
Resuscitation

Best Case Ever 43 Ruptured AAA
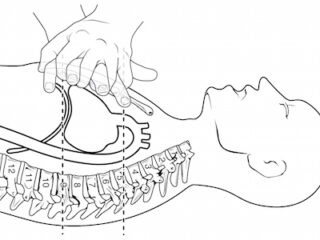
I caught up with Dr. Anand Swaminathan, otherwise known as EM Swami, at The Teaching Course in NYC where he told his Best Case Ever from Janus General of his heroic and collaborative attempts at saving the life of a gentleman who presented to the ED with a classic story for a ruptured AAA. As William Olser famously said, "There is no disease more conducive to clinical humility than aneurysm of the aorta."

Best Case Ever 42 Pediatric Cardiac Arrest
When was the last time you saw ventricular fibrillation in a 4 month old? Dr. Simard tells his Best Case Ever of a Pediatric Cardiac Arrest in which meticulous preparation, sticking to his guns, early activation of the transportation service, and clever use of point of care ultrasound helped save the life of a child. He explains the importance of debriefing your team after an emotionally charged case.

Episode 72 ACLS Guidelines 2015 Post Arrest Care
Once we've achieved ROSC our job is not over. Good post-arrest care involves maintaining blood pressure and cerebral perfusion, adequate sedation, cooling and preventing hyperthermia, considering antiarrhythmic medications, optimization of tissue oxygen delivery while avoiding hyperoxia, getting patients to PCI who need it, and looking for and treating the underlying cause. Dr. Lin and Dr. Morrison offer us their opinion on the new simplified approach to diagnosing the underlying cause of PEA arrests. We'll also discuss when it's time to terminate resuscitation or 'call the code' as well as some fascinating research on gender differences in cardiac arrest care. These co-authors of the guidelines will give us their vision of the future of cardiac arrest care and we'll wrap up the episode with a third opinion, so to speak: Dr. Weingart's take on the whole thing....
Episode 71 ACLS Guidelines 2015 – Cardiac Arrest Controversies Part 1
A lot has changed over the years when it comes to managing the adult in cardiac arrest. As a result, survival rates after cardiac arrest have risen steadily over the last decade. With the release of the 2015 American Heart Association ACLS Guidelines 2015 online on Oct 16th, while there aren’t a lot a big changes, there are many small but important changes we need to be aware of, and there still remains a lot of controversy. In light of knowing how to provide optimal cardio-cerebral resuscitation and improving patient outcomes, in this episode we’ll ask two Canadian co-authors of The Guidelines, Dr. Laurie Morrison and Dr. Steve Lin some of the most practice-changing and controversial questions.
Episode 69 Obesity Emergency Management
Current estimates of the prevalence of obesity are that a quarter of adult Canadians and one third of Americans are considered obese with approximately 3% being morbidly obese. With the proportion of patients with a BMI>30 growing every year, you’re likely to manage at least one obese patient on every ED shift. Obese patients are at high risk of developing a host of medical complications including diabetes, hypertension, coronary artery disease, peripheral vascular disease, biliary disease, sleep apnea, cardiomyopathy, pulmonary embolism and depression, and are less likely compared to non-obese adults to receive timely care in the ED. Not only are these patients at higher risk for morbidity and mortality, but obesity emergency management is complicated by the patient’s altered cardiopulmonary physiology and drug metabolism. This can make their acute management much more challenging and dangerous. To help us gain a deeper understanding of the challenges of managing obese patients and elucidate a number of important differences as well as practical approaches to obesity emergency management, we welcome Dr. Andrew Sloas, the founder and creator of the fantastic pediatric EM podcast PEM ED, Dr. Richard Levitan, a world-famous airway management educator and innovator and Dr. David Barbic a prominent Canadian researcher in obesity in emergency medicine from University of British Columbia....

Best Case Ever 39 – Airway Strategy & Mental Preparedness in EM Procedures with Richard Levitan
I caught up with airway educator, innovator and self-described enthusiast Dr. Richard Levitan at SMACC in Chicago this past June. In this Best Case Ever on Airway Strategy and Mental Preparedness in EM Procedures, Dr. Levitan uses a great save of his in a penetrating trauma case as a basis for discussion on mental preparedness and how we've been thinking about our general approach to emergency procedures the wrong way. Rather than fixating on the final goal of a procedure, which can often be daunting and lead us astray, he suggests a methodical incrementalized and compartmentalized approach to EM procedures that reduces stress and fear, improves confidence and enhances success. He runs through several examples including intubation, cricothyrotomy and initial approach to hypoxia to explain his Simple Incremental Approach to EM Procedures. Could this be a paradigm shift in the way we think about procedures in EM?....
