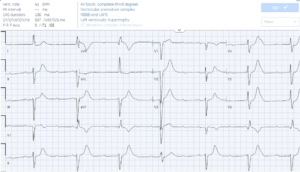
Case 5: 85yo, history of AF, with weakness and normal blood pressure
- H: AF with a slow and regular ventricular response = complete AV block with escape rhythm
- E: incomplete RBBB
- A: LAFB
- R: early R
- T: normal
- S: query peaked T wave
= AF with 3rd degree AV block and ventricular escape rhythm. Labs including potassium and troponin were normal, rate control meds were held, and patient admitted for pacemaker
Take home points for Stable Bradyardia? Or Dangerous Bradycardia Requiring Pacemaker
- Consider secondary causes of bradycardia which may initially appear stable but require immediate treatment: BRASH/hyperkalemia, Reduced vitals, Acute coronary occlusion, Drugs, ICP/Infection (eg lyme)
- If the ventricles are bradycardic, look for a higher rate in the atria associated with an AV block, and consider when a pacemaker might be needed – including infranodal AV blocks (2nd degree type 2, or 3rd degree), bifascicular blocks (eg RBBB + LAFB) in the context of syncope, or AF with a regular ventricular response from 3rd degree AV block
For online, live and highly interactive ECG courses to elevate your skills, join heartsECGcourse.com, including HEARTS arrhythmia: beyond ACLS



You can have a 3rd degree heart block in the context of inferior omi. Narrow qrs, nodal block, +/- 50% respond to atropine (IIa) or sometimes aminophylline (IIb).