
In this ECG Cases blog we review 5 patients with wide complex tachyardias. Which will respond to ACLS, and which require different management?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. April 2026
Five patients presented with wide complex tachycardia with a normal blood pressure. Which will respond to ACLS, and which require different management?
Case 1: 75yo with fever
–
Case 2: 30yo with palpitations
–
Case 3: 80yo weak/confused, with nausea/vomiting
–
Case 4: 70yo with weakness
–
Case 5: 20yo with palpitations
–
Stable wide complex tachycardia
This is the third in a series of blog posts on the pitfalls of ACLS algorithms for adults with a pulse – including pitfalls in ECG acquisition, ECG interpretation, and ECG application. The first looked at unstable bradycardia, the second stable bradycardia, the third unstable tachycardia, and this one will look at stable wide complex tachycardia.
The ACLS algorithm for stable wide complex tachycardia is simple: assume it’s ventricular tachycardia (regardless of age or hemodynamic stability) and treat accordingly with an anti-arrhythmic like amiodarone or procainamide, and if that doesn’t work then electrically cardiovert. This is a safe approach for primary arrhythmias causing a non-sinus, regular, wide complex tachycardia. There are multiple complex algorithms to differentiate VT from SVT with aberrancy, none of which are 100% sensitive, so if those are the only two differentials then it’s safest to assume VT since they are both primary arrhythmias that respond to chemical or electrical cardioversion.
But those are not the only differentials, or even the most common differentials, for wide complex tachycardias. Others will not respond to electrical cardioversion or could worsen if treated with antiarrhythmics. In a CJEM article on wide complex tachycardias in the ED, the majority were AF or sinus tachycardia – and emergency physicians only identified 78.6% of sinus tachycardia.[1] Within the AF group a majority were tachycardic from a secondary cause, which requires treatment different than ACLS. There are number of ACLS pitfalls to consider:
- Acquisition: is it actually a tachy-arrhythmia? Artifact can mimic tachyarrhythmias, but be identified by unaffected leads recorded at the same time, or normal QRS complexes marching through the noise
- Interpretation: ACLS assumes stable wide complex tachycardia is VT (a regular, wide complex tachycardia, not driven by P waves), but is it?
- Irregularly irregular wide complex tachycardia without P waves is atrial fibrillation. The rapid ventricular response often has a secondary cause, or if rates are up to 300 with changing QRS complexes then there’s an accessory pathway that will worsen with AV node blockers (including amiodarone).
- Regular but very wide, or not fast enough, could indicate hyperkalemia or sodium channel toxicity, which will worsen with anti-arrhythmics and not respond to cardioversion.
- Regular, wide complex, driven by P waves is sinus tachycardia and requires treatment of the underlying cause (which may or may not be the reason it’s wide complex)
- Application: is there a secondary cause (eg for AF with rapid ventricular response, or sinus tachycardia)?
Back to the cases
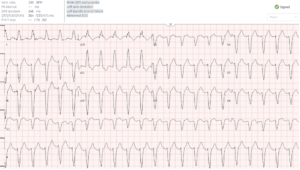
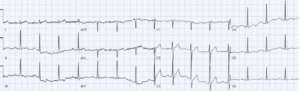
Case 1: 75yo with fever
- Heart rate/rhythm: normal sinus rhythm (P upright in the first complex of lead II), then artifact (with narrow complex QRS marching through the noise, best seen in lead V5 at the bottom)
- Electrical conduction: normal intervals
- Axis: appears left
- R-wave progression: difficult to tell
- Tall/small voltages: normal
- ST/T: difficult to tell
Impression: artifact. Repeat ECG:

–
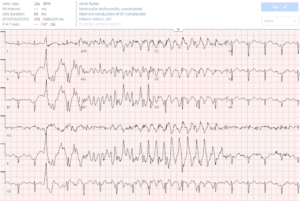
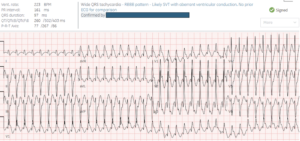
Case 2: 30yo with palpitations
- H: irregularly irregular rhythm (AF), with rates up to 300 with variable QRS morphology (accessory pathway)
- E: variable QRS
- A: variable axis
- R: normal
- T: tall
- S: secondary
Impression: AF + WPW, which is contraindication to AV node blockers including amiodarone. Patient electrically cardioverted into sinus rhythm, revealing delta waves (positive in most antero-latera leads and negative inferiorly):
–
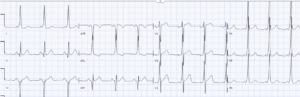
Case 3: 80yo weak/confused, with nausea/vomiting
- H: regular, really wide QRS (one large box or 200ms, with widening of both r and S waves) with normal rate, therefore not VT
- E: atypical LBBB morphology (based on R-wave progression)
- A: extreme
- R: no R wave progression
- T: normal voltages
- S: no specific changes
Impression: regular really wide non-tachycardic rhythm in patient with volume loss = hyperkalemia until proven otherwise, which will worsen with amiodarone or procainamide. Treated with empiric calcium, which restored sinus rhythm with narrow QRS, with peaked T waves (that later resolved after normalization of potassium):

–
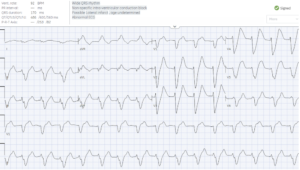
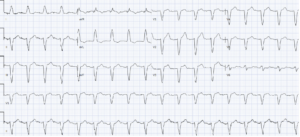
Case 4: 70yo with weakness
- H: regular wide complex tachycardia with preceding P waves = sinus tach
- E: atypical LBBB morphology
- Axis: left
- R-wave progression: no progression
- T: normal
- S: secondary
Impression: sinus tachycardia. Diagnosed with sepsis, tachyardia responded to fluids. Repeat ECG:
–
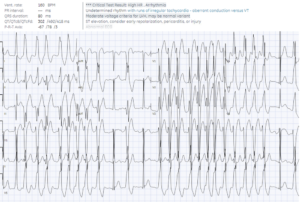
Case 5: 20yo with palpitations
- H: regular wide complex tachycardia without P waves = monomorphic VT until proven otherwise
- E: atypical RBBB (qR in V1, and wide R and S in V1)
- A: left axis with LAFB morphology
- R: early R in V1 from RBBB and persist S in V6 from LAFB
- T: tall
- S: secondary
Impression: rule out fascicular VT, vs SVT with bifascicular block. Electrically cardioverted into sinus rhythm, and EP studies confirmed fascicular VT
–
Take home messages for Stable Wide Complex Tachycardia
- Artifact can mimic wide complex tachycardia, but have unaffected leads recorded at the same time, and regular narrow QRS complexes marching through the noise: repeat the ECG
- Not regular, too wide/slow, or sinus
- Irregularly irregular: AF with rapid ventricular response, treat secondary causes, or cardiovert if it’s very rapid through an accessory pathway
- Too wide or not fast enough: consider hyperkalemia (empiric calcium) or sodium channel toxicity (empiric sodium bicarbonate)
- Regular wide complex tachycardia driven by P waves: treat the secondary cause of sinus tach
- VT vs SVT: if the wide complex tachycardia is regular and not driven by P waves, and the differential is VT vs SVT, assume VT regardless of age or hemodynamic instability (eg fascicular VT in young patients)
For live and highly interactive, CME-acccredited ECG courses to elevate your skills – including online courses, or an in-person pre-conference course at CAEP26, go to www.heartsECGcourse.com
References
- Linton JL, Eagles D, Green MS, et al. Diagnosis and management of wide complex tachycardia in the emergency department. CJEM 2022 Mar;24(2):174-184



Leave A Comment