
Topics in this EM Quick Hits podcast
Justin Morgenstern on when to consider cerebral venous thrombosis (00:53)
Maria Ivankovic on diphenhydramine alternatives (07:38)
Brit Long on abdominal compartment syndrome (13:13)
Sarah Reid on neonatal constipation (19:37)
Anand Swaminathan on intubating metabolic acidosis (27:40)
Podcast: Play in new window | Download (Duration: 34:31 — 31.7MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman; voice editing by Raymond Cho
Podcast content by Justin Morgenstern, Maria Ivankovic, Brit Long, Sarah Reid, Anand Swaminathan & Anton Helman
Written summary & blog post by Graham Mazereeuw, edited by Anton Helman
Cite this podcast as: Helman, A. Morgenstern, J. Ivankovic, M. Long, B. Reid, S. Swaminathan, A. EM Quick Hits 25 – Cerebral Venous Thrombosis, Diphenhydramine Alternatives, Abdominal Compartment Syndrome, Neonatal Constipation, Intubating Metabolic Acidosis. Emergency Medicine Cases. January, 2021. https://emergencymedicinecases.com/em-quick-hits-january-2021/. Accessed [date].
When to Consider Cerebral Venous Thrombosis
Presentation is nonspecific and highly variable:
- Headache in nearly all patients (the only symptom in 25% of patients)
- Other features: focal neurological deficit (40%), seizure (40%), encephalitis (rarely)
Key demographics:
- Young (39 years old on average)
- Female (3x more commonly)
- Usually at least one thrombotic risk factor
Consider this diagnosis in 4 groups of patients:
Group 1: severe or prolonged headache without a clear cause and with at least one thrombotic risk factor
Group 2: thunderclap headache with a negative CT head
Group 3: severe headache with stroke symptoms or neurological findings not clearly mapping to a vascular territory
Group 4: intracranial hemorrhage without a classic bleeding pattern, particularly younger patients or those with thrombotic risk factors
-MR venogram is gold standard; contrast CT venogram has good sensitivity (95%)
-Treat the sequelae (ABCs, treat seizure, treat raised ICP)
-Specific treatment is anticoagulation (even if intracranial hemorrhage!) in consultation with neurology/hematology
-Full recovery = 80%; 30-day mortality = 5%
Bottom line: CVT is the DVT of the brain; be on high alert for CVT in patients with thrombotic risk factors and atypical headache or stroke symptoms.
Episode 14 Part 2: Thunderclap Headache – Cerebral Venous Thrombosis and Cervical Artery Dissection
- Tadi P, Behgam B, Baruffi S. Cerebral Venous Thrombosis. [Updated 2020 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459315/
Diphenhydramine Alternatives
- First-generation antihistamines are “dirty drugs”: diphenhydramine and hydroxyzine have poor receptor selectivity, binding muscarinic, serotonergic, and alpha-adrenergic receptors, as well as cardiac potassium channels in addition to the H1 histamine receptor
- First-generation antihistamines side effects:
- CNS suppression, psychomotor impairment, delirium, coma, and death
- QT prolongation and torsades de pointes
- Recreational misuse (“Benadryl challenge” parties)
- A therapeutic dose of diphenhydramine (50mg) can impair driving similarly to a 0.1% blood-alcohol level (4-5 alcoholic drinks in some people)!
- Second-generation antihistamines are generally safer: less likely to have drug-drug interactions, faster onset, much less sedating
- A second-generation antihistamine is a reasonable (perhaps superior) alternative for post-anaphylaxis urticaria without the potential side-effects of diphenhydramine
Bottom line: First-generation antihistamines such as diphenhydramine and hydroxyzine have multiple side effects and can be replaced by second-generation antihistamines for allergy and post-anaphylaxis urticaria.
- Fein MN, Fischer DA, O’Keefe AW, Sussman GL. CSACI position statement: Newer generation H1-antihistamines are safer than first-generation H1-antihistamines and should be the first-line antihistamines for the treatment of allergic rhinitis and urticaria. Allergy Asthma Clin Immunol. 2019;15:61.
- Fischer, D., Vander Leek, T.K., Ellis, A.K. et al.Allergy Asthma Clin Immunol 14, 54 (2018). https://doi.org/10.1186/s13223-018-0283-4
- Cook VE, Chan ES. Anaphylaxis in the acute care setting. CMAJ. 2014;186(9):694.
- Huynh DA, Abbas M, Dabaja A. Diphenhydramine Toxicity. [Updated 2020 Oct 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557578/
Abdominal Compartment Syndrome
- Abdominal compartment syndrome is a potentially deadly condition caused by increased pressure within the abdominal compartment and is most often diagnosed in the ICU
- Abdominal compartment syndrome is defined by intra-abdominal pressure (IAP) > 20 mm Hg with organ dysfunction
- Suspect abdominal compartment syndrome in penetrating abdominal trauma and post open abdominal surgery with abdominal pain out of proportion, abdominal distension and shortness of breath/increase work of breathing; note that these findings are not accurate for diagnosis, making the clinical diagnosis challenging
- History, physical examination, labs and imaging may suggest the diagnosis, but they should not be used to exclude it
- Diagnosis: IAP measurement, typically through measuring bladder pressure with a Foley catheter
- Management: increase abdominal wall compliance, evacuate gastrointestinal contents, avoid excessive fluid resuscitation, drain intraperitoneal contents, and decompressive laparotomy in select cases; patients typically require admission to an ICU
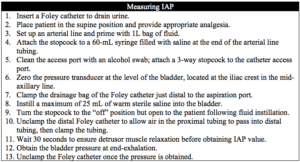
Procedural video measuring intra-abdominal pressure
Bottom line: Consider abdominal compartment syndrome in critically ill patients with multi-organ failure; measure intra-abdominal pressure through the bladder using a Foley catheter.
- Papavramidis TS, Marinis AD, Pliakos I, Kesisoglou I, Papavramidou N. Abdominal compartment syndrome – Intra-abdominal hypertension: Defining, diagnosing, and managing. J Emerg Trauma Shock. 2011 Apr;4(2):279-91.
- Sosa G, Gandham N, Landeras V, Calimag AP, Lerma E. Abdominal compartment syndrome. Dis Mon. 2019 Jan;65(1):5-19.
- Maluso P, Olson J, Sarani B. Abdominal Compartment Hypertension and Abdominal Compartment Syndrome. Crit Care Clin. 2016 Apr;32(2):213-22.
- Sugrue M, De Waele JJ, De Keulenaer BL, Roberts DJ, Malbrain ML. A user’s guide to intra-abdominal pressure measurement. Anaesthesiol Intensive Ther. 2015;47(3):241-51.
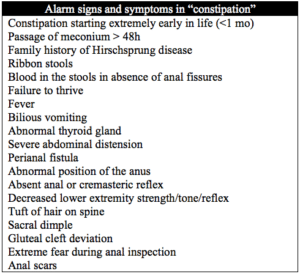
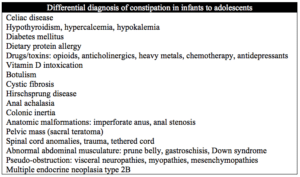
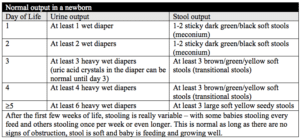
Neonatal “Constipation” Red Flags, DDx and ED Management
- Poor stooling in a newborn is common and often triaged as “constipation”; however, it is most often a result of breastfeeding not being fully established
Management:
- Fractionated bilirubin if concerns about feeding, hydration or weight loss; use bilitool.org to determine the need for phototherapy or exchange transfusion
- Abdominal X-ray with two views if concern for obstruction (bilious vomiting, abdominal distension) if you don’t have other imaging modalities available
- IV fluid resuscitation with strong consideration of full septic workup and empiric antibiotics in any newborn who is lethargic, dehydrated, appears unwell
Disposition:
- Home if: baby is well and there are no red flags; parents are comfortable with increasing feeds, stimulating baby to stay awake during feeds, seeking close follow up with primary care (in next 1-2 days for weight check)
- Admission to paediatrics if: baby is significantly dehydrated, weight loss ³ 10%, concern about underlying abnormality on exam, or social concerns
- General surgery consultation if: concerned about obstruction, Hirschsprung disease, or anal abnormalities
Bottom line: “constipation” in a newborn is likely attributable to ineffective breastfeeding, but be sure to assess for red flags and rule out serious illness
- Tabbers MM, DiLorenzo C, Berger MY, Faure C, Langendam MW, Nurko S, et al. Evaluation and Treatment of Functional Constipation in Infants and Children: Evidence-Based Recommendations from ESPGHAN and NASPGHAN. JPGN 2014;58: 258–274.
- https://www.parentinginottawa.ca/en/breastfeeding/Breastfeeding-in-the-Early-Weeks.aspx
- https://www.albertahealthservices.ca/assets/info/nutrition/if-nfs-ng-healthy-infants-gi-function-management-constipation.pdf
- EM Cases Episode 19 Part 2: Pediatric Gastroenteritis, Constipation and Bowel Obstruction, https://emergencymedicinecases.com/episode-19-part-2-pediatric-gastroenteritis-acute-constipation-bowel-obstruction/
Intubating Patients with Metabolic Acidosis: Apnea Time and Minute Ventilation
- Patients with metabolic acidosis employ a compensatory respiratory alkalosis, which they rely on for pH management
- Apnea induced during intubation impairs this compensation, which can lead to peri-intubation cardiac arrest
- If intubation is necessary, minimize apneic time and ensure adequate minute ventilation
- Approach
-
- Resuscitate the underlying problem/consider NaHCO3 IV drip
- Start NIPPV, which can support the patient and estimate minute ventilation (which you will need when setting the ventilator)
- Consider an awake intubation to maintain ventilation; use ketamine if unable to topically anesthetize the airway (consider KOBI); if RSI needed, use succinylcholine to minimize time of paralysis
- It is critical to maintain pre-intubation minute ventilation in order to maintain pH balance
- If unable to do this on a ventilator, provide pressure support while the patient breathes on their own, or bag-mask ventilate them to the minute-ventilation required
Bottom line: Avoid intubation if you can in the severely acidotic patient; if you must intubate, be sure to minimize apnea time and support minute ventilation to pre-intubation levels.
- Definitive Emergent Awake Intubation with George Kovacs, EMCrit-RACC, podcast 194. https://emcrit.org/emcrit/definitive-emergent-awake-intubation/
- Weingart, S. Podcast 3 – Laryngoscope as a Murder Weapon (LAMW) Series – Ventilatory Kills – Intubating the patient with Severe Metabolic Acidosis. https://emcrit.org/emcrit/tube-severe-acidosis/
None of the authors have any conflicts of interest to declare



Great episode, thank you so much.
One question, what about intubation in a patient with severe metabolic acidosis due to status epilepticus?