

Dr. Joel Yaphe, University of Toronto’s Emergency Medicine Residency Program Director and Dr. Indy Ghosh discuss the difficult diagnostic dilemmas when faced with a patient with acute monoarthritis. They review how to distinguish clinically between septic arthritis and gout and which aspects of the presentation and work-up are the most reliable in risk stratifying patients. The key differential diagnosis of Acute Polyarthritis can be even more of a challenge, but fear not: by then end of this podcast and post you will be able to recognize the key diagnoses, how to work them up, and who needs consultation.
Joel Yaphe and Indy Ghosh discuss such questions as: What are the most predictive signs and symptoms of septic arthritis? How does serum WBC, ESR and CRP contribute to the probability of septic arthritis? Should we still be performing arthrocentesis on patient’s with overlying cellulitis? How can you tell the difference between septic bursitis and septic arthritis? What does the literature tell us about how useful the synovial fluid tests are in ruling in or ruling out septic arthritis? What is the role of bedside ultrasound in septic arthritis? Is there a role for steroid therapy in septic arthritis? When would you consider oral NSAIDs vs oral prednisone vs intra-articular methylprednisolone for the treatment of Gout? Is there a role for colchicine in the ED treatment of Gout (AGREE Trial)? What is acute calcific arthritis of hydroxyapatite disease? How can one distinguish Reactive Arthritis from Septic Arthritis clinically? and many many more…..
Podcast: Play in new window | Download (Duration: 1:21:58 — 65.7MB)
Subscribe: Apple Podcasts
Written Summary and blog post by Lucas Chartier, edited by Anton Helman July 2011
Cite this podcast as: Yaphe, J, Ghosh, I, Helman, A. Acute Monoarthritis. Emergency Medicine Cases. July, 2011. https://emergencymedicinecases.com/episode-16-acute-monoarthritis/. Accessed [date].
ACUTE MONOARTHRITIS
Most Common Causes of Acute Mono-arthritis: Crystal Arthritis (Gout & Pseudogout), Septic Arthritis, Occult Trauma
=> Challenge is that presentations overlap and that there sometimes remains diagnostic uncertainty even after aspiration of the joint
Update 2014: For an excellent review of the JAMA Clinical Examination Series article on LRs for physical exam findings in septic arthritis (in the reference list at the bottom of this post) go to SINAIEM
Non-Gonococcal Septic Arthritis
- Classically presents with an acute hot swollen knee or ankle, constitutional symptoms including fever, non- weight bearing with severe pain on passive ROM of the joint. However, septic arthritis can occur in any joint, can occur in the absence of fever, and subtle signs typically occur in immunocompromised and elderly patients.
- Mortality: reported as 10-30% although probably lower than this in practice
- Morbidity: local joint destruction, sepsis, osteomyelitis, growth impairments
- Risk Factor Triad: Pre-existing joint disease (RA, gout etc), loss of Skin Integrity (intra-articular injections, ulcer, IVDU, dialysis), immunocompromised state (DM, steroid use, HIV etc)
- Distinguishing RA flare from Septic Arthritis: in the context of pre-existing arthritis, the affected joint or joints will usually show sings that are out of proportion to disease activity detected in other joints. However, joint aspiration is usually required to definitively distinguish septic arthritis from an arthritis flare.
- Blood work for septic arthritis: serum WBC +LR only 1.4, ESR >30 +LR only 1.3, CRP >100 only 1.6
- One study showed that the sensitivity of an ESR
- Normal ESR calculation: in males = Age/2, females = Age +10/2
- => no single blood test can rule in or out septic arthritis in the vast majority of patients with mono-arthritis
- Because the most common source of infection in septic arthritis is from hematogenous spread, it is important to do blood cultures in patients with systemic symptoms. Blood cultures will be the only source of a positive bacterial diagnosis in 10% of patients with septic arthritis (ie the joint blood culture may be negative, while the blood culture is positive in some patients)
- How to distinguish Septic Bursitis (image below) from Septic Arthritis: bursitis is extra-articular so pain is not in all planes of joint motion. Our experts recommend aspiration of bursitis that you suspect is infectious because if the patient rapidly improves and the culture is negative, a prolonged course of antibiotics can be avoided.

Arthrocentesis for Acute Monoarthritis
- Arthrocentesis is an essential emergency medicine skill that is often diagnostic as well as therapeutic (relieves pain and is part of the treatment in septic arthritis), and has a very low complication rate.
- Emergency bedside ultrasound was found to decrease pain, total time of procedure and physicians find it easier to perform in a small RCT. For inaccessible joints such as the hip, an ultrasound can be very useful in identifying a joint effusion.
- Contra-indications to arthrocentesis: consider consult before arthrocentesis if there is an obvious cellulitis overlying the joint in question, prosthetic joint or post-op joint. Most experts will do an arthrocentesis on patients with an elevated INR or a known bleeding disorder but the risks and benefits need to be weighed on an individual basis.
Joint Fluid Analysis in Acute Monoarthritis
- Joint WBC and PMNs are the 2 most important lab tests for septic arthritis. The higher the joint WBCs the more likely septic arthritis and the lower the joint WBC the less likely, but strict cut-offs should not be used because studies have shown that about 1 in 4 patients with septic arthritis will have a joint WBC <40,000.
- WBC <25,000 (negative LR = 0.32 for septic arthritis); WBC >25,000 (positive LR = 2.9 for septic arthritis); WBC>50,000 (positive LR = 7.7 for septic arthritis)
- PMNs >90% (positive LR = 3.4) vs PMNs <90% (negative LR = 0.34)
- Gram stain sensitivity = 50% and Culture sensitivity = 80%
- The finding of crystals on joint fluid aspiration does not rule out septic arthritis as 1.5% of patients with arthrocentesis proven crystal disease had concurrent septic arthritis in one study (JEM, 2007 Jan;32(1):23-6).
- => While there is no single symptom, signs, blood test or joint fluid finding that can definitively rule in or out septic arthritis, patients can be risk stratified (as we do with chest pain patients). Note – this is a retroactive study, so the evidence is relatively weak
![]() Update 2022: A multicenter retrospective study of 598 adult patients diagnosed with septic arthritis found that synovial fluid neutrophil-to-lymphocyte ratio was significantly more accurate for the diagnosis of septic arthritis compared to traditional diagnostic criteria using synovial fluid WBC count and PMN ratio. (Note – this is a retroactive study, so the evidence is relatively weak) Abstract
Update 2022: A multicenter retrospective study of 598 adult patients diagnosed with septic arthritis found that synovial fluid neutrophil-to-lymphocyte ratio was significantly more accurate for the diagnosis of septic arthritis compared to traditional diagnostic criteria using synovial fluid WBC count and PMN ratio. (Note – this is a retroactive study, so the evidence is relatively weak) Abstract
Update 2015: Predictive value of the usual clinical signs and laboratory tests in the diagnosis of septic arthritis CJEM
Excerpt from 2015 CJEM paper

Treatment of Septic Arthritis
- Staph Aureus is the most common pathogen
- For patients with Gram Stain showing gram positive bacteria: Vancomycin 1g IV (to cover for MRSA)
- For patients with Negative Gram Stain: Ceftriaxone 2g + Vancomycin 1g IV
- Systemic Steroids for Septic Arthritis: While there have been small RCTs in the pediatric population showing more rapid clinical improvement and decreased length of stay with IV Dexamethasone in hip septic arthritis, there is no evidence in adult septic arthritis for the use of systemic steroids, so no recommendations can be made at present.
- Definitive Management: Serial closed needle aspiration has been shown to be as effective as open drainage of the joint where the joint is accessible and adequacy of drainage can be assessed.
- Indications for surgery in septic arthritis: (open drainage or laprascopic lavage) prosthetic joint, large purulent effusion, joints that are difficult to access, when there is lack of improvement with needle aspiration
Gonococcal Septic Arthritis
- Variable Presentations: often younger patients with STI risk factors with isolated monoarticular acute arthritis or polyarticular arthritis with dermatitis, tenosynovitis and migratory polyarthritis
- Clinical clue: significant periarticular inflammation
- Work-up: Urethral, rectal, pharyngeal and skin swabs should be done in all patients suspected of GC arthritis in addition to joint aspiration, as the culture yield on joint fluid is very low and the bacterial diagnosis is most often made from a distant site.
- Treatment: IV Ceftriaxone 2g q24h until symptoms improve, then switch to oral cephalosporin for minimum of 7 days, plus treat for chlamydia (doxycycline or azithromycin) and notify public health office as well as contacts for assessment.
Gout
- Dutch JAMA Study: Male, previous arthritis attack, onset within 24hrs, HTN, hyperuricemia, joint redness, 1st MTP involvement makes Gout a likely diagnosis
- Other Risk Factors: beer and liquor intake (not wine), red meat, diuretic use
- An elevated Uric Acid level in the ED patient with an acute mono-arthritis, while increasing the likelihood of the mono-arthritis being caused by gout, has PPV and NPV that are not good enough to rule in or out the diagnosis with certainty and our experts don’t find it useful in their decision making.
- Elderly patients with gout: more likely to have polyarticular gout, a more indolent course, tophi and upper extremity involvement.
- Treatment Options for Gout:
-
- NSAIDs (eg Indomethacin or Naproxen minimum 10day course – consider taper) – avoid in CHF, CRF, Hx GI bleed, HTN
- Oral Prednisone/Prednisolone– (minimum 10days course with taper)
-
- Intra-articular Methylprednisolone – only for pts with crystals on joint aspiration and considered at extremely low likelihood for septic arthritis who have good follow up, or oral medication failure
- Colchicine – low dose colchicine, 1.2mg followed by 0.6mg at one hour for patients who present within 12hrs of symptom onset was shown to be effective in the the AGREE trial which provides a reasonable ‘pill in the pocket’ abortive strategy for their next gouty attack (beware in patients with renal or liver impairment)
- Do not interrupt the use of Allopurinol or diuretics in patients who come to ED on allopurinol or diuretics unless they have just very recently been started on it, as stopping allopurinol may cause fluctuations in uric acid levels that worsen gout.
Other Causes of Acute Monoarthritis
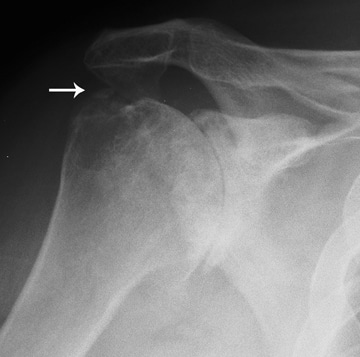
- Pseudogout (CPPD crystal disease): classically, elderly woman with ‘hot joint’ that is often precipitated by trauma, and often not particularly red, with findings of chondrocalcinosis on X-ray (See image below)


- Acute Calcific Periarthritis/Arthritis of Hydroxyapatite Disease: profound periarticular inflammation with ‘fluffy infiltrates’ on X-ray (see image below)
APPROACH TO ACUTE POLYARTHRITIS
- First, rule out septic arthritis and gout as they can both be polyarticular (which carries a worse prognosis)
- Next, identify patients who are systemically unwell and/or have non-MSK organ involvement as they require further work-up and usually an admission.
- Consider routine blood work plus urine dip for protein, creatinine and CXR for patients who are systemically unwell or you suspect might have non-MSK
- Seronegative Arthritis: Reactive arthritis (most common in ED), Psoriatic Arthritis, Ankylosing Spondylitis, IBD Arthritis (suspect seronegative arthritis in patients with oligoarthritis, axial joint involvement, enthesitis and skin changes)
- Enthesitis: inflammation where tendons or ligaments insert into bone that is often present in the seronegative arthropathies (classically Achilles tendon enthesitis)
- Reactive Arthritis: ‘Reiter’s syndrome’ an acute arthritis caused by a preceding GU (eg: Chlamydia) or GI bacteria (eg: Camplylobacter) and recently C. difficile with the classic triad of urethritis, conunctivitis and arthritis (although majority will not have classic triad). Other clinical clues are Enthesitis and axial joint involvement.
- Sarcoidosis: systemic disease that can affect any organ but commonly occurs in young pt with lower extremity mono or oligo acute arthritis with tender papular rash on the shins – erythema nodosum (see image below). Look for nodular granulomas on CXR.

For more on arthritis on EM Cases:
Best Case Ever 5 Septic Arthritis
Dr. Japhe and Dr. Helman have no conflicts of interest to declare.
Key References
Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oral colchicine for early acute gout flare: Twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum. 2010;62(4):1060-8. www.ncbi.nlm.nih.gov/pubmed/20131255
Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis?. JAMA. 2007;297(13):1478-88. www.ncbi.nlm.nih.gov/pubmed/17405973
Janssens HJ, Fransen J, Van de lisdonk EH, Van riel PL, Van weel C, Janssen M. A diagnostic rule for acute gouty arthritis in primary care without joint fluid analysis. Arch Intern Med. 2010;170(13):1120-6.
Full Article: http://archinte.jamanetwork.com/article.aspx?articleid=225738
Now test your knowledge with a quiz.



Leave A Comment