

For such a large organ, EM physicians spend proportionally little time thinking about the liver. Sure, we’re often in the neighborhood (whether it be doing a FAST or diagnosing biliary disease), but the liver really doesn’t get the credit it’s due. Nonetheless, from time to time, whether it be the acute liver failure patient gushing from a varix whose INR is greater than his shoe size, or the confused hepatic encephalopathy patient levitating off the bed using nothing but asterixis, there are definitely times where the middle child of the abdomen steals the show.
In this podcast on liver emergencies and acute liver failure with Dr.Walter Himmel and Dr.Brian Steinhart, we answer questions such as: What are the most important causes of acute liver failure that we need to identify in the ED so we can initiate timely treatment? What are some of the common medications we use in the ED that we should avoid in the liver patient? How should we approach the interpretation of liver enzymes and liver function tests? What are the key management steps in treating acute liver and hepatorenal syndrome? Why do liver failure patients become hypoglycemic and how should hypoglycemia in these patients be treated in the ED? How do we diagnose hepatorenal syndrome in the ED? How can the MELD score help us manage liver patients? What are the indications for IV albumin? What is the role of an ammonia level in the diagnosis of hepatic encephalopathy? Is polyethylene glycol a better alternative to lactulose for treating hepatic encephalopathy? and much more…
Podcast: Play in new window | Download (Duration: 1:11:35 — 65.5MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman. Voice editing by Raymond Cho.
Written Summary and blog post by Jennifer He and Anton Helman, November, 2020
Cite this podcast as: Helman, A. Himmel, W. Steinhart, B. Episode 148 Liver Emergencies: Acute Liver Failure, Hepatic Encephalopathy, Hepatorenal Syndrome, Liver Test Interpretation & Drugs to Avoid. Emergency Medicine Cases. November, 2020. https://emergencymedicinecases.com/liver-emergencies-acute-liver-failure-hepatic-encephalopathy-hepatorenal-syndrome-liver-test-interpretation. Accessed [date]
Acute Liver Failure
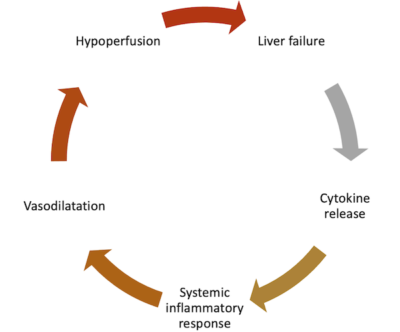
Patients with acute liver failure in the ED may progress to multiorgan failure unless treatment is initiated early. The cytokine release in liver failure and necrosis kicks off a systemic inflammatory response, causing vasodilation and hypoperfusion.
Patients with liver cirrhosis have an increased susceptibility to bacterial infections due to a compromised immune system, portal hypertension due increased portal venous flow and hepatic resistance, thrombosis due to complex alterations in the coagulation factors and hypoalbuminemia, and bleeding due to portal hypertension as well as complex alterations in the coagulation factors . Liver patients may have decreased gluconeogenesis (leading to hypoglycemia), decreased lactate clearance (leading to metabolic acidosis) and decreased ammonia clearance (leading to hyperammonemia). All of these need to be considered in the ED management of patients with acute liver failure.
Triggers for decompensation in patients with liver disease: Search carefully for infections
Infections are a common high risk trigger for acute liver failure in patients with chronic liver disease and may present in a subtle manner, similar to the immunocompromised patient. It is therefore incumbent upon the emergency physician to conduct a thorough search for underlying infection in the sick liver patient. Pneumonia, ARDS and sepsis are the most common diagnoses of ESLD patients admitted to ICU. These patients are also at high risk for urinary tract infections, C. Diff and spontaneous bacterial peritonitis. Have a low threshold to treat for sepsis on speculation.
Other common triggers include ongoing alcohol use, acetaminophen overdose, adverse drug effects, trauma, GI bleed and electrolyte disturbances. Common vague triggers include constipation (decreased gut transit time increases ammonia levels) and malnutrition.
Causes of acute liver failure in the absence of known liver disease
Hepatic ischemia from any shock state (“shock liver”) is a common cause of acute liver failure in the ED where treatment is aimed at the underlying cause of shock.
Common disease states that cause fulminant acute liver failure that should be considered in the ED:
- Acetaminophen toxicity
- Drug induced liver injury
- Viral hepatic diseases
- Autoimmune diseases
- Mushroom toxicity
- Wilson’s disease
Pearl: As recommended by The Association for the Study of Liver Diseases, draw an acetaminophen level on all patients with acute liver failure (recognizing that a “therapeutic” level does not rule out acetaminophen toxicity) and have low threshold for starting NAC in those suspected of acetaminophen toxicity
Misconception: a common misconception is that patients with acute liver failure will be jaundiced. Jaundice may not be present despite severe decompensated acute liver failure.
Treatment of Acute Liver Failure in the ED
Hypoperfusion/vasodilatation – our experts recommend blood products for the bleeding patient in shock, fluid resuscitation with normal saline for the non-bleeding liver failure patient, and to consider IV albumin in patients with hepatorenal syndrome, hepatic encephalopathy and low albumin, post-paracentesis >5L and bacterial peritonitis.
Bacterial infections – have a low threshold for initiating antibiotics in patients with acute liver failure suspected of infection as a trigger.
Hypoglycemia – a common pitfall in managing acute liver failure patients in the ED is the inadequate treatment of hypoglycemia. Maintaining normal glucose levels can help prevent starvation ketosis, ketoacidosis and lactic acidosis. One bolus of 50% dextrose may not be adequate therapy because of depleted glycogen stores; maintenance infusions of D10W or D25W should be administered after the D50W bolus.
Hyperammonemia – ammonia levels are unreliable and may be misleading; patients with acute liver failure and hepatic encephalopathy should be presumed to have elevated ammonia levels and be treated with lactulose and/or PEG and rifaximin accordingly
Demystifying Liver Enzymes and Liver Function Tests in Liver Emergencies
Liver enzymes (AST, ALT, ALP, GGT) and liver function tests – LFTs (INR, PTT, albumin, bilirubin) are terms that are often mistakenly used interchangeably. Simply put, the main difference between liver enzymes and LFTs is that the former are a measure of the degree of cell death/damage to the liver, whereas the latter involves the synthetic capability of liver – liver metabolism.
Liver enzymes
Insults to hepatocytes lead to necrosis and cause elevated transaminases. ALT is most specific for liver disease. ALP is found in bone and liver and is usually elevated in obstructive biliary disease. An elevated GGT that is proportional to an elevated ALP can help distinguish liver disease from bone disease.
The degree of elevation of liver enzymes can help guide the differential diagnosis:
- Mild elevation: up to 5 x of normal – fatty liver, end-stage liver cirrhosis, infiltrative liver disease
- Moderate elevation: 5-10 x of normal – alcohol related liver disease, chronic hepatocellular and cholestatic disease
- Severe elevation: >15 x of normal – acute liver failure including viral hepatitis, acetaminophen toxicity, shock liver, HELLP
The commonly known ratio of 2:1 AST:ALT is suggestive of alcoholic liver disease, with the caveat that other conditions such as NASH, hepatitis C and rhabdomyolysis may have a similar liver enzyme ratio.
Pearl: in cholestasis, the first enzyme to increase is often ALT, which occurs prior to the elevation of ALP.
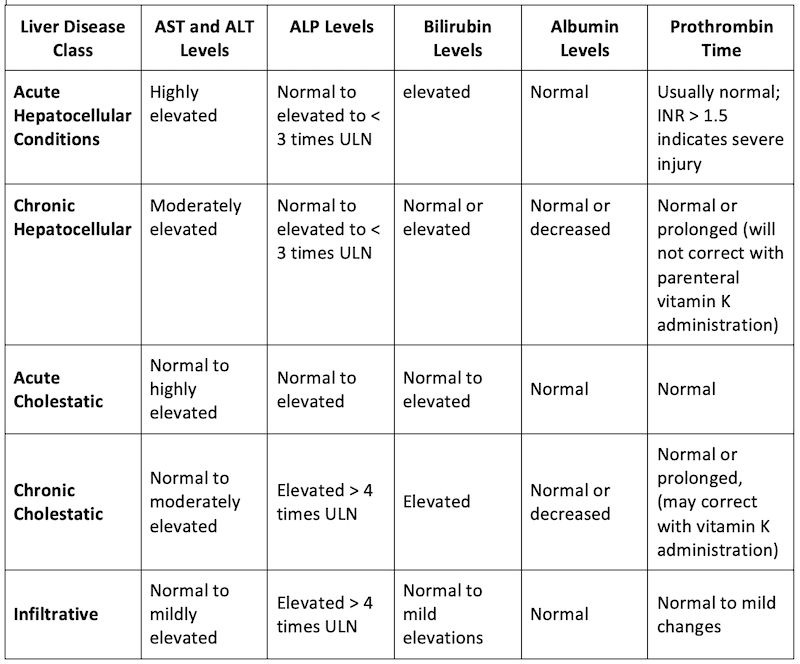
Adapted from: Woreta TA, Alqahtani SA. Evaluation of abnormal liver tests. Med Clin North Am. 2014;98(1):1-16.
LFTs
Albumin – hypoalbuminemia is found not only in patients with liver disease, but also in those with nephrotic syndrome, protein losing enteropathy, heart failure and malnutrition.
INR – while the INR is elevated in many patients with liver disease and may help to predict prognosis, a liver patient with an elevated INR is not necessarily at increased risk for bleeding, and an elevated INR in a liver patient does not rule out the possibility of thrombosis
Bilirubin – serum conjugated bilirubin level does not become elevated until the liver has lost 50% of its excretory capacity; while an elevated bilirubin may suggest poor liver function it cannot distinguish between hepatocellular, cholestatic, or infiltrative liver disease and may be normal or elevated in each
MELD score stratifies severity of end-stage liver disease for transplant planning and includes Creatinine, INR, bilirubin, sodium and renal replacement therapy. It has poor sensitivity, but its constituents are useful in the ED to get a general sense of severity of disease.
ED Medications to Adjust or Avoid in Liver Patients and Liver Emergencies
Susceptibility to adverse effects from medications increases with worsening liver function. In general, try to avoid sedative drugs (benzodiazepines, opioids, antihistamines, antiemetics) in patients with severe liver disease.
Opioids
No opioid is ideal in the liver patient. Morphine has toxic metabolites that may accumulate in liver patients; hydromorphone has impaired elimination. If opioids are required, our experts recommend IV fentanyl in the ED and oral hydromorphone at lower doses with longer time in between doses (e.g. hydromorpohone 0.5mg po q8h) after discharge. Consider IV ketamine as an alternative to opioids for analgesia in the liver patient in the ED.
Acetaminophen
A common misperception is that acetaminophen is strictly contraindicated in all liver patients. In those with mild liver disease, it is generally safe to prescribe acetaminophen at a lower dose (500mg q6h, max 2g daily). Acetaminophen should be avoided in patients with severe liver disease and those with active alcohol use.
NSAIDs
- NSAIDs can cause renal impairment and even lead to hepatorenal syndrome in liver patients in addition to triggering GI bleeding
- NSAIDs should be avoided in patients with cirrhosis and in patients with acute liver failure, but can be considered in low doses/short courses in patients with mild liver disease
Benzodiazepines
Benzodiazepines should generally be avoided in patients with severe liver disease and dosages should be lowered in those with mild liver disease. Patients with even mild hepatic encephalopathy are very sensitive to GABAergic medications. The exception, of course, is alcohol withdrawal. Lorazepam is the benzodiazepine of choice for alcohol withdrawal in patients with severe liver disease – see Episode 87 Alcohol Withdrawal & Delirium Tremens for details.
Antiepileptic medications
Carbamazepine and valproate are contraindicated in patients with severe liver disease and phenytoin should be used with caution. Expert opinion dictates that if ALT values exceeding 5x the upper limit of normal (or lesser elevations associated with any rise in bilirubin or any associated symptoms of hepatitis), phenytoin should be discontinued. The antiepileptic medication of choice in patients with liver disease is levetiracetam.
Antiemetics
Sedating antiemetics should should be avoided in patients with severe liver disease. Metoclopramide and ondansetron require significant dose reduction in patients with cirrhosis.
Antibiotics
While most antibiotics are safe in liver patients, macrolides, ciprofloxacin, nitrofurantoin, trimethoprim-sulfamethoxazole should be avoided in liver patients, and amoxicillin/clavulanic acid can cause liver failure even when taken at therapeutic doses.
Cardiac medications
Medications such as beta-blockers, diltiazem and amiodarone are metabolized through first-pass metabolism. If starting these medications, start low, go slow.
Pearl: if prescribing a drug that may be constipating, consider starting a laxative empirically to decrease transit time in the GI tract and minimizing the risk of hepatic encephalopathy
Antibiotics to avoid in liver patients
- Patients with hepatic encephalopathy have excess GABA stimulation, so they are very sensitive to GABAergic medications (e.g. benzodiazepines or barbiturates).
- Administration of benzodiazepines or barbiturates to a patient with hepatic encephalopathy risks inducing a prolonged stuporous/comatose state.
Hepatic Encephalopathy: A Diagnosis of Exclusion
Step 1: Rule out other causes of altered level of awareness (LOA) including sepsis, renal failure, alcohol withdrawal and subdural hematoma.
Step 2: Assess for and address common precipitants of hepatic encephalopathy which include:
- Medications – noncompliance/use of diuretics/benzodiazepines
- GI bleeding
- Hypokalemia
- Alkalosis
- Volume depletion
- Sepsis
Step 3: Make the diagnosis
- After excluding other causes of altered LOA look for asterixis (nonspecific – also seen in renal failure) and signs of cirrhosis
- Diurnal sleep pattern reversal may help support a diagnosis of hepatic encephalopathy
- In general, the more altered the patient is, the more severe the disease
Step 4: Correct presumed hyperammonemia (without the need for a serum ammonia level)
- Lactulose 20 g (30mL) po, titrated to 3 to 4 soft stools per day (reduces mortality, serious complications)
- If patient is NPO, Polyethylene glycol (PEG) via NG tube 4L over 4 hours (more rapid resolution of hepatic encephalopathy compared to lactulose in 2 small RCTs) or lactulose enema with 1–3 L of 20% solution
Step 5: Replace fluid and glucose deficits
- NS is our experts’ crystalloid of choice for fluid replacement in hepatic encephalopathy
- Consider albumin in patients with low serum albumin given some weak RCT evidence that it may improve outcomes in hepatic encephalopathy
- One bolus of 50% dextrose may not be adequate therapy for hypoglycemia because of depleted glycogen stores; maintenance infusions of D10W or D25W should be administered after the D50W bolus
Step 6: Treat even the mildest hypokalemia
- Hypokalemia contributes to hyperammonemia by decreasing ammonia excretion; correcting hypokalemia is thought to decrease ammonia levels in patients with hepatic encephalopathy
Step 7: Assess for and treat cerebral edema
- Cerebral edema is the most common cause of death in patients with hepatic encephalopathy due to the rapid accumulation of ammonia
- Cerebral edema may be clinically subtle; if suspected, keep the head of the bed elevated at 45 degrees and consider hypertonic saline (20 ml of 30% NaCl targeting a serum Na level between 145-150 mmol/L)
Step 8: Consider refaximin
- Rifaximin 400-550 mg po daily – this antibiotic is not absorbed through the gut, eradicates E. Coli which produces ammonia, and is used for long term maintenance of patients with recurrent hepatic encephalopathy
Pearl: Diurnal Sleep Pattern Reversal: Could it be Hepatic Encephalopathy? This can present with a patient who may be up all night and sleeping during the day. It is not 100% sensitive or specific for the diagnosis but may help support a diagnosis of hepatic encephalopathy.
The myth of ammonia
The #1 recommendation by Choosing Wisely Canada – Hepatology is “d
Pitfall: a common pitfall is ruling out hepatic encphalopathy with a normal ammonia level; ammonia levels can be normal or near-normal in hepatic encephalopathy; as such they can be misleading
Pearl: a trick to eliciting asterixis in a patient who is unable to follow commands involves placing their forearm on the stretcher and forcibly dorsiflexing the wrist to bring out asterixis
Hepatorenal Syndrome: Another Diagnosis of Exclusion
Hepatorenal Syndrome carries a mortality rate of >50% in the absence of liver transplant. It is a diagnosis of exclusion.
It is difficult to diagnose Hepatorenal Syndrome in the ED because the diagnostic criteria include:
- Cirrhosis with ascites
- Creatinine > 132 umol/L
- No improvement in serum Creatinine after 2 days of diuretic withdrawal and albumin volume expansion
- Absence of shock
- Absence of nephrotoxic medications
- No parenchymal renal disease (no proteinuria > 500 mg/day, microhematuria, or renal US abnormality)
Patients typically have decreased urine output, elevated creatinine, low urine sodium, and no/little urine sediment/protein (“bland urine”), and no improvement in renal function with correction of hypovolemia.
Many liver patients are on diuretics which may alter sodium excretion. While low urine sodium is typical in hepatorenal syndrome, it can only be interpreted accurately after several days of discontinuation of diuretics, long after the patient has left the ED.
Clinical clue: suspect Hepatorenal Syndrome in a patient with liver disease in whom volume status does not improve with fluids or albumin
Beware: the excessive use of diuresis, underuse of albumin and underperformance of paracentesis increase the risk of Hepatorenal Syndrome
ED Management of Hepatorenal Syndrome
- This is a complex disease – get help from your ICU and GI colleagues
- Avoid give diuretics and benzodiazepines
- Replace low serum albumin with IV albumin 1.5 g/kg
- Manage hypotension aggressively as these patients are significantly vasodilated; consider norepinephrine
- Discuss giving octreotide and/or midodrine with admitting physician
- Consider if patient is a liver transplant candidate based on the MELD score
Take home points for Liver Emergencies: Acute Liver Failure, Hepatic Encephalopathy, Hepatorenal Syndrome, Liver Test Interpretation & Drugs to Avoid
- Have a low threshold to order acetaminophen levels in the sick liver patient
- Sepsis is a common trigger of acute liver failure and may be subtle – when in doubt, treat on speculation
- ED medications requiring dose adjustment or avoidance in the liver patient: NSAIDs, opioids, acetaminophen, benzodiazepines, antiepileptics (except levetiracetam), macrolides, B-blockers, amiodarone
- Watch out for hypoglycemia in sick liver patients and start an infusion of D10W after you have corrected the hypoglycemia
- Serum ammonia levels are unreliable and can be misleading; assume high ammonia levels in the patient suspected of hepatic encephalopathy and treat with lactulose and/or polyethylene glycol and rifaximin
- IV albumin needs to be considered in the patient with acute liver failure, hepatorenal syndrome and hepatic encephalopathy
- Have a low threshold to treat for hepatic encephalopathy and hepatorenal syndrome on speculation as they are both diagnoses of exclusion
- Some patients with hepatic encephalopathy will develop cerebral edema and this may be subtle; keep the head of bed at 45 degrees and give hypertonic saline if there are any clinical signs of cerebral edema
For part 2 of this series on Liver Emergencies go to Episode 149 Liver Emergencies: Thrombosis and Bleeding, Portal Vein Thrombosis, SBP, Paracentesis Tips and Tricks
References
- Montrief T, Koyfman A, Long B. Acute liver failure: A review for emergency physicians. Am J Emerg Med. 2019;37(2):329-337.
- Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369(26):2525-34.
- Lee WM, Stravitz RT, Larson AM. Introduction to the revised American Association for the Study of Liver Diseases Position Paper on acute liver failure 2011. Hepatology. 2012;55(3):965-7.
- Lee WM, Stravitz RT, Larson AM. Introduction to the revised American Association for the Study of Liver Diseases Position Paper on acute liver failure 2011. Hepatology. 2012;55(3):965-7.
- Montrief T, Koyfman A, Long B. Acute liver failure: A review for emergency physicians. Am J Emerg Med. 2019;37(2):329-337.
- Lewis JH, Stine JG. Review article: prescribing medications in patients with cirrhosis – a practical guide. Aliment Pharmacol Ther. 2013;37(12):1132-56.
- Lewis JH. The rational use of potentially hepatotoxic medications in patients with underlying liver disease. Expert Opin Drug Saf. 2002;1(2):159-72.
- Lewis JH, Stine JG. Review article: prescribing medications in patients with cirrhosis – a practical guide. Aliment Pharmacol Ther. 2013;37(12):1132-56.
- Mazoit JX, Sandouk P, Zetlaoui P, Scherrmann JM. Pharmacokinetics of unchanged morphine in normal and cirrhotic subjects. Anesth Analg. 1987;66(4):293-8.
- Soleimanpour H, Safari S, Shahsavari nia K, Sanaie S, Alavian SM. Opioid Drugs in Patients With Liver Disease: A Systematic Review. Hepat Mon. 2016;16(4):e32636.
- Chandok N, Watt KD. Pain management in the cirrhotic patient: the clinical challenge. Mayo Clin Proc. 2010;85(5):451-8.
- Woreta TA, Alqahtani SA. Evaluation of abnormal liver tests. Med Clin North Am. 2014;98(1):1-16.
- Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ. 2005;172(3):367-79.
- Woreta TA, Alqahtani SA. Evaluation of abnormal liver tests. Med Clin North Am. 2014;98(1):1-16.
- Shakil AO, Kramer D, Mazariegos GV, Fung JJ, Rakela J. Acute liver failure: clinical features, outcome analysis, and applicability of prognostic criteria. Liver Transpl. 2000;6(2):163-9.
- Fouad YM, Yehia R. Hepato-cardiac disorders. World J Hepatol. 2014;6(1):41-54.
- Montrief T, Koyfman A, Long B. Acute liver failure: A review for emergency physicians. Am J Emerg Med. 2019;37(2):329-337.
- Lockwood AH. Blood ammonia levels and hepatic encephalopathy. Metab Brain Dis. 2004 Dec;19(3-4):345-9.
- Vilstrup H, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014 Aug;60(2):715-35.
- Nassar Junior AP, Farias AQ, D’ Albuquerque LA, et al. Terlipressin versus norepinephrine in the treatment of hepatorenal syndrome: a systematic review and meta-analysis. PLoS One 2014;9(9):e107466.
- Salerno F, Navickis RJ, Wilkes MM. Albumin treatment regimen for type 1 hepatorenal syndrome: a dose-response meta-analysis. BMC Gastroenterol 2015;15: 167.
- Bohra A, Worland T, Hui S, Terbah R, Farrell A, Robertson M. Prognostic significance of hepatic encephalopathy in patients with cirrhosis treated with current standards of care. World J Gastroenterol. 2020;26(18):2221-2231.
- Gluud LL, Vilstrup H, Morgan MY. Non-absorbable disaccharides versus placebo/no intervention and lactulose versus lactitol for the prevention and treatment of hepatic encephalopathy in people with cirrhosis. Cochrane Database Syst Rev 2016;(5):CD003044.
- Kimer N, Krag A, Møller S, et al. Systematic review with meta-analysis: the effects of rifaximin in hepatic encephalopathy. Aliment Pharmacol Ther 2014;40(2): 123–32.
- Long B, Koyfman A. The emergency medicine evaluation and management of the patient with cirrhosis. Am J Emerg Med. 2018;36(4):689-698.
- Murphy N, Auzinger G, Bernel W, Wendon J. The effect of hypertonic sodium chloride on intracranial pressure in patients with acute liver failure. Hepatology. 2004;39(2):464-70.
- Sharma BC, Singh J, Srivastava S, et al. Randomized controlled trial comparing lactulose plus albumin versus lactulose alone for treatment of hepatic encephalopathy. J Gastroenterol Hepatol 2017;32(6):1234–9.
Drs. Helman, Himmel and Steinhart have no conflicts of interest to declare
Now test your knowledge with a quiz.



Excellent podcast on a topic that needed exposure. Great job.
Do you recommend empirical NAC for fulminant hepatitis even if no tylenol ingestion at hx/labs?