

In the first part of this epic 2 part must-hear episode, Transfusions, Anticoagulants & Bleeding, we have the triumphant return of Dr. Walter Himmel (also known as ‘The walking encyclopedia of EM’) along with Dr. Katerina Pavenski (Head of Transfusion Medicine at St. Michael’s Hospital) & Dr. Jeannie Callum (Head of Transfusion Medicine at Sunnybrook Hospital) who will update you on the latest in transfusion indications & risks, managing INRs and how Wararin compares to Dabigatran, Rivaroxiban & Apixaban. They give you the authoritative low down on: Indications for red cell transfusions in different clinical scenarios (GI bleed, cardiac disease, vaginal bleeding etc) and how to give them, Risks of red cell transfusions including Host vs Graft Disease, TRALI & TACO and how to manage them, IV Iron as an alternative to red cell transfusions, Managing INRs: indications for Vit K, Prothrombin Complex Concentrates (Octaplex & Beriplex), adjusting Warfarin Dose, liver patients, and much much more………
Podcast: Play in new window | Download (Duration: 1:28:18 — 80.9MB)
Subscribe: Apple Podcasts
Written Summary by Claire Heslop, edited by Anton Helman September, 2013
Cite this podcast as: Himmel, W, Pavenski, K, Callum, J, Helman, A. Transfusions, Anticoagulants and Bleeding. Emergency Medicine Cases. September, 2013. https://emergencymedicinecases.com/episode-36-transfusions-anticoagulants-bleeding-part-1/. Accessed [date].
Go to part 2 of this 2-part podcast on transfusions, anticoagulants, and bleeding
When to Group & Screen and Cross Match
Group & Screen Order if there is any chance that the patient may require blood
- Group: ABO and Rh Status
- Screen: Screens patient’s blood for antibodies to other antigens
Cross Match Order cross match if there is a1 in10 chance of giving blood, and ask the lab to put the blood on hold. Uncrossmatched Blood Order if you need stat blood. Call the lab and communicate that you need unmatched O- or O+ blood stat.
- O+: males or females > 45 yo
- O-: females of child bearing age, or known Rh- patient.
- O- blood prevents alloimmunization that could affect future pregnancies.
Indications for Transfusion in General Factors to consider:
- Is there active bleeding?
- If active bleeding, how brisk is the bleeding?
- Age
- Comorbidities (i.e. CAD)
- Symptoms
- Hb level
Red Blood Cell Transfusions
How to Give RBCs
- In non-urgent, non-bleeding patients, transfuse 1 unit at a time, repeat exam to reassess the need for further units.
- Duration of transfusion: slowly, up to 4 hours per transfusion.
- Furosemide to prevent TACO: To prevent transfusion associated circulatory overload (TACO) consider IV furosemide prior to the start of transfusion in patients at high risk for TACO (see below). For patients at lower risk for TACO, po furosemide may be adequate.
Counseling Patients on the Risks of Transfusion Emphasize the risk of fever, TACO (1/700), transfusion related acute lung injury (TRALI, 1/10,000), acute hemolytic transfusion reaction (1/40,000), sepsis (bacterial infection, 1/250,000 for RBCs), allergic reactions. De-emphasize viral infections, which are much more rare: Hep B/C (1 in 2 million), HTLV (1 in 4 million), HIV (1 in 8 million). TACO Risk Factors
- Age > 70
- History of CHF
- Renal failure
- Positive fluid balance
Distinguishing TACO from TRALI
- TRALI is non-cardiogenic pulmonary edema, with onset within 6h of transfusion.
- Findings include SOB, hypoxia, diffuse bilateral infiltrates on CXR. Dx clue: TRALI does not respond to furosemide.
- Treatment: stop the transfusion, disconnect tubing, supplemental 02, ventilatory support prn.
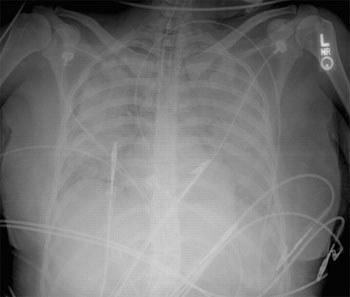
CXR showing diffuse bilateral infiltrates in TRALI
Transfusion Related Graft vs. Host Disease (GVHD) Rare, high mortality. Can damage liver, skin, mucosa, GI tract causing diarrhea. Preventable by using irradiated blood in at-risk immunosuppressed patients (including patients with bone marrow transplant, leukemia/lymphoma, hodgkins, immunodeficiency state, use of certain medications, sickle cell patients). For all immunocompromised patients speak to your transfusion technologist regarding special requirements for blood (i.e. irradiated blood).
For the latest on Infection Risk in Transfusions see Ryan Radecki’s analysis of a JAMA meta-analysis on the subject from May 2014.
Transfusing GI Bleeds
Stable patients with a chronic GI bleed of small volume can tolerate low hemoglobins. Upper GI bleeds are associated with worse outcomes when transfused liberally (see below – increased bleeding, higher mortality, increased length of stay). NJEM (2013) Study: patients with upper GI bleeds randomized to a restricted transfusion group (transfused for Hb < 70, goal 70-90) had better outcomes (lower mortality, less bleeding, less cardiac events, decreased need for surgery) versus the liberally transfusion group (transfused for Hb <90, goal 90-110). Note: this study was in a highly controlled environment with rapid access to GI scopes, therefore, may not applicable to all clinical settings.
Indications for Red Cell Transfusion in CAD
American Association of Blood Bank (2012) recommends transfusion in CAD patients with Hb < 80 and symptomatic. Our experts recommend maintaining NSTEMI patients with a Hb > 80, STEMI patients with a Hb >90 and possibly higher.
![]() Update 2021: A randomized controlled trial aiming to determine the optimal transfusion strategy in patients with acute MI and anemia (Hgb between 7-10 g/dL) demonstrated that a restrictive transfusion strategy was non-inferior to a liberal transfusion strategy, when comparing the frequency of MACE after 30 days. Abstract
Update 2021: A randomized controlled trial aiming to determine the optimal transfusion strategy in patients with acute MI and anemia (Hgb between 7-10 g/dL) demonstrated that a restrictive transfusion strategy was non-inferior to a liberal transfusion strategy, when comparing the frequency of MACE after 30 days. Abstract
![]() Update 2023: A randomized control trial including 3,504 patients with myocardial infarction and anemia (hemoglobin level of less than 10g/dL) found that a liberal transfusion strategy (hemoglobin cutoff <10g/dL) compared to a restrictive strategy (hemoglobin cutoff 7 or 8g/dL) was not associated with decreased composite outcome of myocardial infarction or death at 30 days (14.5% vs 16.9%, risk ratio 1.15, 95% CI 0.99 to 1.34, P = 0.07). Abstract
Update 2023: A randomized control trial including 3,504 patients with myocardial infarction and anemia (hemoglobin level of less than 10g/dL) found that a liberal transfusion strategy (hemoglobin cutoff <10g/dL) compared to a restrictive strategy (hemoglobin cutoff 7 or 8g/dL) was not associated with decreased composite outcome of myocardial infarction or death at 30 days (14.5% vs 16.9%, risk ratio 1.15, 95% CI 0.99 to 1.34, P = 0.07). Abstract
MANAGING INR
In patients with an INR that is supratherapeutic and are on warfarin, consider the following factors prior to adjusting dose:
- Why does the patient have a supratherapeutic INR? Diet changes, illness/infection, medication/herb interactions (antibiotics, antifungals, amiodarone, st. johns wort, ginseng, etc.)
- Is there any evidence of active bleed?
- What is the patient’s risk of traumatic bleed? (e.g. is the patient prone to falls)
- Is the patient at high risk for thrombosis if INR reduced to subtherapeutic level? (mechanical valve, previous stroke with subtherapeutic INR, previous venous or arterial thrombosis)
Risk of Bleeding on Warfarin
Chronic anticoagulation is associated with 1-3% rate of major bleeds (ICH, GI bleed, spinal epidural hematoma, retroperitoneal hematoma, compartment symptoms), and a 6-10% rate of minor bleeds.
- No bleeding, INR < 10
- No INR reversal
- Warfarin dose adjustment (see below)
- No bleeding, INR > 10
- PO vitamin K (1-2mg)
![]() Update 2020: A retrospective cohort study involving 809 patients demonstrated that Vitamin K administration does not improve clinical outcomes in non-bleeding patients with an INR above 10, and patients may be treated with warfarin interruption alone. Abstract
Update 2020: A retrospective cohort study involving 809 patients demonstrated that Vitamin K administration does not improve clinical outcomes in non-bleeding patients with an INR above 10, and patients may be treated with warfarin interruption alone. Abstract
Guidelines for Warfarin Adjustment (based on the RELY Trial)
Calculate dose on weekly basis
With a change in warfarin dose, it takes 48 hours for the INR to reflect the dose.
- INR 1.5 – increase by 15%
- INR 1.5-2 – increase by 10%
- INR 3-4 – decrease by 10%
- INR 4-5 – hold 1 day or decrease by 10%
- INR 5-9 hold until INR is 2-3 or decrease by 15%
- INR > 9 consider 1-2 mg po vitamin K
Minor Bleeding INR Management Options (e.g. gums/epistaxis/dental):
1) Reverse INR to therapeutic level.
- Avoid reversing the INR to a subtherapeutic level so that prevention of thrombosis is maintained. Give small dose of oral vitamin K (e.g.1 mg po vitamin K).
2) No reversal of INR (i.e. continue same warfarin dose) and consider Tranexamic Acid (see Episode 38: ENT Emergencies Pearls & Pitfalls, Tips & Tricks)
Managing elevated INR in liver disease
Remember elevated INR secondary to liver disease is treated differently than elevated INR secondary to vitamin K antagonists. Classic teaching is that a bleeding patient with INR >1.5 requires plasma. However, our experts advise caution against this, except in massively bleeding patients.
Reversing INR in Preparation for OR in Non-bleeding Patients
IV Vitamin K usually required as PO Vitamin K will take 1-2 days to work.
![]() For more on Transfusions, Anticoagulants and Bleeding on EM Cases:
For more on Transfusions, Anticoagulants and Bleeding on EM Cases:
Episode 37: Anticoagulants, PCCs and Platelets
Episode 88 – DOACs Part 1: Use and Misuse
Episode 89 – DOACs Part 2: Bleeding and Reversal Agents
Best Case Ever 18: Anticoagulant Reversal in Trauma
Best Case Ever 51 – Anticoagulants and GI Bleed with Walter Himmel
Dr. Helman, Dr. Himmel, Dr. Pavenski and Dr. Callum have no conflicts of interest to declare.
References
AABB Guidelines. Ann Int Med. 2012;157:49-58. www.aabb.org/pressroom/pressreleases/Pages/pr120…
Hebert et al. TRICC Study. NJEM. 1999;340:1056. www.nejm.org/doi/full/10.1056/NEJM19990211340060…
Villaneuva et al. NJEM. 2013; 368(1):11-21. www.nejm.org/doi/full/10.1056/NEJMc1301256
Additional FOAMed Resources
Bloody Easy 3 – Blood Transfusions, Blood Alternatives & Transfusion Reactions: A Guide to Transfusion Medicine. 3rd edition. 2008. Ontario Regional Blood Coordinating Network. Full PDF
Now test your knowledge with a quiz.



[…] here for an in depth discussion with Walter Himmel, Katerina Pavenski & Jeannie Callum on […]
Thanks for this amazing podcast.