
Topics in this EM Quick Hits podcast
Isaac Bogoch on tick borne illness update – anaplasmosis and babesiosis (1:30)
Matthew McArther on evidence-based update in nailbed repair (9:32)
Kathleen Stephanos on simplified approach to pediatric ECG interpretation (19:05)
Shawn Segeren on closed loop communication done right (30:36)
Brit Long on basic approach to end stage renal disease (36:02)
Catherine Varner & Victoria Myers on leadership and career choices in EM in our EM Leadership Spotlight series (44:08)
Podcast: Play in new window | Download (Duration: 1:00:21 — 55.3MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Anton Helman, August, 2025
Cite this podcast as: Helman, A. Bogoch, I. McArther, M. Stephanos, K. Segeren, S. Long, B. Myers, V. Varner, C. EM Quick Hits 67 – Tick Borne Illness Update, Pediatric ECG Interpretation, Nailbed Repair, Closed Loop Communication, ESRD, Leaders in EM Dr. Catherine Varner. Emergency Medicine Cases. August, 2025. https://emergencymedicinecases.com/em-quick-hits-month-year/. Accessed August 6, 2026.
Tick Borne Illnesses Beyond Lyme: Don’t Miss Co-Infections
Why it matters: Warmer, shorter winters are expanding tick ranges; Lyme is rising and under-reported. Same Ixodes ticks can transmit anaplasmosis and babesiosis—co-infection rates up to ~10–20% in highly endemic US regions. Think broadly.
When to test for tick borne illnesses
- If you’re ordering Lyme serology, also order anaplasma and babesia testing, especially with non-localizing febrile illness after tick exposure or travel from tick country.
- Erythema migrans: treat empirically for Lyme; serology may be negative early. Still send Lyme serology to aid downstream decision-making. Repeat if symptoms persist.
Treatment cues
- Anaplasmosis: often covered by your Lyme doxycycline course; clue = fever + leukopenia.
- Babesiosis: not covered by doxy; treat like malaria (e.g. atovaquone + azithromycin). Order specific testing.
Bottom line: If you thought “order Lyme,” add anaplasma + babesia—and tailor treatment if babesiosis is in play.
- Lantos PM, Rumbaugh J, Bockenstedt LK, et al. Clinical practice guidelines by the IDSA, AAN, and ACR: 2020 guidelines for the prevention, diagnosis and treatment of Lyme disease. Clin Infect Dis. 2021;72(1):e1-e48.
- Krause PJ, Auwaerter PG, Bannuru RR, et al. IDSA 2020 guideline on diagnosis and management of babesiosis. Clin Infect Dis. 2021;72(2):e49-e64.
- Biggs HM, Behravesh CB, Bradley KK, et al. Diagnosis and management of tick-borne rickettsial diseases: Rickettsia, Ehrlichia, and Anaplasma. MMWR Recomm Rep. 2016;65(2):1-44.
- Diuk-Wasser MA, Vannier E, Krause PJ. Coinfection by the tick-borne pathogens Babesia microti and Borrelia burgdorferi: ecological, epidemiological, and clinical consequences. Trends Parasitol. 2016;32(1):30-42.
Nail Bed Injuries: Faster, Simpler—Without Sacrificing Outcomes
Evidence refresh
- Skin glue vs sutures: Similar cosmetic/functional outcomes; skin glue is significantly faster.
- NINJA Trial (peds) & adult RCT: After standard nail bed repair, discarding the nail is as good as replacing/suturing it.
When to remove the nail to explore/repair
-
Deep laceration of proximal/lateral nail fold, mobile/lifted/split nail plate, or significantly displaced phalanx fracture. Intact margins → often no need to remove.
Take-homes
-
Consider skin glue for repair and discarding the nail post-repair—quicker with comparable outcomes.
- Strauss EJ, Weil WM, Jordan C, Paksima N. A prospective, randomized, controlled trial of 2-octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg Am. 2008;33(2):250-253.
- Jain A, Jones A, Gardiner MD, et al; NINJA Collaborative. Effectiveness of nail bed repair in children with or without replacing the fingernail: NINJA multicentre randomized clinical trial. Br J Surg. 2023;110(4):432-438.
- Greig A, Gardiner MD, Sierakowski A, et al. Randomized feasibility trial of replacing or discarding the nail plate after nail-bed repair in children. Br J Surg. 2017;104(12):1634-1639.
- Rock J, Kurland A, Congiusta DV, et al. Nail bed injury repair: nail plate replacement versus non-replacement. Eplasty. 2024;24:e37.
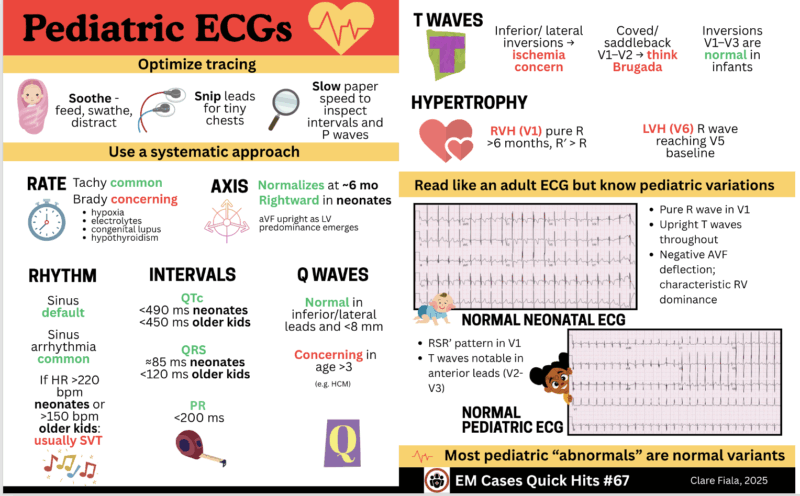
Pediatric ECGs: A Systematic Approach
Get a clean tracing: “Soothe · Snip · Slow”
-
Soothe (feed/swathe/distract), Snip leads for tiny chests, Slow paper speed to inspect intervals and P waves. Repeat if artifact.
Read it like an adult ECG—know the pediatric normals
- Rate: Tachy common; bradycardia is concerning—think hypoxia, electrolytes, congenital lupus, hypothyroidism.
- Rhythm: Sinus is default; sinus arrhythmia is very common. SVT is most actionable; rates >220 bpm neonates or >150 bpm older kids = usually SVT (often mistaken for VT).
- Axis: Rightward in neonates; by ~6 months aVF upright as LV predominance emerges.
- Intervals: Rough guides—QTc <490 ms neonates, <450 ms older kids; PR <200 ms; QRS <120 ms (≈85 ms neonates).
- Q waves: Normal inferior/lateral <age 3 if narrow and <8 mm; after age 3 these become concerning (e.g., HCM).
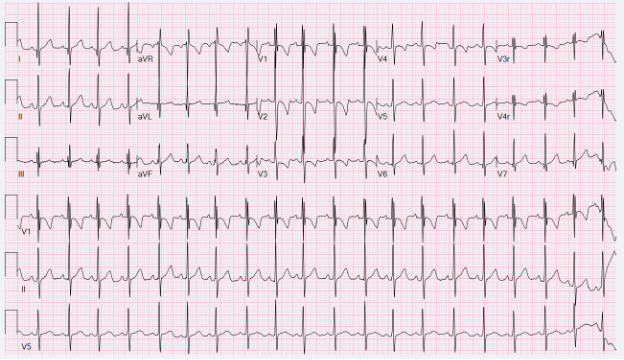
This normal pediatric ECG demonstrates many of the findings typical for a child- the RSR’ pattern seen in V1, the T waves notable in the anterior leads (V2-V3).
–
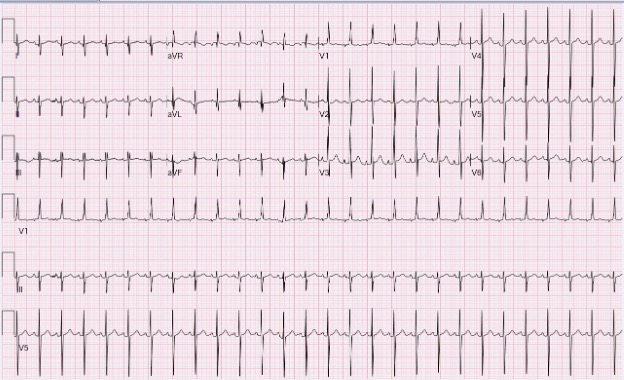
This normal neonatal ECG demonstrates the pure R wave in V1, the upright T waves throughout, and predominantly negative deflection of aVF characteristic of the right ventricular dominance in this age group.
-
Hypertrophy checks:
- RVH (V1): upright T after week 1, pure R after 6 months, or R′ > R.
- LVH (V6): R wave reaching the V5 baseline.
-
T waves: Inversions V1–V3 are normal beyond neonatal period; inferior/lateral inversions → ischemia concern; coved/saddleback V1–V2 → think Brugada.
Confidence boost: Most peds “abnormals” are normal variants—apply the framework above and slow the strip to find those P waves.
- Dickinson DF. The normal ECG in childhood and adolescence. Heart. 2005;91(12):1626-1630.
- Rijnbeek PR, Witsenburg M, Schrama E, Hess J, Kors JA. New normal limits for the paediatric electrocardiogram. Eur Heart J. 2001;22(8):702-711.
- Davignon A, Rautaharju P, Boisselle E, et al. Normal ECG standards for infants and children. Pediatr Cardiol. 1980;1(2):123-131.
Closed-Loop Communication That Actually Works
Not just “read-back.” Build a shared mental model.
Full loop steps (the practical version)
- Direct the order (“Alex, draw up 100 mg ketamine”).
- Receiver confirms (“Drawing up 100 mg ketamine”).
- Report readiness (“Ketamine ready—give now?”).
- Green light from prescriber.
- Call it out when done (“100 mg in”).
- Document aloud (time/dose).
Why teams fail: Skipped confirmations in fast resus → surprise med pushes, confusion, duplication. Even partial structure (directed orders + clear confirmations + call-outs) reduces errors; deliberate simulation practice is key.
- Abd El-Shafy I, Doumit M, AkI T, et al. Closed-loop communication improves task completion in trauma resuscitations. J Surg Educ. 2017;74(4):627-632.
- Diaz MCG, Dawson K. Impact of simulation-based closed-loop communication training on medical errors in a pediatric emergency department. Am J Med Qual. 2020;35(5):474-478.
- Gjøvikli K, Hovland N, Pillgram-Larsen J, et al. Closed-loop communication in interprofessional emergency teams: an observational study. J Interprof Care. 2023;37(4):613-621.
ESRD & Dialysis in the ED: A Quick Primer
Scope: >500,000 on dialysis in the US; Hemodialysis most common; Peritoneal dialysis (PD) ~7%. Access = AV fistula (best), graft, or CVC (highest infection/clot risk).
Important complications to screen for: Infection, fluid overload, cardiovascular disease (HF/MI/pericarditis), neurologic (uremia, subdural), anemia/thrombosis, peritonitis (PD).
History checklist
- Uremic symptoms? Missed dialysis?
- Cause of ESRD, urine output, native kidneys.
- Dialysis type/schedule/adherence, recent complications.
- Dry weight, usual vitals/labs (Hgb).
- Access issues/manipulations; for PD: exchanges, dwell times, dialysate concentration.
Exam essentials
- Assess volume (lungs/edema, bedside US helpful).
- Access site: bruit/thrill, erythema, warmth, tenderness, bleeding/ulcer.
- Neuro (subtle encephalopathy—ask family).
- PD: abdominal tenderness, catheter site infection, hernia.
On shift framing: Stabilize first, then run the focused ESRD Hx/Exam to triage volume/infection/complication drivers and coordinate with dialysis team.
- Long B, Koyfman A, Lee CM. Emergency medicine evaluation and management of the end stage renal disease patient. Am J Emerg Med. 2017;35(12):1946-1955.
- West J, Chan HK, Wang H, et al. Emergency department visits for hemodialysis by insurance status in the United States. JACEP Open. 2022;3(2):e12698.
- Wang N, Pei J, Fan H, et al. Emergency department use by patients with end-stage renal disease in the United States. BMC Emerg Med. 2021;21(1):25.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Kidney disease statistics for the United States. Accessed August 2025.
None of the authors have any conflicts of interest to declare



Great review on tick related illness. We have seen A LOT of anaplasmosis in Kingston, ON this summer. Look for the leukopenia + thrombocytopenia as clue with sx of fever, myalgias, headache, nausea and have been in tick endemic area. Patients don’t always have a known bite.