
Convulsive status epilepticus is one of the most morbid neurologic emergencies we manage in the ED, and outcomes depend far more on speed than drug selection. Like ventricular fibrillation, each minute of ongoing convulsions worsens hypoxia, acidosis, cardiovascular instability, and neuronal injury, while making seizures progressively harder to terminate. Modern definitions are intentionally time-compressed to force early, parallel, clock-anchored action. Any patient still convulsing when you reach the bedside should be treated as evolving status epilepticus.
In this EM Cases podcast with Dr. Sara Gray, we take a practical, time-based approach to convulsive status epilepticus, focusing on early, adequately dosed benzodiazepines, avoiding common escalation and dosing pitfalls, anticipating post-ictal cardiovascular collapse, and knowing when to escalate to second-line agents, airway control, and anesthetic-dose therapy. We also address the transition to non-convulsive status epilepticus and how to recognize ongoing seizures when EEG is not immediately available.
We answer questions such as: Why does time to first benzodiazepine matter more than the drug or route? What critical actions should occur in parallel with the first dose? Why is underdosing second-line antiseizure medications—especially levetiracetam—a common and dangerous pitfall? What are 3 key actions to do in parallel with the first benzodiazepine? When should persistent seizures trigger intubation and anesthetic-dose therapy? How can we identify non-convulsive status epilepticus once tonic-clonic activity stops? And many more (we also include a high yield status epilepticus management algorithm!)…
If you find EM Cases helpful in your clinical practice, please consider supporting our work so we can continue producing free, high-quality emergency medicine education for clinicians around the world.
Make a donation here: https://emergencymedicinecases.com/donation/
Podcast: Play in new window | Download (Duration: 59:25 — 54.5MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Anton Helman, February 2026
Cite this podcast as: Helman, A. Gray, S. Update in Management of Status Epilepticus. Emergency Medicine Cases. February, 2026. https://emergencymedicinecases.com/upate-management-status-epilepticus. Accessed July 21, 2026
Why management of status epilepticus is a race against time
Convulsive status epilepticus (CSE) is one of the most destructive neurologic emergencies we see in the ED, with high risks of death and long‑term disability when seizures are not shut down quickly. Prolonged seizures drive acidosis, cardiovascular collapse, and neuronal injury; outcomes track closely with both total seizure duration and time to first benzodiazepine. Modern definitions and management aim to make us act earlier, anchor decisions to the clock, and anticipate post‑ictal physiologic collapse rather than reacting late.
Working definition of convulsive status epilepticus
- Generalized tonic–clonic activity lasting >5 minutes, or
- Recurrent seizures without recovery of baseline neurologic function between events.
Most isolated seizures terminate within 1–3 minutes, but beyond a few minutes, GABA receptors internalize and excitatory pathways upregulate, making seizures self‑perpetuating and benzodiazepine‑resistant. Any patient still convulsing by the time you are at the bedside should be presumed to be in status and treated as such.
First five minutes: parallel actions and first‑line benzodiazepines
Time to first benzodiazepine is the key determinant of outcomes
The key determinant of success in management of status epilepticus is time to first benzo, not which benzo or route you choose. Early treatment reduces total dose needed and lowers the chance of progression to refractory status; delaying “to see if it stops” exposes the patient to more apnea, hypoxia, hypotension, and neuronal injury than the drug does.
Decision to Initiate the First Benzodiazepine
The decision to administer the first benzodiazepine should be guided by ongoing seizure activity at the point of clinical intervention, rather than strict adherence to a five-minute time threshold. Although many seizures self-terminate within one to three minutes, by the time emergency care is initiated a patient who is still seizing has effectively declared evolving status epilepticus. Delaying treatment to observe for spontaneous resolution risks progression to pharmacoresistant seizures, as prolonged convulsions are associated with reduced benzodiazepine responsiveness and increasing excitatory neurotransmission. Importantly, respiratory depression and hypotension are more strongly linked to ongoing seizure activity than to early, adequately dosed benzodiazepines, supporting prompt and decisive first-line treatment once seizure activity persists.
Think parallel, not sequential. From the moment you recognize ongoing convulsions, call for help, assign roles, and start a team-visible timer; our perception of time compresses dramatically during seizures.
Key actions to do in parallel with the first benzodiazepine
- Check capillary glucose A-B-C– D‑E‑F‑G: “Don’t Ever Forget Glucose.”
- Send a STAT VBG with electrolytes, specifically to screen for severe hyponatremia or other life‑threatening metabolic derangements early – this will alter management significantly (see below)
- Anticipate post‑ictal hypotension: have norepinephrine mixed and ready; many patients will need vasopressor support once the seizure and catecholamine surge terminate, especially after adequate benzo and propofol dosing.
Benzodiazepines (0–5 minutes)
- Preferred: Lorazepam 4 mg IV push (consider 8mg in patients with alcohol or benzodiazpeine withdrawal seizures and those with high BMI); some experts recommend 2mg IV in rapid succession for repeat every 2–3 minutes to a total up to about 8 mg in large, tolerant, or alcohol‑use‑disorder patients.
- Alternative IV: Midazolam 5–10 mg IV; be prepared for repeat dosing or infusion because of its shorter CNS effect.
- No IV access: Midazolam 10 mg IM; prehospital RCTs show IM midazolam is at least as effective as IV benzos when you factor in earlier delivery.
Pearl: Ask for multiple pre‑drawn benzo doses up front so you can redose every 2–3 minutes without pharmacy trips or hesitation.
Second 5 minutes (5–10): second‑line antiseizure meds and reversible causes
By 5 minutes of ongoing convulsions, your patient meets the modern definition of status and should already be loading a second‑line antiseizure medication. Do not wait to “see what the benzo does” once you cross this time point.
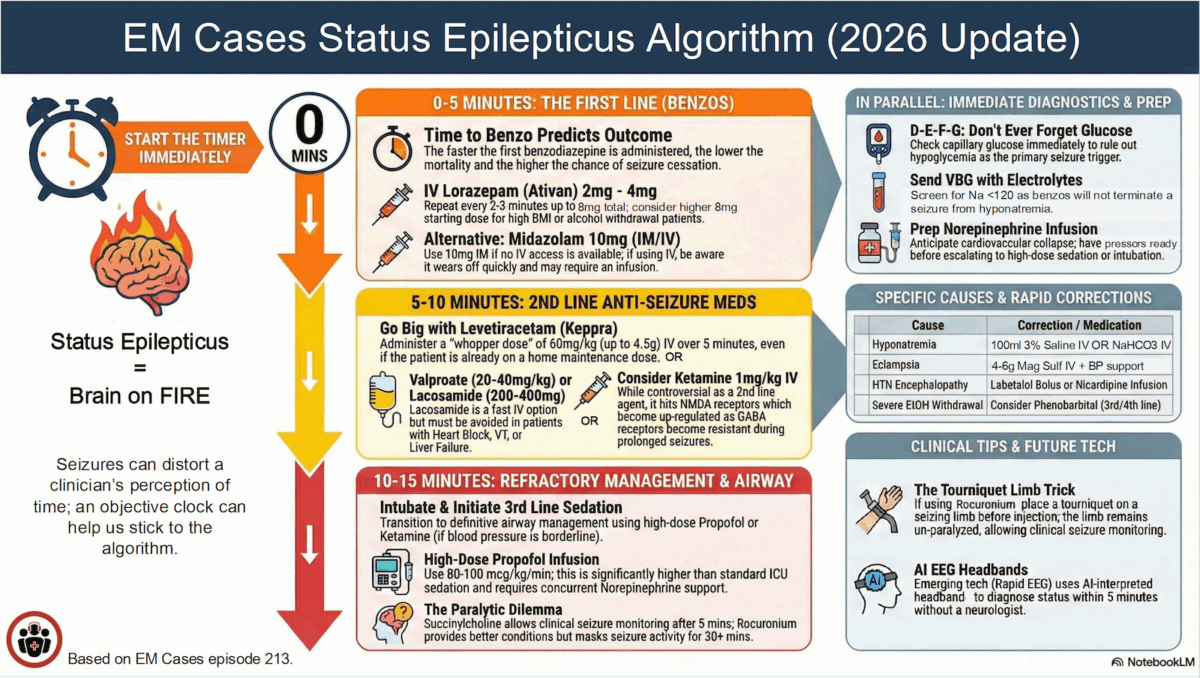
Time‑anchored escalation framework in management of status epilepticus
- 0–5 minutes: Benzodiazepines
- 5–10 minutes: Second‑line IV antiseizure medication
- 10–15 minutes: Intubation and anesthetic‑dose therapy
Evidence‑supported second‑line options in the management of status epilepticus
Large multicenter trials (e.g., ESETT) suggest equivalent efficacy between the major second‑line agents when used at full doses.
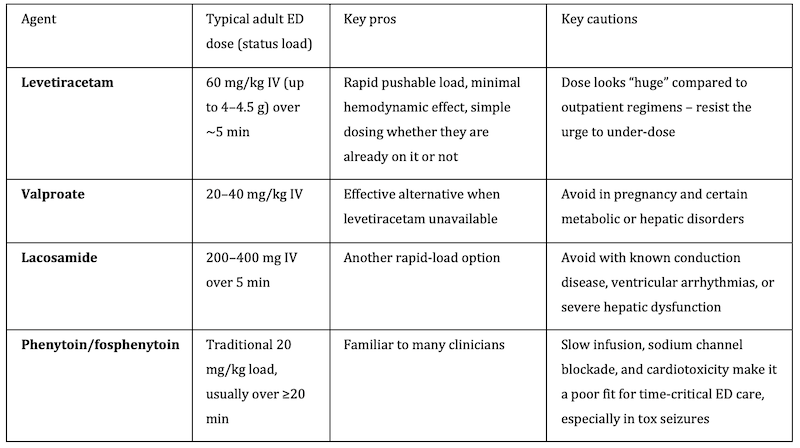
Common Pitfall: A common pitfall is underdosing 2nd line medications. Second‑line doses are intentionally large; full loading (especially levetiracetam 60 mg/kg) is necessary to portend the best chance of terminating status.
Reversible precipitants/causes of status epilepticus to address in parallel
Do not delay antiseizure therapy while chasing causes, but treat likely reversible drivers early.
- Hypoglycemia: Give IV dextrose immediately.
- Hyponatremia: Give 3% saline 100 mL IV boluses; where hypertonic saline is unavailable, repeated amps of sodium bicarbonate can provide an alternative sodium load.
- Eclampsia: Magnesium sulfate 4–6 g IV over ~15 minutes, then infusion; antihypertensives in parallel; watch for hypotension and be ready with norepinephrine.
- Hypertensive encephalopathy: Control BP with labetalol boluses (e.g., 20 mg) or nicardipine infusion, depending on local availability.
- Toxicologic etiologies: Consider sodium channel blocker toxicity, isoniazid, etc. and use targeted antidotes where applicable.
Third 5 minutes (10–15) of status epilepticus management: airway, anesthetic‑dose therapy, refractory status
Ongoing convulsions beyond the second‑line window should trigger definitive airway management and escalation to anesthetic‑dose therapy.
Indications to intubate in management of status epilepticus
- Persistent convulsions despite adequate benzos and a full second‑line load
- Apnea, loss of airway reflexes, aspiration risk
- Need for continuous high‑dose sedative infusions and neuromuscular blockade
Induction and paralysis
- Induction: Many clinicians prefer propofol; ketamine is reasonable, especially when baseline blood pressure is marginal. Expect to require vasopressors regardless of agent once high‑dose infusions are running.
- Paralytic options:
- Succinylcholine is appropriate when seizure onset is clearly <20–25 minutes, as hyperkalemia risk is low and its short duration lets you reassess clinical seizure activity within minutes.
- Rocuronium offers the best intubating conditions when onset time is uncertain or seizures are prolonged, but its longer duration masks ongoing convulsions. Sugammadex, where available, can effecively reverse the effects of rocuronium within 1-2 minutes in studies, however this drug is often not immediately available in many EDs.
Pearl: The Tourniquet limb trick: Before rocuronium, apply a tight tourniquet to the limb with the most obvious clonic activity; this prevents paralytic from reaching the limb and preserves a crude but useful visual monitor for ongoing seizure in the absence of EEG.
Post‑intubation infusions in management of status epilepticus
- High‑dose propofol: Think anesthetic doses, not routine sedation: roughly 80–100 micrograms/kg/min (or 5–10 mg/kg/h, depending on your pump convention).
- Continuous benzo and additional antiseizure agents (e.g., ongoing levetiracetam, valproate, ± lacosamide) are typically layered in by ICU teams for refractory and super‑refractory cases.
- Norepinephrine: Start early; most intubated, heavily sedated status patients will need vasopressors to maintain perfusion.
Pitfall: underdosing propofol infusion is a common pitfall in the management of refractory status epilepticus; think anesthetic doses of 80-100 microgram/kg/min (5-10mg/kg/h), not routine sedation doses.
Refractory status epilepticus—persistent seizures despite adequate benzo and at least one full second‑line agent—usually mandates ICU admission, continuous EEG where available, and prolonged high‑dose sedative and antiseizure therapy with gradual weans once EEG silence is achieved.
Special scenarios: non‑convulsive status epilepticus (NCSE) and monitoring the “post‑ictal” patient
Cessation of visible tonic–clonic activity does not guarantee that seizures have stopped. Patients who fail to show meaningful neurologic recovery within about an hour should be assumed to have non‑convulsive status until proven otherwise by EEG.
At the bedside, clues include persistent eye deviation, nystagmus, blinking, subtle facial or limb twitching, or an otherwise “off” level of awareness. A practical approach is to fully expose the patient, scrutinize the eyes and small muscle groups, and maintain a low threshold to treat ongoing subtle activity with additional benzodiazepines and antiseizure therapy. Emerging AI‑interpreted EEG headbands may eventually give EDs near‑real‑time seizure detection, but at present continuous EEG remains a scarce resource in many systems.
Key take home points for Update in Management of Status Epilepticus
- Status epilepticus is a race against time. Outcomes track most closely with total seizure duration and, above all, time to first benzodiazepine.
- Any patient still convulsing when you reach the bedside should be treated as status epilepticus, without waiting for a rigid five-minute threshold. Beyond a few minutes, seizures become self-perpetuating and increasingly benzodiazepine-resistant.
- Think parallel, not sequential, and start a team-visible timer. Time perception compresses during seizures, and clock-anchored escalation (0–5, 5–10, 10 minutes) prevents dangerous delays.
- With the first benzodiazepine, act in parallel: check capillary glucose, send a STAT blood gas with electrolytes (especially sodium), and prepare norepinephrine for anticipated post-ictal hypotension.
- Benzodiazepines must be dosed adequately and re-dosed early. Lorazepam 4 mg IV push (up to 8 mg IV push in patients with known alcohol withdrawal and/or high BMI) with rapid repeat dosing every 2–3 minutes; IM midazolam 10 mg is effective when IV access is delayed.
- By 5 minutes of ongoing convulsions, a full-dose second-line antiseizure medication should already be loading, and timing and dose matter more than drug choice. Large RCTs show similar efficacy among agents such as levetiracetam, valproate, and lacosamide when used appropriately, and underdosing—particularly of levetiracetam—is a common and avoidable pitfall.
- Ketamine may be considered earlier in selected patients but is not yet universal second-line therapy. A 1 mg/kg IV dose may be reasonable in early benzodiazepine resistance or borderline hemodynamics.
- Persistent seizures beyond 10 minutes require airway control and anesthetic-dose therapy. Intubate when indicated, use anesthetic-range propofol dosing, start norepinephrine early, and assume non-convulsive status epilepticus if neurologic recovery is delayed.
References
- Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3‑23.
- Smith DM, et al. Guidance for the acute management of status epilepticus in adult patients. Pract Neurol. 2025;25(3):180‑194.
- Emergency Department Management of Patients With Status Epilepticus. Emerg Med Pract. 2025;27(9):1‑24.
- Strategies to innovate emergency care of status epilepticus. Emerg Med J. 2024;41(12):845‑852.
- Mullhi R, Hayton T, Midgley-Hunt A, et al. Guidance for the acute management of status epilepticus in adult patients. J Intensive Care Soc. 2025.
- Glauser T, Shinnar S, Gloss D, et al. Evidence‑based guideline: Treatment of convulsive status epilepticus in children and adults. Epilepsy Curr. 2016;16(1):48‑61.
- Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus: Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015;56(10):1515‑1523.
- Kapur J, Elm J, Chamberlain JM, et al. Randomized trial of three anticonvulsant medications for status epilepticus (ESETT). N Engl J Med. 2019;381(22):2103‑2113.
- Silbergleit R, Durkalski V, Lowenstein D, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus (RAMPART). N Engl J Med. 2012;366(7):591‑600.
- Sánchez Fernández I, Gainza‑Lein M, Chapman KE, et al. Time‑dependent changes in treatment response in convulsive status epilepticus: A systematic review. Seizure. 2014;23(9):708‑716.
- Köhle F, Madlener M, Bruno EF, et al. Status epilepticus and benzodiazepine treatment: Use, underdosing and outcome—insights from a retrospective, multicentre registry. Seizure. 2023;109:1–8.
- Rossetti AO, Alvarez V, Burnand B, et al. Treatment deviating from guidelines does not influence status epilepticus prognosis. J Neurol. 2013;260(2):421‑428.
- Legriel S, Oddo M, Brophy GM. Ketamine for the treatment of refractory status epilepticus. Neurocrit Care. 2015;22(2):153‑160.
- Hsieh CY, Sung CW, Fan JS, et al. Ketamine use in refractory status epilepticus in the emergency department: A retrospective observational study. Am J Emerg Med. 2022;56:120‑126.
- Efficacy of Intravenous Ketamine in Status Epilepticus. Epilepsia. 2025;66(12):e101‑e112.
- Zitek T, Tanone I, Buckley R, et al. Ketamine for the treatment of convulsive status epilepticus in the emergency department. Ann Emerg Med. 2025.
- Rosati A, L’Erario M, Ilvento L, et al. Efficacy and safety of ketamine in refractory status epilepticus in adults and children: A systematic review. CNS Drugs. 2023;37(1):1–15.
- Williams NC, Koenig KL, Kahn SA. Ketamine in the management of status epilepticus and refractory seizures. Am J Emerg Med. 2024.
- Aldhafeeri BF, Alsaleh M, Al-Mutairi R, et al. Efficacy of intravenous ketamine in refractory and super-refractory status epilepticus: A systematic review and meta-analysis. Epilepsia. 2025.
- Falksen JA, Schomer KJ, Dodd KW, et al. Neurologic examination facilitated by reversal of rocuronium with sugammadex. J Intensive Care Med. 2024;39(10):971‑978.
- Cormack JR, Brull SJ, Prielipp RC. To reverse or not to reverse: Sugammadex and rocuronium in the emergency setting. Anesth Analg. 2018;126(1):31‑35.
- Jansson PS, et al. Emergency department use of sugammadex to facilitate neurologic assessment after neuromuscular blockade. Acad Emerg Med. 2024.
- Herman ST, Abend NS, Bleck TP, et al. Consensus statement on continuous EEG in critically ill adults and children, part I: Indications. J Clin Neurophysiol. 2015;32(2):87‑95.
- Sivaraju A, Obiako R, Drislane FW. Nonconvulsive status epilepticus in the emergency department. Epilepsy Behav. 2015;49:158‑163.
- Burman RJ, Semple BD, Read J, et al. Time‑critical treatment of status epilepticus: Pathophysiologic rationale and practical recommendations. Pract Neurol. 2023;23(1):45‑56.
Drs. Helman and Gray have no conflicts of interest to declare
Now test your knowledge with a quiz.



Nice updates