
Melanie Baimel’s Best Case Ever on Post-Arrest Hyperkalemia on EM Cases
Post arrest patients can sometimes be challenging. We need to think of a variety of underlying causes of the arrest, antiarrhythmics, possible cath lab activation, targeted temperature management, sedation and more. To add to this, many post arrest patients do not have ideal vital signs that require attention. In this Best Case Ever, in anticipation of our upcoming episode on A Rational Approach to Hyperkalemia Dr. Melanie Baimel describes a post arrest patient who remains bradycardic and hypotensive despite multiple pressors….
Podcast: Play in new window | Download (Duration: 4:26 — 4.1MB)
Subscribe: Apple Podcasts
Published September 2016 by Anton Helman
Hyperkalemia is the Great ECG Imitator
Hyperkalemia can cause almost any dysrhythmia, but in particular, in patients who appear to be in “slow VTach” (ie. wide complex bradycardias), hyperkalemia should be high on your differential diagnosis. Not only can hyperkalemia cause almost any dysrhythmia, but the ECG in patients with hyperkalemia can even look like a STEMI, Brugada Syndrome or Benign Early Repolarization. One way to distinguish the ECG of a true STEMI from hyperkalemia with ST elevation is that the latter will usually show a right axis deviation.

Hyperkalemia mimicking Brugada Syndrome (care of Dr. Smith’s ECG Blog)
Classic hyperkalemia ECG progression
- Peaked T wave – a sensitive sign is if the amplitude of the T exceeds the amplitude of the R, but one needs to think about early MI as well!
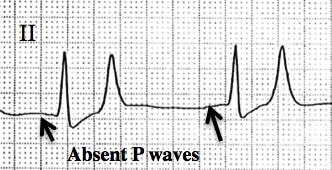
- Prolonged PR interval and flattening of the P wave
- Widening of the QRS
- Sine Wave

Peaked T waves of hyperkalemia

Sine wave pattern – pathagnomonic for hyperkalemia
Dr. Helman and Dr. Baimel have no conflicts of interest to declare.
References
Mattu A, Brady WJ, Robinson DA. Electrocardiographic manifestations of hyperkalemia. Am J Emerg Med. 2000;18:721–729.
FOAMed Resources
EM Cases 2015 ACLS Guidelines Post Arrest Care Controversies Episode
Dr. Smith’s ECG Blog on Hyperkalemia Pseudoinfarction Patterns



I think Also in true STEMI there would be reciprocal changes that is not typically seen with STE with hyperkalemia..