
Sleep is wonderful. And it’s essential to life. The better we sleep the better we concentrate, make decisions and perform. Sleep minimizes the chance of making errors on shift. Better sleep makes us learn better – it plays a key role in consolidating both declarative and procedural memory. Better sleep means better adaptive capacity to stressful situations, which are plentiful in EM. The better we sleep the better mood we’re in and the better our relationships. The better we sleep the lower our chance of developing cancer, heart disease, depression, and the longer we live –more sleep is associated a decreased mortality rate! So, the better we sleep the happier and healthier we are. In this main episode EM Cases podcast with sleep expert Dr. Michael Mak, we answer questions such as: When and how should melatonin or other sleep aids be used in shift work, and when should they be avoided? How long before bedtime should you avoid caffeine, alcohol, exercise, and heavy meals to optimize sleep? How do light intensity and color temperature (Kelvin) affect melatonin release and sleep onset? How can you use light strategically before, during, and after a night shift to improve performance and recovery? What’s the best way to get back to sleep if you wake up in the middle of the night and can’t fall asleep? What is the ideal nap length before a night shift to boost alertness without worsening grogginess? What are the most effective shift scheduling strategies to optimize sleep hygiene? and many more…
Podcast: Play in new window | Download (Duration: 1:21:04 — 74.3MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Anton Helman, September, 2025
Cite this podcast as: Helman, A. Mak, M. Episode 207 Sleep Strategies for Shift Work. Emergency Medicine Cases. September, 2025. https://emergencymedicinecases.com/sleep-strategies-shift-work. Accessed July 22, 2026
Why Sleep Strategies Matter for Shift Work
Sleep is not just rest; it is an active biological process essential for life, health, and performance. Adequate, high-quality sleep sharpens our ability to concentrate, make decisions, and perform complex tasks. For Emergency Physicians, nurses, and paramedics, this translates directly into improved clinical judgment, faster cognitive processing, and fewer errors on shift. Sleep also plays a critical role in consolidating both declarative memory—facts, protocols, and knowledge—and procedural memory—skills, techniques, and motor patterns. Beyond cognition, sleep enhances emotional resilience. Well-rested clinicians are better able to navigate the interpersonal challenges and stressful situations that are common in emergency care. There are also profound long-term benefits: adequate sleep lowers the risk of cardiovascular disease, certain cancers, depression, and even premature death. Conversely, chronic sleep deprivation is associated with increased mortality and diminished quality of life.
Unfortunately, shift work disrupts our circadian rhythm and our homeostatic sleep drive, the twin forces that govern sleep timing and quality. This disruption is far from trivial. In the short term, it increases the likelihood of near-miss events, such as motor vehicle collisions on the drive home from a night shift. Over years, it takes a toll on mental and physical health. The good news: by understanding the physiology of sleep and applying evidence-based strategies, we can mitigate these effects and protect both our performance and our long-term well-being.
Pitfall: Underestimating sleep debt. Even mild cumulative sleep loss impairs vigilance and reaction time to a degree comparable to legal intoxication.
Understanding Sleep Strategies: The Physiology of Sleep – Two Engines
Sleep regulation relies on two interacting processes:
-
Homeostatic Sleep Drive (Process S):
-
Driven by adenosine accumulation during wakefulness.
-
The longer you’re awake, the stronger the drive for sleep.
-
-
Circadian Rhythm (Process C):
-
Controlled by the suprachiasmatic nucleus (SCN) in the hypothalamus.
-
Light—especially blue-spectrum—suppresses melatonin, delaying sleep onset.
-
Darkness permits melatonin release, promoting sleep.
-
Cortisol: Peaks 30–45 min after waking, enhancing alertness. Falls throughout the day to reach its nadir near bedtime.
When these processes are in sync, sleep is restorative, and wakefulness is optimized. Shift work disrupts both, creating mismatches between internal physiology and the external environment.
Duration and Timing of Sleep
Adults typically need seven to nine hours of sleep, though genetics and age influence this range. Those over 65 may require slightly less—about seven to eight hours. The key to circadian stability is a consistent wake time, anchored each day with morning light exposure. This daily cue keeps the internal clock aligned to the external world.
Bedtime should not be forced. Instead, it should coincide with genuine sleepiness—the head-nodding, eyelid-heavy sensation—rather than simply physical fatigue. This distinction matters: going to bed when you are not sleepy can condition the brain to associate the bed with wakefulness, paving the way for insomnia. While the wake time should remain constant, bedtime can and should vary depending on the day’s activities, stressors, and physical exertion.
Preparing for Sleep
The hours before bedtime set the stage for restorative sleep. About three hours before sleep, it is best to avoid strenuous physical activity, which elevates core body temperature and activates the sympathetic nervous system. Similarly, large meals close to bedtime can delay sleep onset and disrupt sleep continuity, in part due to gastrointestinal activity and discomfort.
Caffeine is a well-known antagonist of adenosine. For most people, avoiding caffeine for at least 6 hours before bed minimizes its impact on sleep latency and quality. Slow metabolizers—often identifiable by exaggerated jitteriness or tremor—may need a 12-hour buffer. Daily intake should remain under 400 mg, the equivalent of about four cups of coffee. Timing also matters: caffeine’s peak effect occurs about 45 minutes after ingestion, so it should be consumed strategically to match periods of needed alertness.
Alcohol and cannabis deserve special mention. While alcohol can speed sleep onset by enhancing GABAergic inhibition, its metabolism leads to rebound arousal and fragmented sleep. Cannabis, particularly with chronic nightly use, reduces deep and REM sleep, leading to long-term tolerance and impaired sleep quality. Both should be avoided in the three hours before bedtime.
Light is another powerful sleep regulator. In the evening, bright blue-spectrum light delays melatonin release. Reducing light intensity and shifting toward warm, low-Kelvin light (1,000–2,700 K) supports the natural circadian wind-down. If screens must be used, blue light filters or e-ink readers are preferable.
3 hours before bed – avoid:
-
Vigorous exercise (raises core temp & sympathetic tone)
-
Large meals (delays gastric emptying, may cause reflux)
-
Alcohol or cannabis (initial sedation, but later sleep fragmentation)
-
Bright, blue-spectrum light from screens or overhead lighting
Caffeine:
-
Avoid ≥6 hrs before bed (≥12 hrs if slow metabolizer).
-
Max daily dose: 400 mg (≈4 cups coffee).
-
Time morning caffeine ~1 hr after waking for optimal effect.
Light hygiene:
-
Use warm, low Kelvin (<2700K) lighting in the evening.
-
Minimize screen use; if unavoidable, use blue-light filters or e-ink devices.
Optimizing the Sleep Environment
An optimal sleep environment is cool, dark, and quiet. The target temperature is around 20°C (68°F), which facilitates the natural drop in core body temperature associated with sleep onset. The room should be completely dark; blackout curtains or a comfortable sleep mask such as Manta can achieve this even during daylight hours. Noise should be minimized with earplugs or, if preferred, a white noise machine.
Visible clocks should be removed from view. Checking the time during nocturnal awakenings increases cognitive arousal, promotes clock-watching, and worsens insomnia. If you wake in the night and cannot return to sleep, leave the bed for a dimly lit, non-stimulating environment, and engage in a quiet, boring/non-stimulating activity such as a word search game until sleepiness returns which is when sleep should be attempted again.
Light and Dark Strategies for Optimal Sleep
Light is the most potent external cue for the circadian system. Exposure to bright blue light (≥10,000 lux) for about 30 minutes in the morning with either light emitting glasses or a light emitting screen, advances the sleep phase, making it easier to fall asleep earlier the next night. This strategy can also improve mood, even in those without seasonal affective disorder. Conversely, avoiding bright light in the evening—especially blue-spectrum light—helps maintain timely melatonin release.
For those sleeping after night shifts, light management is critical. Wearing dark sunglasses on the commute home reduces morning light exposure that might otherwise delay daytime sleep onset. Once home, the bedroom should be kept dark until waking.
-
Morning: Bright blue light (≥10,000 lux for 30 min) to advance sleep phase and improve mood.
-
Night: Dim, warm light; avoid bright/blue light ≥3 hrs before sleep.
-
Daytime sleep after night shift: Wear sunglasses on commute; keep bedroom dark.
Shift Scheduling Strategies
Casino shifts—split overnight into two shorter segments (i.e 10pm-4am and 4am-10am)—allow at least some sleep during the natural dark period, preserving “anchor sleep” and reducing circadian disruption.
When casino shifts are not possible, night shifts should be grouped together, ideally two or three in a row, rather than spread across a month. This clusters the circadian disruption into a shorter period, allowing recovery. Forward rotation—progressing from day to evening to night shifts—aligns better with the natural human tendency to delay sleep and wake times, making adaptation easier than backward rotation.
Matching shifts to chronotype can further reduce circadian strain. Morning types may fare better with early shifts, while evening types adapt more easily to nights. Recovery time between shifts is also essential: at least 11 hours between shifts gives the body a chance to recover, reducing fatigue and medical error rates.
-
Casino shifts (e.g., 10p–4a & 4a–10a): Preserve anchor sleep in darkness.
-
Cluster night shifts (max 2–3 in a row) instead of spreading through month.
-
Forward rotation (day → evening → night) easier than backward.
-
Chronotype matching: Assign night shifts to natural night owls.
-
Recovery time: ≥11 hrs between shifts.
Napping for Optimal Performance on Shift
Naps can be a powerful tool, but timing and duration matter. A brief 20-minute nap avoids entry into deep sleep and minimizes grogginess upon waking. A full 90-minute nap allows a complete sleep cycle, avoiding sleep inertia. Naps of 30–60 minutes, however, often interrupt deep sleep and can worsen alertness and mood.
-
20 min nap: Boosts alertness, avoids sleep inertia.
-
90 min nap: Completes full sleep cycle; prevents grogginess.
-
Avoid 30–60 min naps (wakes from deep sleep → worse alertness).
Pre-, On-, and Post-Shift Sleep Strategies
|
Strategies | |
|---|---|---|
| Pre-shift | – Nap 20 or 90 min before night shift (not 30-60mins) – Bright light exposure if starting early – Exercise & caffeine 30–60 min pre-shift |
|
| On shift |
|
|
| Post shift | – Wear sunglasses on commute home – Avoid screens & bright light before bed – Keep bedroom cool, dark, quiet – Consider melatonin 0.3–5 mg 3–4 hrs before desired sleep |
Melatonin: A Hormone of Darkness
Melatonin is not a sedative in the traditional sense. It’s a hormone of darkness—a circadian signal that tells your brain it’s time for sleep. Its role is primarily to shift or reinforce the timing of your internal body clock, rather than to “knock you out.”
When to use:
- For shift work adaptation, melatonin is most effective when taken 3–4 hours before the desired sleep onset (for example, after a night shift, if you want to fall asleep at 9 a.m., take it around 5–6 a.m.).
- Especially useful after a block of night shifts to help re-entrain to a daytime schedule, or when rotating between different shift patterns.
Dosing:
- 0.3–5 mg is recommended.
- Lower doses (0.3–1 mg) can be just as effective for circadian signaling with fewer side effects.
- Higher doses (>5 mg) offer no added benefit for sleep onset or quality, and in some people may paradoxically worsen sleep or shift circadian phase in the wrong direction.
Safety and side effects:
- Generally safe for short-term use with minimal next-day sedation.
- Can cause vivid dreams, headache, or grogginess in some individuals.
- Timing is critical—if taken at the wrong circadian phase, it can shift the clock in the wrong direction.
Other Sleep Aids
Prescription Hypnotics (Z-drugs)
Examples: Zolpidem, Zopiclone
- Mechanism: Enhance GABA activity, promoting sedation.
- Role: Consider only for short-term relief of acute insomnia or when other behavioral strategies fail.
- Risks: Tolerance, dependence, rebound insomnia, and next-day sedation that can impair driving or clinical performance.
- Best avoided for chronic use in shift workers.
Wake-Promoting Agents
Examples: Modafinil, Armodafinil
- Mechanism: Exact action not fully understood, but likely involves dopaminergic and orexinergic pathways to enhance wakefulness.
- Role: For diagnosed shift work sleep disorder (SWSD) in which excessive sleepiness persists despite optimized sleep hygiene and light strategies.
- Evidence: Improves alertness and cognitive performance during night shifts.
- Risks: May cause headache, anxiety, insomnia, hypertension, and in rare cases, severe rash or psychiatric effects.
- Should be prescribed with caution, ideally under sleep medicine specialist supervision.
Cannabinoids (THC, CBD, CBN)
- Evidence: Short-term studies may show reduced sleep latency, but chronic nightly use reduces deep and REM sleep and increases fragmentation.
- Risks: Tolerance, dependency, rebound insomnia, and potential for psychiatric effects including psychosis—even in people without clear predisposition.
- Consensus: Not recommended for shift work–related insomnia except in narrow contexts (e.g., severe chronic pain with/without cancer, after weighing risks).
Over-the-Counter Sleep Aids
Antihistamines (diphenhydramine, doxylamine)
- Cause sedation via H1 blockade.
- Side effects include anticholinergic effects (dry mouth, constipation, urinary retention) and residual grogginess.
- Generally not recommended for ongoing use, especially in older adults.
The TimeShifter App for Shift Workers
The TimeShifter app applies some of the science discussed in this podcast to help shift workers adapt their body clock for optimal performance and alertness. By entering your upcoming shifts, chronotype, and caffeine habits, the app generates a personalized plan for when to seek or avoid light, take strategic naps, consume caffeine, and, if desired, use melatonin.
Key Take Home Points on Sleep Strategies for Shift Work
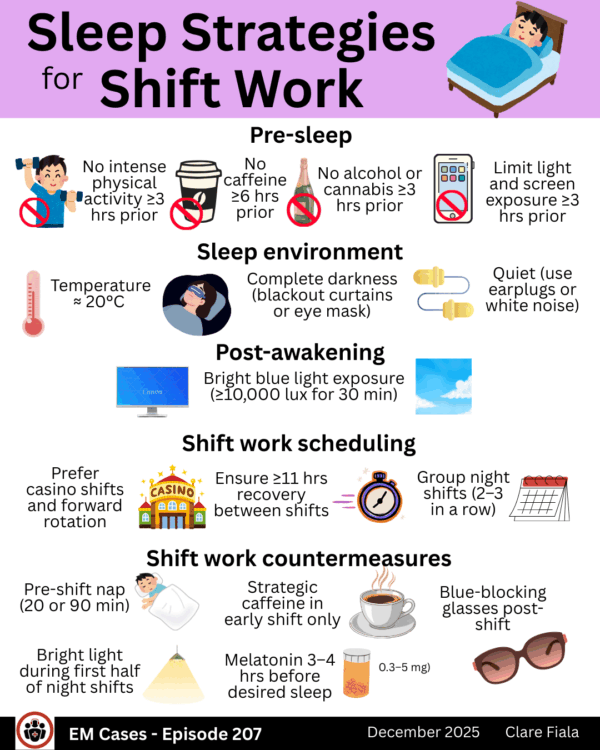
Pre-sleep:
- No caffeine ≥6 hrs prior
- No alcohol or cannabis ≥3 hrs prior
- No intense physical activity ≥3 hrs prior
- Limit light and screen exposure ≥3 hrs prior
Sleep environment:
- Temperature ≈ 20°C (68°F)
- Complete darkness (blackout curtains or eye mask)
- Quiet (use earplugs or white noise)
Post-awakening:
-
Bright blue light exposure (≥10,000 lux for 30 min)
Shift work scheduling:
- Prefer casino shifts and forward rotation
- Group night shifts (2–3 in a row)
- Ensure ≥11 hrs recovery between shifts
- Assign shifts based on chronotype when possible
Shift work countermeasures:
- Pre-shift nap (20 or 90 min)
- Strategic caffeine in early shift only
- Bright light during first half of night shifts
- Blue-blocking glasses post-shift
- Melatonin (0.3–5 mg) 3–4 hrs before desired sleep
References
- Shriane AE, Rigney G, Ferguson SA, Bin YS, Vincent GE. Healthy sleep practices for shift workers: consensus sleep hygiene guidelines using a Delphi methodology. Sleep. 2023 Dec 11;46(12):zsad182.
- Newbury CR, Crowley R, Rastle K, Tamminen J. Sleep deprivation and memory: Meta-analytic reviews of studies on sleep deprivation before and after learning. Psychol Bull. 2021 Nov;147(11):1215-1240.
- Vandekerckhove M, Wang YL. Emotion, emotion regulation and sleep: An intimate relationship. AIMS Neurosci. 2017 Dec 1;5(1):1-17
- Kent RG, Uchino BN, Cribbet MR, Bowen K, Smith TW. Social Relationships and Sleep Quality. Ann Behav Med. 2015 Dec;49(6):912-7
- Institute of Medicine (US) Committee on Sleep Medicine and Research; Colten HR, Altevogt BM, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington (DC): National Academies Press (US); 2006. 3, Extent and Health Consequences of Chronic Sleep Loss and Sleep Disorders. Available from:
- James SM, Honn KA, Gaddameedhi S, Van Dongen HPA. Shift Work: Disrupted Circadian Rhythms and Sleep-Implications for Health and Well-Being. Curr Sleep Med Rep. 2017 Jun;3(2):104-112
- Lee ML, Howard ME, Horrey WJ, Liang Y, Anderson C, Shreeve MS, O’Brien CS, Czeisler CA. High risk of near-crash driving events following night-shift work. Proc Natl Acad Sci U S A. 2016 Jan 5;113(1):176-81
- Reichert CF, Deboer T, Landolt HP. Adenosine, caffeine, and sleep-wake regulation: state of the science and perspectives. J Sleep Res. 2022 Aug;31(4):e13597
- Wahl S, Engelhardt M, Schaupp P, Lappe C, Ivanov IV. The inner clock-Blue light sets the human rhythm. J Biophotonics. 2019 Dec;12(12):e201900102
- Adam EK, Quinn ME, Tavernier R, McQuillan MT, Dahlke KA, Gilbert KE. Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology. 2017 Sep;83:25-41
- Boivin DB, Boudreau P, Kosmadopoulos A. Disturbance of the Circadian System in Shift Work and Its Health Impact. J Biol Rhythms. 2022 Feb;37(1):3-28
- Baranwal N, Yu PK, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis. 2023 Mar-Apr;77:59-69
- Shen B, Ma C, Wu G, Liu H, Chen L, Yang G. Effects of exercise on circadian rhythms in humans. Front Pharmacol. 2023 Oct 11;14:1282357
- Iao SI, Jansen E, Shedden K, O’Brien LM, Chervin RD, Knutson KL, Dunietz GL. Associations between bedtime eating or drinking, sleep duration and wake after sleep onset: findings from the American time use survey. Br J Nutr. 2021 Sep 13;127(12):1-10
- Colrain IM, Nicholas CL, Baker FC. Alcohol and the sleeping brain. Handb Clin Neurol. 2014;125:415-31
- Kaul M, Zee PC, Sahni AS. Effects of Cannabinoids on Sleep and their Therapeutic Potential for Sleep Disorders. Neurotherapeutics. 2021 Jan;18(1):217-227
- Chang AM, Aeschbach D, Duffy JF, Czeisler CA. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc Natl Acad Sci U S A. 2015;112(4):1232-1237
- Tang NK, Anne Schmidt D, Harvey AG. Sleeping with the enemy: clock monitoring in the maintenance of insomnia. J Behav Ther Exp Psychiatry. 2007 Mar;38(1):40-55
- Blume C, Garbazza C, Spitschan M. Effects of light on human circadian rhythms, sleep and mood. Somnologie (Berl). 2019 Sep;23(3):147-156
- Waggoner LB, Concannon TW, Darby MJ. Designing shift schedules for reduced fatigue and improved health outcomes. J Emerg Nurs. 2012;38(6):571-573
- Dunbar M, Gray S. Shift work fatigue and medical errors: is 11 hours enough? CJEM. 2022;24(S1):S74.
- Di Muzio M, Diella G, Di Simone E, Pazzaglia M, Alfonsi V, Novelli L, Cianciulli A, Scarpelli S, Gorgoni M, Giannini A, Ferrara M, Lucidi F, De Gennaro L. Comparison of Sleep and Attention Metrics Among Nurses Working Shifts on a Forward- vs Backward-Rotating Schedule. JAMA Netw Open. 2021 Oct 1;4(10):e2129906
- Hittle BM, Gillespie GL. Identifying shift worker chronotype: implications for health. Ind Health. 2018 Nov 21;56(6):512-523
- Boukhris O, Trabelsi K, Ammar A, Abdessalem R, Hsouna H, Glenn JM, Bott N, Driss T, Souissi N, Hammouda O, Garbarino S, Bragazzi NL, Chtourou H. A 90 min Daytime Nap Opportunity Is Better Than 40 min for Cognitive and Physical Performance. Int J Environ Res Public Health. 2020 Jun 28;17(13):4650
- Lovato N, Lack L. The effects of napping on cognitive functioning. Prog Brain Res. 2010;185:155-66
- Hogan CL, Mata J, Carstensen LL. Exercise holds immediate benefits for affect and cognition in younger and older adults. Psychol Aging. 2013 Jun;28(2):587-94
- Institute of Medicine (US) Committee on Military Nutrition Research; Marriott BM, editor. Food Components to Enhance Performance: An Evaluation of Potential Performance-Enhancing Food Components for Operational Rations. Washington (DC): National Academies Press (US); 1994. 20, Effects of Caffeine on Cognitive Performance, Mood, and Alertness in Sleep-Deprived Humans. Available from:
- Costello RB, Lentino CV, Boyd CC, O’Connell ML, Crawford CC, Sprengel ML, Deuster PA. The effectiveness of melatonin for promoting healthy sleep: a rapid evidence assessment of the literature. Nutr J. 2014 Nov 7;13:106
- Scharner V, Hasieber L, Sönnichsen A, Mann E. Efficacy and safety of Z-substances in the management of insomnia in older adults: a systematic review for the development of recommendations to reduce potentially inappropriate prescribing. BMC Geriatr. 2022 Feb 1;22(1):87
- Czeisler CA, Walsh JK, Roth T, et al. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353(5):476-486
- Wickwire EM, Geiger-Brown J, Scharf SM, Drake CL. Shift Work and Shift Work Sleep Disorder: Clinical and Organizational Perspectives. Chest. 2017 May;151(5):1156-1172
- Minzenberg MJ, Carter CS. Modafinil: a review of neurochemical actions and effects on cognition. Neuropsychopharmacology. 2008 Jun;33(7):1477-502.
Dr. Michael Mack has received unrestricted educational funds from Paladin, Eisai, Jazz Pharmaceuticals, and ResMed to support the Sleep Medicine Fellowship in the Department of Psychiatry at the University of Toronto.



Leave A Comment