

Most of us in North America live in cultures that almost never talk about death and dying. And medical progress has led the way to a shift in the culture of dying, in which death has been medicalized. While most people wish to die at home, every decade has seen an increase in the proportion of deaths that occur in hospital. Death is often seen as a failure to keep people alive rather than a natural dignified end to life. This is at odds with what a lot of people actually want at the end of their lives: 70% of hospitalized Canadian elderly say they prefer comfort measures as apposed to life-prolonging treatment, yet as many as ⅔ of these patients are admitted to ICUs.
Podcast: Play in new window | Download (Duration: 1:07:49 — 62.1MB)
Subscribe: Apple Podcasts
Written Summary and blog post Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Sept 2015
Discussing End of Life Care in Emergency Medicine
Find a quiet room to have end of life discussions. In an unresponsive patient, find a room where the patient cannot hear the discussion. It is prudent to assume the unconscious patient hears everything (1).
Allow patients and/or their families the time to tell their story so you can understand it. Avoid power struggles with families. It is often prudent to provide your clear medical opinion, and when appropriate, make clear recommendations rather than giving options only and leaving end of life decisions to family alone. This may help reduce the burden of this difficult decision on the family.
See Episodes 49 and 51 on effective patient communication and managing difficult patients.
Palliative Care Myth #1: Code status discussion should focus on descriptions of CPR/CCR
In discussions regarding goals of care and code status, talking about the risk of broken ribs will not help you, the patient and their family get any closer to effective decisions about goals of care. Rather, discussions around goals of care ![]() should include information regarding overall prognosis, patient goals, and explanations of different levels of care.
should include information regarding overall prognosis, patient goals, and explanations of different levels of care.
An informed decision involves sharing realistic expectations. The common and uncommon material risks of CPR/CCR and treatment (2) may include:
- Incomplete recovery
- Prolonged death
- Uncomfortable investigations and treatments
- Ventilator dependence
Do Not Resuscitate (DNR) Orders in End of Life Care in Emergency Medicine
Palliative Care Myth #2: DNR means do not treat
DNR means no resuscitation in the setting of a full cardiopulmonary arrest. This is often misinterpreted, and sometimes associated with lower quality or less care. Patients can and should still receive full and aggressive medical management even if they are rendered DNR.
There is a movement, as stated in the AHA Cardiopulmonary Resuscitation Guidelines in 2010, towards changing the DNR order to ‘Allow Natural Death’ (AND). AND uses positive language, stating what we will do, as opposed to what we will not do. Patients and their families may feel less guilt and may be more likely to be agreeable to an AND order than to a DNR order.
Discussing Prognosis in End of Life Care in Emergency Medicine
There are multiple barriers to communicating prognosis which include:
- Physicians in general are poor prognosticators: ED physicians in particular do not have experience taking care of patients over time in their trajectory towards death
- There is uncertainty in medicine: uncertainty should be communicated with patients, this also leads to the patient’s increase in sense of trust with the health care team
- ED physicians often feel a lack of ownership/responsibility regarding end of life discussions, as it is thought to be the responsibility of the primary care physician
- Lack of skill in communication of prognosis
- We assume patients do not want to know their prognosis; however, it has been shown that the majority of patients do want to know their prognosis.
Palliative Care Myth #3: It is the primary care physician’s role to discuss end of life issues
End of life discussions and issues around prognosis and palliative care are appropriate in the ED, and often lead to more appropriate care pathways from the ED.
Models for Prognostication in End of Life Care
There are two models of death, which can help ED physicians prognosticate for patients. The first one describes the final hours-days and the second one describes the final months-years.
The ‘Two Roads to Death’ Model (Fig 1):
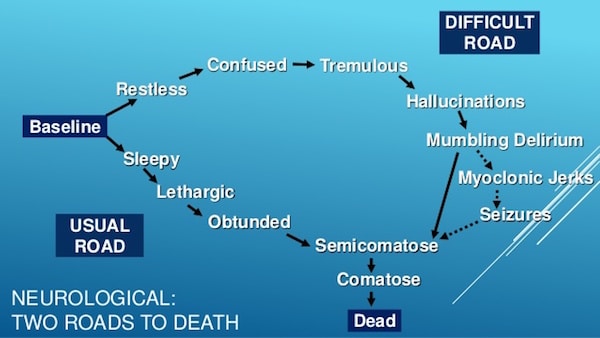
- Usual Road: In this pathway, patients are sleepy, lethargic, obtunded and then progress towards death. Death typically occurs quickly.
- Difficult Road: In this pathway, patients are restless, confused, develop hallucinations, delirium, may develop seizures, and ultimately progress towards death. In this pathway, death is typically prolonged and more difficult.
Trajectory of Illness Model (Fig 2): This model allows one to prognosticate death based on illness diagnosis, and over a longer period of time. There are four different categories of dying.
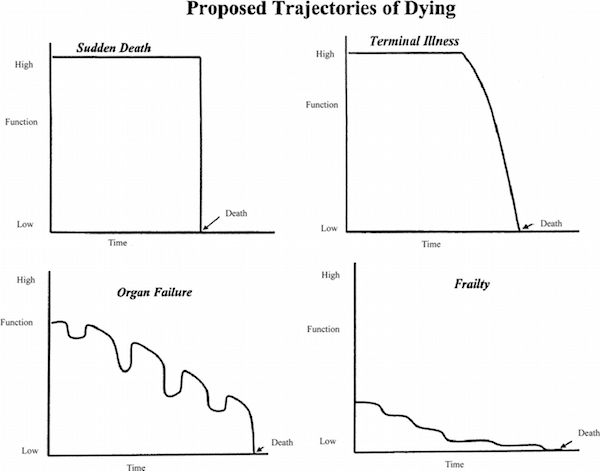
- Sudden Death: In this trajectory, patients have not been ill, and there is nothing to predict anything bad will happen. Patients suddenly become critically ill or injured and die. (i.e. sudden massive MI, traumatic injury, etc.)
- Frailty: In this trajectory, patients die of ‘old age’, and have a slow and gradual decline. These patients may or may not develop a severe illness, but slowly decline in mobility, function and/or cognition, and ultimately die from a complication of their progressive disability.
- Terminal Illness: In this trajectory, it is expected that patients will have a prolonged illness where they can generally maintain their function, until the end of life, when function sharply drops off. (i.e. cancer)
- Organ Failure: In this trajectory, there is a relatively steep decline in function with intermittent exacerbations. Patients ultimately die during one of these exacerbations, and if they survive, they never reach their prior level of function. (i.e. heart failure, COPD)
Prognostic Signs at the End of Life
Besides the obviously crashing patient, there are multiple signs on physical exam that can give us clues that a patient is near death. Some of these signs include:
- Delirium with hypotension and tachycardia: median survival 10 days
- Death rattle: medial survival 1 day
- Respirations with mandibular movement: median survival 2.5 hours
- Cyanosis to extremities: medial survival 1 hour
Palliative Care Myth #4: Making a patient palliative results in shortened survival
Early palliative care in multiple studies has been shown to prolong survival.
Approach to End of Life Communication
Do’s:
- Introduce yourself, give information that you have reviewed
- Ask ‘what is your understanding of your loved one’s illness, their quality of life?’
- Ask ‘what were you hoping we can do for your loved one?’
- Ask what patients/families are most afraid of
- Ask ‘if your loved one were to die tomorrow, what would they want us to accomplish before that?’
Don’ts:
- Get into arguments
- Power struggle

A useful mnemonic for end of life communication is the SILVER mnemonic:
Seeks Information:
- Elicits information regarding baseline level of function, behaviours, and symptoms that suggest progressive decline
- Elicits information regarding current diagnosis, prognosis, and treatment plan
- Elicits information regarding key players in decision making, including family and health care workers
- Elicits information regarding previous end of life discussions, including advance directives
Life Values
- Elicits information regarding the patient’s personality and approach to life
- Elicits information regarding how the patient views death and dying
Educates/Extends Care
- Provides information regarding the patient’s disease process, current condition, and treatment options
- Explains how end of life decisions will impact further treatment
Responds
- Solicits questions from family and offers continued support and availability for further information.
For more on tips for discussing end of life issues see this great post by Justin Morgenstern on First 10 EM: Breaking Bad News – Notifying Family Members of a Death in the Emergency Department
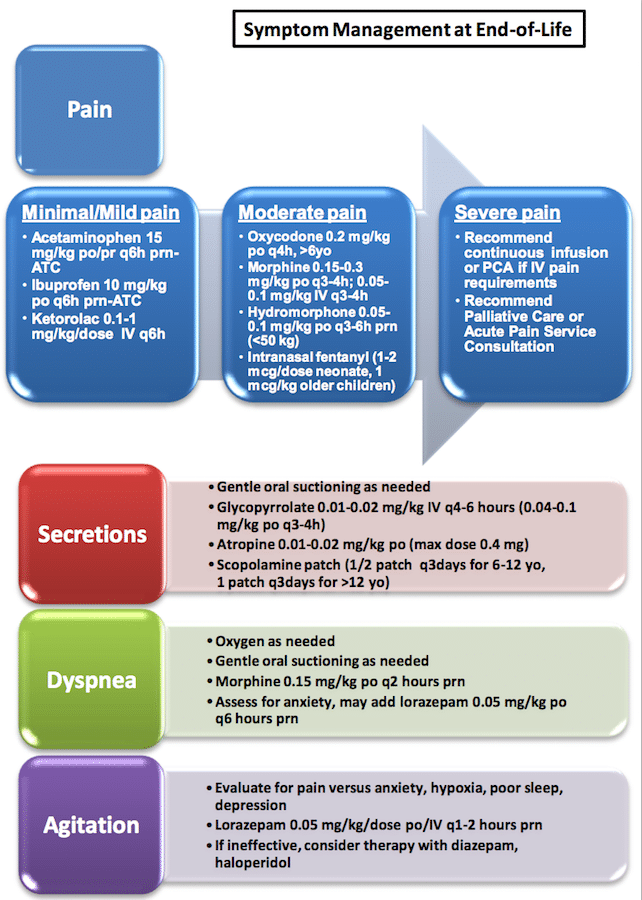
Symptom Management in the Palliative Patient
Pain
Obtain an analgesia history and convert narcotics into morphine daily dose (MDD). Use a calculator for the conversion (there are multiple online calculators available). When switching from oral to IV, reduce the IV dose by 25% as a starting point. Titrate medications frequently: consider a 50% increase every 15-30 minutes.
- Consider NSAIDs
- Consider corticosteroids
- SQ route and butterfly needles are reasonable options
- Ketamine is not routinely recommended at this time by our experts in the palliative patient for pain control as it may cause emergence reactions
Dyspnea
Opioids decrease the sensation of being shortness of breath. They are used for dyspnea at much smaller doses than they are for pain control (e.g. 0.5 – 2mg morphine IV).
Palliative Care Myth #5: Opioids hasten death
Studies have shown that O2 and CO2 levels stay the same despite the decreased respiratory rate associated with opioids. Opioids in the palliative patient are appropriate and ethically permissible as long as the intent is symptoms relief.
Consider adjuvant therapies for dyspnea:
- Oxygen – although studies have failed to show comfort-oriented benefit of supplemental oxygen in the dying patient, our experts recommend it as it often makes families more comfortable
- Non-invasive Positive Pressure Ventilation (BiPAP or CPAP)
- A fan blowing air in the patient’s face has been shown to improve the dying patient’s comfort
![]() Update 2021: Randomized, crossover study of 48 palliative adult patients with hypoxemic respiratory failure with do-not-intubate (DNI) status in an ED (Bangkok, Thailand) . Compared high-flow nasal cannula (flow rate 30-60 L/min) and conventional oxygen therapy (with non-rebreather mask); targeting >95% oxygen saturation in both cases. High-flow nasal cannula was superior in reducing dyspnea severity (according to modified Borg scale), improved respiratory rate, and required lower initial doses of morphine. Abstract
Update 2021: Randomized, crossover study of 48 palliative adult patients with hypoxemic respiratory failure with do-not-intubate (DNI) status in an ED (Bangkok, Thailand) . Compared high-flow nasal cannula (flow rate 30-60 L/min) and conventional oxygen therapy (with non-rebreather mask); targeting >95% oxygen saturation in both cases. High-flow nasal cannula was superior in reducing dyspnea severity (according to modified Borg scale), improved respiratory rate, and required lower initial doses of morphine. Abstract
Secretions
- Re-position the patient
- Suction the upper airway
- Medications:
- Glycopyrrolate 0.2mg
- Scopolamine patch (delayed onset)
- 1-2 drops of 1% atropine eye drops under the tongue
Terminal Delirium
Terminal delirium at the end of life is fairly common and may include moaning, restlessness, and agitation. Terminal delirium is difficult for families to watch. It should be treated aggressively and early. Treatment options include:
- Benzodiazepines: In adults, start with midazolam 1-4 mg IV, with frequent reassessments
- Haloperidol: 0.5-2 mg IV, with frequent reassessments
![]() For more on end of life care on EM Cases:
For more on end of life care on EM Cases:
Best Case Ever 40 End of Life Care & Consultant Communication
Key References
- You JJ, Fowler RA, Heyland DK . 2013. Just ask: Discussing goals of care with patients in hospital with serious illness. CMAJ; 186(6): 425-32. Full pdf
- Diem SJ, Lantos JD & Tulsky JA. 1996. Cardiopulmonary resuscitation on television: Miracles and misinformation. NJEM; 334: 1578-82. Full pdf
- Lunney JR, Lynn J, Foley DJ, et al. 2003. Patterns of functional decline at the end of life. JAMA; 289: 2387-2392. Full pdf
- Howey, L, Peppercorn, J. 2013. Early palliative care in cancer treatment: rationale, evidence and clinical implications.Ther Adv Med Oncol. 2013 Nov; 5(6): 318–323. Abstract
Quote of the Month
”Cure sometimes, treat often and comfort always”
-Hippocrates
Dr. Helman, Dr. Ovens, Dr. Miller and Dr. MacLachlan have no conflicts of interest to declare
Other FOAMed Resources on End of Life Care
End of Life Care in the Emergency Department Order Set from Mount Sinai Hospital, Toronto
Choosing Wisely Canada’s patient hand-out on End of Life Care for cancer patients
Great post by Justin Morgenstern on First 10 EM: Breaking Bad News – Notifying Family Members of a Death in the Emergency Department



[…] Medicine Cases has an excellent review of End of Life Care in EM. […]
Great podcast!
Just a thought:
Instead of “AND” allow natural death, – in which the word “allow” implies to me an element of complacency, I suggest “OND” – optimize natural death.
Yes! That perfectly describes the active (as apposed to passive) management of end of life and that we should be striving for the best care possible.
Hi Anton. Another great episode. Thanks for delving into this topic. Really liked the questioning of DNR concept and how it often leads to “do no treat”. I firmly believe that if a patient actively receives palliative care in the community then they deserve good care in the ED too. Also I think DNR tends to have health care staff be less aggressive even in the setting on curable entities (ie sepsis or GIB unrelated to a patient’s underlying disease) – these still deserve optimal management even if intubation/ICU is not in the patient’s care plan.
Do you or your guests happen to have an ED pre-printed order set for palliative care? I’d love to introduce one to my department.
-Elisha
Thanks for your comments Elisha. There is a link to the order set for end of life care in the ED at the bottom of the blog post. Let me know if you need any further information and I can ask Howard Ovens.
beautifully put..goldmine for ppl like me who are just about transitioning into registrarship..thank you for your work
Thanks very much for all your episodes, and this one in particular. It was a terrific discussion, particularly the comments on the problems with active care directives, explaining the possible trajectories, and use of the term ‘allow natural death’.
This is an amazing podcast would you believe u got this same question in my Emerg DM Exam. Gave me a lot of clarity.