
In this ECG Cases blog we look at 5 unstable patients with tachycardia. Do they need cardioversion or another treatment?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. February 2026
Five unstable patients presented with tachycardia. Do they need cardioversion per the ACLS algorithm, or something else?
Case 1: 60yo with chest pain
–
Case 2: 90yo with weakness, fever and hypotension.
–
Case 3: 75yo with acute CHF and hypoxia.
–
Case 4: 70yo with sepsis and hypotension.
–
Case 5: 55yo chest pain. VT?
–
Unstable tachycardia: Cardiovert?
This is the third in a series of blog posts on the pitfalls of ACLS algorithms for adults with a pulse, and how a systematic approach to 12-lead ECG can help with ECG acquisition, interpretation, and application. The first looked at unstable bradycardia, the second stable bradycardia, and this one will look at unstable tachycardia.
The ACLS algorithm for unstable tachyarrhythmia is simple: immediate cardioversion. This works well if it is a primary tachyarrythmia that is causing the instability (eg SVT or VT), but there are a number of pitfalls in this assumption.
- ECG acquisition: is it actually a tachy-arrhythmias? Artifact can mimic a tachy-arrhythmia. This can be identified by unaffected leads recorded at the same time, and narrow QRS complexes marching through the noise
- ECG interpretation: is the tachy-arrhythmia a primary electrical problem? There are other tachycardias in unstable patients that may fail to respond to cardioversion:
- AF (irregularly irregular rhythm), where the patient’s instability may be related to a secondary cause
- Sinus tachycardia (in response to a secondary cause): can best be identified by upright P waves in II and biphasic P waves in V1.
- ECG application: Is the rhythm causing the instability, or is there a secondary cause – including one that might be revealed by the 12-lead, like hyperkalemia or occlusion MI?
Back to the cases
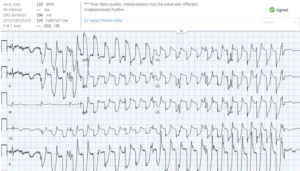
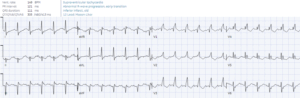
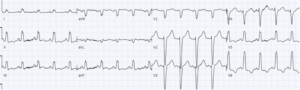
Case 1: 60yo with chest pain
Artifact: bizarre polymorphic complexes sparing lead III, which shows sinus rhythm. Repeat ECG unremarkable, and labs normal
–
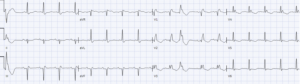
Case 2: 90yo with weakness, fever and hypotension.
- Heart rate/rhythm: irregularly irregular rhythm without P waves (AF), with PVCs, and rapid ventricular response
- Electrical conduction: typical LBBB
- Axis: normal
- R-wave progression: transition V5 (LBBB)
- Tall/small voltages: tall voltages
- ST/T: discordant and proportional ST, secondary to LBBB
= AF with RVR and LBBB. After treatment for sepsis the heart rate improved and the AF spontaneously cardioverted to sinus rhythm, with ongoing LBBB
–
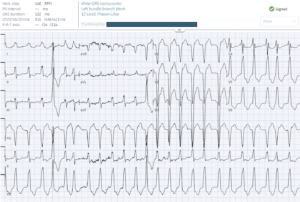
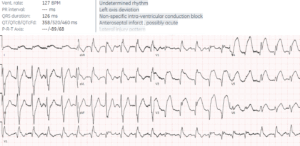
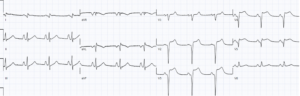
Case 3: 75yo with acute CHF and hypoxia.
- H: regular wide complex tachycardia driven by P waves (upright in II, also well seen V4) = sinus tach
- E: typical LBBB
- A: normal
- R: transition V5 (LBBB)
- T: normal
- S: discordant and proportional (secondary to LBBB)
=sinus tach, not VT. Not initially identified so had cardioversion, which failed. After secondary cause treated (nitro/bipap for CHF) the rate slowed:
–
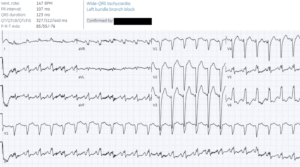
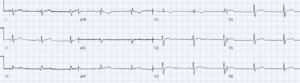
Case 4: 70yo with sepsis and hypotension.
- H: regular wide complex tachy driven by P waves (biphasic in V1) = sinus tach
- E: RBBB
- A: left from inferior infarct
- R: early from RBBB
- T: normal
- S: anterior STD/TWI secondary to RBBB
= sinus tach not SVT. Not initially identified so the patient had cardioversion, which failed. After treatment for the secondary cause (sepsis) the heart rate slowed:
–
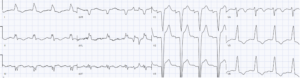
Case 5: 55yo chest pain. VT?
- H: sinus tach
- E: intermittent RBBB
- A: left axis from LAFB
- R: Q wave and intermittent early R from RBBB
- T: normal
- S: anterolateral STE/hyperacute
= proximal LAD occlusion with bifascicular block, and tachycardia from cardiogenic shock. Cath lab activated: proximal LAD occlusion. After reperfusion the heart rate slowed and the bifascicular block resolved, but Q waves remained.
–
Take home points for unstable tachycardia, cardiovert?
- Artifact mimicking tachy-arrhythmia: repeat
- Unstable from primary tachy-arrhytmia (eg VT, SVT): cardiovert per ACLS
- Unstable and tachycardic from secondary cause (eg sinus tach, AF with RVR from secondary cause): treat underlying cause
For live and highly interactive ECG courses to elevate your skills – including online courses, or an in-person pre-conference course at CAEP, go to www.heartsECGcourse.com



Leave A Comment