
In this EM Cases CritCases blog – a collaboration with STARS Air Ambulance Service, and their medical director Mike Betzner, we present a challenging airway obstruction case, discuss the limitations of non-rebreather masks, using PEEP on bag-valve-masks, heliox, tips on awake intubation, and the differential for high peak inspiratory pressures in the post intubation period. With commentary by Michael Betzner and Reuben Strayer as well as expert peer review by George Kovacs…
Written by James Brokenshire; Edited by Michael Misch, Patrick Gilbride & Anton Helman; Expert Peer Review by George Kovacs, Feb 2017.
The Case
A 56 year old man develops respiratory distress on a commercial flight. He is provided supplemental oxygen while in flight, but does not improve and the plane diverts. EMS attends to the patient, where he is found to be hypoxic with a GCS of 12.
Initial vitals are T 37.4, HR 125, BP 160/95, RR 40, SpO2 50% room air, 63% on non-rebreather (NRB), high flow O2 with good pulse oximetry waveform .
Little is known with respect to this patient’s history. EMS requests advice with respect to improving this patient’s oxygenation for transport.

What would you advise to improve oxygenation for transport?
This patient presents with critical hypoxia, despite high flow oxygen by NRB. Oxygen saturations in this range put him at risk for hemodynamic instability, arrhythmia, anoxic brain injury, and death as he is on the steepest part of the oxyhemoglobin dissociation curve.
NRB face mask can deliver FiO2 in the range of 60-70% with 15L of O2 flow. Despite its name, most NRB masks don’t have a one way valve preventing air ingress. It is possible to increase the FiO2 delivered by standard NRB mask by increasing O2 flow to 30-60L/min, and this should be recommended to EMS in this case. Many standard fittings and tanks don’t support delivery beyond 15L/min however.
If you are not achieving adequate oxygenation with a non-rebreather, switch to a Bag Valve Mask (BVM). It is critical that you know the type of BVM at your institution. Many BVMs have a self inflating bag which can improve the FiO2 delivered. Optimally, the BVM should have one way inspiratory and expiratory valves. If this is not the case, when not assisting with ventilation the patient may entrain room air and dilute the Fi02, the extent of which depends on the minute ventilation that the patient is requiring. You can counter this by attaching a Positive End Expiratory Pressure Valve) (PEEP, see image below) to your BVM. BVMs with one way valves deliver oxygen to the patient if that patient makes enough inspiratory effort to open the valve (which may not be the case), or if the practitioner assists by squeezing the bag. This is an important concept. It is also crucial to maintain an adequate seal at the face to ensure a high FiO2 is delivered. Ensure that EMS is assisting the patient’s respirations with a BVM with a one way valve using good two-handed technique at the mask.
Knowing the type of BVM at your institution is critical.

Two handed technique to ensure adequate seal with BVM
This patient’s degree of hypoxia despite high FiO2 suggests that he may be exhibiting shunt physiology, in which alveoli are perfused but not ventilated. Noninvasive Positive Pressure Ventilation (NPPV) can be effective at recruiting alveoli and improving oxygenation in situations where shunt physiology is present. PEEP can be delivered in the ED or prehospital setting by using a simple PEEP valve which may be attached to the exhalation port of the BVM. Most PEEP valves allow the practitioner to dial in the amount of expiratory pressure. 10cmH2O would be a good starting point for EMS in this case. Ask EMS if they have a PEEP valve, and if so they should assist the patient with this in place, using a good two handed seal.

PEEP valve
Case Continued…
The patient is provided assistance with a BVM including a PEEP valve, and his SpO2 improves to 75%. IV access is obtained. He is transported without further intervention to your center. Further history is obtained. He has a recent diagnosis of a “soft tissue mass of the carina”, a neuroendocrine tumour for which he has had a tracheal stent placed. He has no other relevant medical history. Medications include Hydromorphone, Ondansetron and Citalopram. He is brought to the resuscitation bay, being assisted by EMS.
Vitals upon arrival are T 37.0, HR 120, BP 170/90, RR 48, SpO2 75% on 15L BVM assist with 10cmH2O PEEP.
He has marked respiratory distress, mild stridor and decreased air entry to the right base. He is awake and cooperative. He has a full code status. POCUS shows lung sliding and comet tails bilaterally, no pericardial effusion, no dilated RV, and reasonable LV function.
What is your initial management? What is your differential?
The differential diagnosis includes:
– tumor obstructing the tracheal lumen
– stent obstruction
– stent migration
– pneumothorax (less likely given the POCUS findings)
– chemotherapy induced cardiovascular collapse
– pneumonia
– pulmonary embolism
For initial management focus on improving oxygenation. This patient is awake and cooperative and is a perfect candidate for BiPAP. Oxygenate the patient in the upright position rather than supine. Ultimately this patient is likely to require definitive airway management, and it is crucial to improve oxygenation before this is entertained.
“I’d probably throw some heliox on – I’ve seen it work really well in large airway obstruction. Need to be careful and monitor closely since it’s only 40% O2.”
-Chris Hall MD FRCPC
Heliox is thought to reduce airflow resistance, work of breathing and dynamic hyperinflation. However, there is scant evidence for any benefit in lower airways obstructive lung disease. Heliox is considered to be a temporizing measure only and oxygenation should remain a priority.
In a critically ill patient where an infectious respiratory process is being considered, broad spectrum antibiotics such as Piperacillin/Tazobactam are appropriate. Consider the use of intravenous steroids such as dexamethasone as tumour obstruction is in the differential. Septic workup should likely include a chest X-ray, labs including lactate, VBG, and blood cultures. Get your “double set up” airway equipment to the bedside.
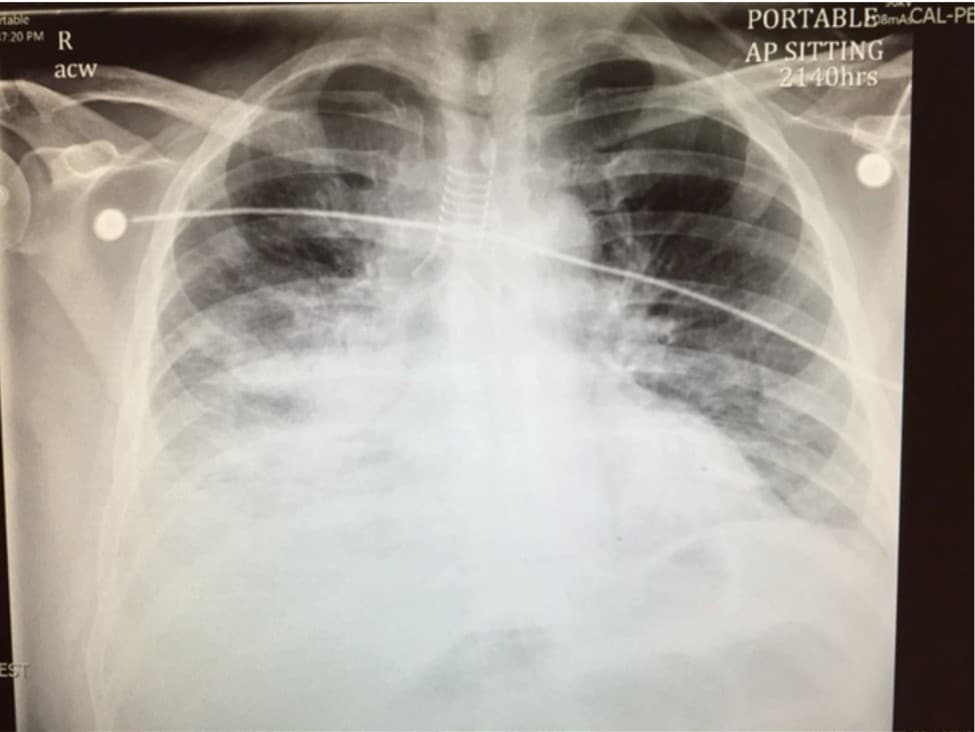
CXR showing tracheal stent, increased lung markings in the right lung base
Case Continued…
The respiratory therapist arrives and places the patient on BiPAP. His SpO2 quickly improves to 93%. He is now fatiguing, and the PvCO2 returns at 85 mmHg. The decision to intubate is made.
What is your approach to definitive airway management in this patient? Which medications will you use to facilitate endotracheal intubation?
The presence of an obstructing mass (the stent/tumour) in the subglottic region makes the management of this patient especially difficult. Time permitting, obtain anesthesia and surgical consultation for intubation in the OR setting with a “double setup” for possible operative airway.
“Surgery at bedside preferable. If the stent was visible when you tried to intubate because it had migrated proximally and you couldn’t push it gently down, then you’d have to go to a low trach.”
-Mike Betzner MD FRCPC“If the problem at this moment is the carina tumor, assuming no other anatomic difficulties, endotracheal intubation (ETI) should not be anatomically difficult, i.e. it shouldn’t be difficult to see the cords/deliver the tube. However, ETI may not help much, if his (lower) airway is critically obstructed from a carina tumor. However, with some of these anatomic obstructions, negative pressure (i.e. physiologic) ventilation doesn’t work, put positive pressure does – laryngospasm is famous for this ball-valve type effect. So ETI might make a big difference. That the patient improved markedly with PPV suggests that this effect is in play. If you have V-V ECMO capability, this would be a good time for that. Otherwise, I would probably maximally preoxygenate with high flow nasal cannula (if available) under NIV, then RSI with assistant standing by with pre-lubricated LMA in hand and everything you need for cricothyrotomy, though if the problem is a big carina tumor I’m not sure cric would go.”
-Reuben Strayer MD
In this case you may not have time to transport the patient to the OR. The presence of this mass makes the possibility of can’t intubate/can’t ventilate situation more likely. The use of sedation and paralytic to improve intubating conditions is always a balance of risk and benefit. Here, the use of paralytic, where the inability to secure a surgical airway likely exists, is suboptimal.
“Ideally intubated awake with a scope because of risk of upper airway obstruction. I’d call for anesthesia or ICU to scope. Doesn’t sound like there is much time so lido neb, lidocaine spray and ketamine prepared in case help isn’t immediately available. If I had to do it I would use a Bougie, advance gently, and wouldn’t paralyze even after intubation.”
-Rob Hall MD FRCPC“If my hand was forced I would proceed with Video Laryngoscopy (VL) with Bougie at the bedside, as well as a bronchoscope preloaded with an endotracheal tube in case I need help maneuvering an unexpected supraglottic mass. It would also help the ability to visualize the subglottic region once intubated. I would have various tube sizes and try to place the largest one possible.”
-Andrea Boone MD FRCPC
Awake intubation offers you several advantages in this case. You have a reasonably cooperative patient, you can maintain a spontaneously breathing patient, and you can maintain the patient’s airway reflexes by avoid the use of general anaesthesia and paralysis. Awake intubation can be accomplished using only topical anaesthesia, using sedation, or a combination of the two. Cooperative patients can often be awake intubated using only topical anaesthesia, however many ED patients require some measure of sedation. Ketamine in varying doses may help to facilitate awake intubation. It has the advantages of hemodynamic stability and minimal respiratory suppression. You are likely to have the most success using either Video Laryngoscopy (VL), or Fiberoptic Laryngoscopy, though direct laryngoscopy is acceptable. Which method you use will depend on your experience with these modalities, and the equipment and resources in your department. Fibreoptic Laryngoscopy is performed either via the nose or the mouth. In the case of the oropharyngeal route, it is best to use a bite block. The endotracheal tube is “railroaded” over the scope. That is, the scope is placed within the lumen of the tube. After the scope is passed through the chords, the tube is passed over it and the cuff inflated.
This patient is intubated awake, facilitated by Ketamine sedation. There a several considerations:
To inhibit oral secretions and facilitate local anesthesia:
– Glycopyrrolate 4 mcg/kg IV
– Atropine 0.4-0.6 mg IV
To provide topical anesthesia:
– 5 cc of atomized/nebulized 4% lidocaine
– 2% viscous lidocaine delivered to the posterior pharynx by tongue depressor
– Lidocaine 10 mg metered dose inhaler
For sedation
– Ketamine 0.5 to 2 mg/kg

This patient is given glycopyrolate 300 mcg IV. His airway is then topicalized with nebulized 4% lidocaine and topical 2% viscous lidocaine followed by 70 mg of ketamine. He continues to breath spontaneously. Laryngoscopy is performed using VL, and he is intubated with good EtCO2 and stable SpO2. It is important to have medication at the ready for induction of anaesthesia and perhaps paralytic for after successful intubation.
Case Continued…
Your respiratory therapist tells you they are having difficulty with high airway pressures post intubation. What is your management for this airway obstruction now?
The differential for high peak inspiratory pressures in the post intubation period includes:
1. Auto-PEEP caused by breath stacking
2. Tension pneumothorax
3. Bronchospasm
4. ETT obstruction
5. Ventilator circuit obstruction
6. Pneumonia
7. ARDS
You can troubleshoot this issue by determining the difference between peak (Ppeak) and plateau (Pplat) pressures. If the difference is greater than 5cm/H2O the differential for increased resistive work includes bronchospasm, circuit obstruction or ETT obstruction. If the difference is less than 5cm/H2O the differential for increased elastic work includes pneumothorax, auto-PEEP, pneumonia, and ARDS.
In this case the difference between Ppeak and Pplat is 8cm/H2O. RT checks the circuit, and it is unobstructed. You call for chest X-ray, and review its findings. This reveals the ETT in the trachea sitting directly against the tracheal stent, just proximal to the carina. You ask for the ETT to be brought back 2cm (to 21cm at the lips), and the high airway pressures resolve.

Case Resolution
With successful intubation, and ventilation with an FiO2 of 1.0 with high PEEP, you are able to oxygenate and ventilate this patient successfully. Anaesthesia attends the patient after transfer to ICU and on fiberoptic endoscopy finds stenosis proximal to the tracheal stent. A CT is obtained, and the results are visible below. He is consulted to radiation oncology for consideration of radiotherapy to reduce tumor size.

Take Home Points for Airway Obstruction
1. BVM with a PEEP valve can be used to facilitate preoxygenation in patient with shunt physiology.
2. BiPAP is an excellent modality to facilitate preoxygenation.
3. Awake intubation is a good option for situations in which you have a cooperative patient, you wish to maintain a spontaneously breathing patient, and you wish for the patient to maintain intact airway reflexes.
4. Topicalizing the patient adequately is crucial to success in awake intubation.
5. Ketamine may aid in obtaining proper conditions for awake intubation while maintaining a spontaneously breathing patient.
6. It is important to have an approach to common ventilator complications in the post intubation period.
7. Tracheal stents and their complications represent a relatively new and emerging area of knowledge for EPs.
Expert Peer Review by George Kovacs 
Theoretically there are only two options to manage the airway in the ED, either awake or by RSI. The default approach has become RSI as evidence supports a relatively high success rate in skilled hands. The one relative contraindication is the “difficult airway” which may be any or all of difficult laryngoscopy, intubation, mask ventilation, SGA ventilation and front of neck access (FONA). In patients in whom difficult intubation is predicted and where either BMV and rescue oxygenation (SGA, FONA) is predicted difficult, an awake approach is indicated. The one scenario where difficulty is relatively easily predicted is an upper airway obstruction. Stridor in adults should scare you and initiate a call for help. The airway is usually compromised by 50% in patients with acute resting stridor. Complete obstruction from this point is often sudden and lethal. Having information as to where the obstruction is relative to the glottic inlet and the cricothyroid membrane is helpful and may be available in cancer patients.
If this airway needs to be managed it should be done by the most experienced physician available, ideally in the OR with a surgeon available for FONA whether that be a trach or cric depending on the location of pathology. An awake trach (or awake cric) may be the most appropriate procedure to manage the patient’s upper airway pathology. Before I comment on the supraglottic approach this patient has a second reason to have an awake intubation – apnea intolerance. His sats are improved but they are most definitely not fully preoxygenated. In fact, apnea intolerance is the most common reason I perform awake intubations in the ED.
Let’s assume that the patient is cooperative. Ideally I would use no sedation as even ketamine in patients with upper airway obstruction may cause problems. I agree that the device for an awake intubation should be determined by the expertise of the user. VL with a hyperacute angled blade (GlideScope, CMAC D-blade) are good choices as they will be better tolerated than DL as less pressure is required on the back of the tongue. However, remember that getting too good of a view may cause problems with VL intubation and having a POGO of 50% or less with the glottis occupying the top half of the screen and the blade in the valleculae provides the most favorable orientation for placing the ETT with a GlideScope. Using a flexible intubating scope is a great option (and my preferred approach) as it allows visualization to the carina and is generally better tolerated.
High flow oxygen
Put the patient on high flow nasal oxygen (HFNO) during topicalization and the intubation process. Alternatively, keep them on BiPAP holding the mask to the patient’s face and performing topicalization in steps with intermittent ventilation (plus HFNO).
Heliox
Consider the use of heliox.
Topicalization
The key to successful awake intubation is meticulous application of topical anesthetic. Get the patient to stick out their tongue and get an assistant to trap the tongue anteriorly with gauze. Get 5% lidocaine ointment and apply it gently to the posterior tongue, the most “gagogenic” region of the oropharynx. Use an atomizer (not a nebulizer) and administer 4% lidocaine to everything in sight. Bend the nozzle tip inferiorly to anaesthetize the glottis and trachea ideally during inspiration. They will cough and they can obstruct so always have your blade, bougie and ETT for an emergency FONA.
ETT type and size
Use a small ETT in a patient with stridor (definitely nothing bigger than a 7.0) and have smaller tubes ready. Consider using a specialized Parker flextip ETT which because of bevel orientation, shape and flexibility can make ETT advancement easier with both VL and flexible intubating scopes.
Drugs and end tidal CO2
Have your post intubation drugs connected to your line ready for administration with end tidal CO2 detection.
Drs. Brokenshire, Misch, Gilbride, Helman and Kovacs have no conflicts of interest to declare.
References
1. Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA guidelines in the remote location.J Clin Anesth. 2004;16:508-516.
2. Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during
emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.
3. Nimmagadda U, Salem MR, Joseph NJ, et al. Efficacy of preoxygenation with tidal volume breathing. Comparison of breathing systems.Anesthesiology. 2000;93:693-698.
4. Joffe AM, Hetzel S, Liew EC. A two-handed jaw-thrust technique is superior to the one-handed “EC-clamp” technique for mask ventilation in the apneic unconscious person. Anesthesiology. 2010 Oct;113(4):873-9.
5. Patil VP. Airway emergencies in cancer. Indian J Crit Care Med. 2007;11(1):36-44.
6. Fitzgerald E, Hodzovic I, Smith AF. ‘From darkness into light’: time to make awake intubation with
videolaryngoscopy the primary technique for an anticipated difficult airway? Anaesthesia. 2015 Apr;70(4):387-92.
7. Mcgarvey JM, Pollack CV. Heliox in airway management. Emerg Med Clin North Am. 2008;26(4):905-20, viii.
Other FOAMed Resources on Airway Obstruction, Awake Intubation, Preoxygenation and Heliox
Life in the Fastlane reviews awake intubation
EMCrit discusses awake intubation
EMCrit reviews preoxygenation
Brian Driver video on heliox for airway obstruction
Life in the Fastlane reviews heliox



Fantastic review, and great case! Thanks for sharing.
Curious as to your thoughts about BVM seal using “thenar eminence” 2-hand grip on mask versus the “C-E” grip shown in your photo above. I’m a fan of the former, FWIW.
See: http://resus.me/effective-bmv/