
In this ECG Cases blog we look at an approach to Takotsubo syndrome through 10 patients with ECGs demonstrating ST elevation or T wave inversion.
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. September 2022
10 patients presented with cardiorespiratory symptoms and ST elevation and/or T wave inversion. Which had Takotsubo syndrome?
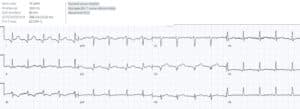
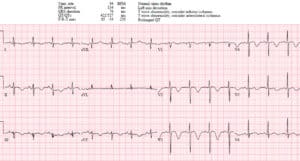
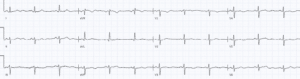
Case 1: 50 year old with 12 hours of chest pain and shortness of breath, cocaine few days prior

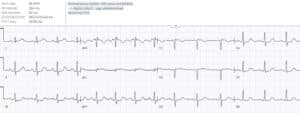
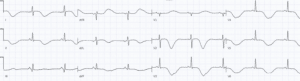
Case 2: 45 year old with acute exertional chest pain
Case 3: 50 year old with acute chest pain, diaphoresis and vomiting, two days after a funeral
Case 4: 80 year old with 6 hours of chest pain

Case 5: 70 year old found aphasic, right hemiparesis

Case 6: 45 year old, recent pneumonia, with one week shortness of breath

Case 7: 35 year old with shortness of breath on exertion
Case 8: 70 year old with one week shortness of breath on exertion, asymptomatic at rest

Case 9: 75 year old with chest pain and shortness of breath, hypoxic
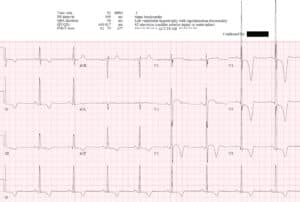
Case 10: 50 year old, recent admission for thyrotoxicosis, with one week shortness of breath and weakness

Takotsubo – two ECG mimics
Takotsubo syndrome (TTS) is reversible LV dysfunction in the absence of pre-existing cardiomyopathy or obstructive coronary disease. It goes by many names, which explain the syndrome.
Trigger: primary TTS is triggered by an emotional stress (“broken heart syndrome”) or no obvious trigger, while secondary TTS is triggered by any physical stress (“stress cardiomyopathy”) ranging from sepsis and CNS catastrophes (“neurogenic stunned myocardium”) to surgery or substance use.
Pathophysiology: the stressful trigger leads to a surge in catecholamines that produces microvascular vasoconstriction and myocardial stunning, leading to the description of “acute catecholaminergic myocardial stunning.”
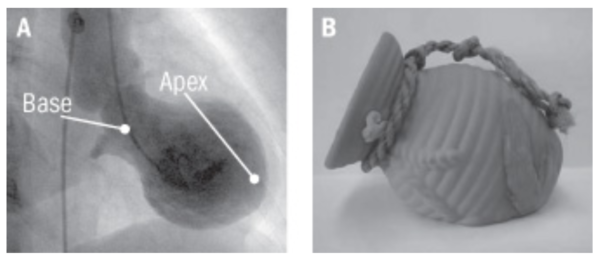
Distribution: myocardial stunning typically affects the apex of the heart, which balloons while the base contracts—leading to the term “apical ballooning syndrome”—and this resembles the pots used in Japan to trap octopus (called tako-tsubo). [1,2,3]

Patients with TTS can present with symptoms of myocardial stunning (chest pain, shortness of breath, syncope) or with its complications (cardiogenic shock, stroke from apical emboli, arrhythmias, or cardiac arrest). This produces a modest elevation in troponin (less than expected given regional wall motion abnormalities) and significant rise in BNP. But with supportive treatment—including managing CHF and arrhythmias, preventing thrombo-embolism, and treating triggers of secondary TTS—there is recovery of LV function. This makes TTS a retrospective diagnosis of exclusion—with an angiogram ruling out occlusion, a ventriculogram showing apical ballooning, and a follow up echo showing recovery of LV function. [1,4]
While we will not make the diagnosis of TTS in the ED, we will see patients who present with one of two phases of ECG changes—ST elevation or T wave inversion.[5] The first mimics acute coronary occlusion and requires immediate cath lab activation, while the second has a broader differential including reperfusion.
- ST elevation mimicking STEMI/Occlusion MI: cath lab activation
The acute phase of TTS produces ST elevation +/- Q waves, as a result of microvascular vasoconstriction that mimics acute coronary occlusion. Faced with ischemic symptoms and ST elevation, there are no demographic, ECG or POCUS findings that can confirm TTS and exclude Occlusion MI. Especially considering TTS is rare (2% of suspected STEMI), the diagnosis is based on angiographic exclusion of obstructive coronary disease and recovery of LV function, and the treatment is supportive. This is further complicated by 15% of patients with TTS having concomitant coronary artery disease, and the possibility of spontaneous reperfusion prior to angiography.
While postmenopausal women are the large majority of patients with TTS, this population is also underdiagnosed and undertreated for ACS[6]—so anchoring on history of recent stress or absence of cardiovascular risk factors could lead to delayed reperfusion for Occlusion MI. Because TTS usually affects the apex, it often produces ST elevation V2-5 and II, without the inferior ST depression typically associated with anterior STEMI. But TTS can be midventricular or focal, LAD occlusion beyond the first diagonal does not produce inferior ST depression, and wraparound or distal LAD occlusion can produce both anterior and inferior ST elevation.[7,8]
- T wave inversion with a long QT: differential and admission
After the acute phase of TTS, the ST elevation and Q waves resolve and there’s development of T wave inversion that reflects myocardial edema and stunning. T wave inversion has a broad differential, and when present in both anterior and inferior leads this includes apical hypertrophic cardiomyopathy (LVH with secondary T wave inversion), pulmonary embolism (primary T wave inversion from RV strain), or wraparound LAD reperfusion (primary T wave inversion with resolved symptoms).
There are sometimes differences in the distribution of T wave inversion: antero-inferior (but not lateral) in PE with RV strain, anterior +/- lateral (+/- inferior if wraparound/distal) in LAD reperfusion, and more diffuse in TTC. [9] TTS often develops giant T wave inversions, which are very deep and with a QT interval which is very long.[4,10]
Because this phase mimics reperfusion rather than occlusion, and there is a broader differential, there is no need for immediate angiography. But these patients require admission to rule out coronary artery disease, manage the complications of TTS, and treat triggers.
Back to the cases
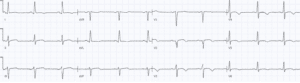
Case 1: query primary TTS mimicking proximal LAD occlusion, vs spontaneous reperfusion or spasm
- H: normal sinus rhythm
- E: normal conduction
- A: normal axis
- R: poor R wave progression
- T: normal voltages
- S: concave ST elevation V1-2 with hyperacute T waves, and I/aVL with reciprocal TWI in III/aVF
Impression: ECG appearance of proximal LAD occlusion. Cath lab activated: 50% stenosis of left main and LAD, EF 35% with akinetic apex without thrombus, troponin 14,000. Diagnosed with TTS because of echo findings, lack of occlusion at the time of angiogram, and recent patient stresses. But could have been LAD occlusion that reperfused by the time of the angiogram, or spasm from recent cocaine use. Discharge ECG showed precordial and inferior T wave inversion with normal QT interval, no follow up echo available to confirm reversible LV dysfunction.
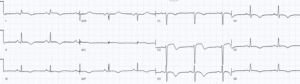
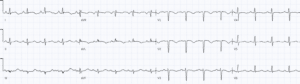
Case 2: primary TTS mimicking first diagonal occlusion
- H: normal sinus rhythm
- E: normal conduction
- A: normal axis
- R: Q waves V2-3
- T: normal voltages
- S: ST elevation with Q waves I/aVL/V2, with reciprocal STD/TWI in III
Impression: ECG appearance of first diagonal STEMI(+)OMI. Cath lab activated: normal coronaries, LV ballooning, first troponin 400ng/L and peak 5,000. Subsequent ECG developed precordial and inferior deep T wave inversion with long QT interval, typical of TTS, with improvement by discharge
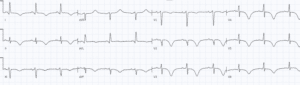
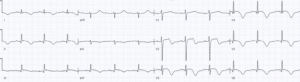
Case 3: primary TTS (“broken heart syndrome”) mimicking first diagonal STEMI(-)OMI
- H: normal sinus rhythm
- E: normal conduction
- A: normal axis
- R: Q wave in V2, otherwise normal R wave progression
- T: normal voltages
- S: mild concave ST elevation and hyperacute T wave I/aVL, Q in aVL/V2, and reciprocal ST depression III/aVF
Impression: ECG appearance of first diagonal STEMI(-)OMI. Cath lab activated: normal coronaries, first troponin 200ng/L and peak 5000. Echo: mid cavitary akinesis with EF 25%, recovered to 50% by discharge. Post-cath ECG had mild anterolateral T wave inversion, which recovered by discharge.

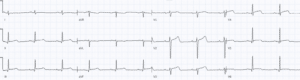
Case 4: primary TTS mimicking inferolateral Occlusion MI
- H: normal sinus rhythm
- E: normal conduction
- A: normal axis
- R: loss of R waves V3-4, Q waves lateral precordial and inferior limb leads
- T: normal voltages
- S: concave ST elevation and hyperacute T waves lateral precordial and inferior limb leads, with reciprocal T wave inversion in aVL
Impression: ECG appearance of inferolateral STEMI(+)OMI. Cath lab activated: normal coronaries, apical ballooning without thrombus, troponin 21,000. Postcath ECG had precordial and inferior T wave inversion with long QT, and discharge ECG had normalization of ECG changes.
Case 5: stroke secondary to TTS, after STEMI and aortic dissection ruled out
- H: sinus bradycardia
- E: normal intervals
- A: left axis from LAFB
- R: loss of precordial R waves
- T: normal voltages
- S: convex ST elevation lateral and inferior
Impression: ECG appearance of inferolateral STEMI(+)OMI in patient with stroke. Stat CT head showed MCA stroke, then angiogram showed normal normal coronaries with no aortic dissection. Echo showed EF 35%, apical akinesis with thrombus, which normalized on follow up echo a few weeks later. Discharge ECG had resolution of Q waves and ST segments, but little T wave inversion
Case 6: wraparound LAD occlusion with reperfusion T wave inversion
- H: sinus rhythm
- E: short PR, other intervals normal
- A: normal axis
- R: loss of precordial R waves
- T: normal voltages
- S: precordial and inferior convex ST elevation with terminal T wave inversion
Impression: wraparound LAD occlusion with some reperfusion. Initially referred to cardiology as myocarditis because of widespread ST changes, but this is diagnosis of exclusion. Cath lab activated: 70% LAD occlusion, akinetic apex with thrombus, first troponin 3000ng/L and peak 5000. Discharge ECG had resolution of ST elevation, deepening of reperfusion T wave inversion with normal QT

Case 7: giant T wave inversion secondary to apical hypertrophic cardiomyopathy
- Heart rate/rhythm: sinus bradycardia
- Electrical conduction: normal intervals
- Axis: normal
- R-wave: normal progression
- Tall/small voltages: LVH with large voltages in apical distribution
- ST/T: T wave inversion across precordial and inferior leads, secondary to LVH and proportional to voltages
Impression: large apical voltages with secondary T wave inversion and normal QT. Echo showed apical hypertrophic cardiomyopathy
Case 8: proximal LAD reperfusion (Wellens)
- H: normal sinus with PAC
- E: normal conduction
- A: normal axis
- R: normal R wave progression
- T: normal voltages
- S: primary T wave inversion anterolateral, with reciprocal tall T in III
Impression: proximal LAD reperfusion (Wellen’s syndrome). Angiogram: 85% LAD occlusion, peak trop 200ng/L, and discharge ECG the same
Case 9: acute RV strain from PE
- H: normal sinus rhythm
- E: prolong QT
- A: normal axis but S wave in I
- R: delayed R wave progression
- T: normal voltages
- ST: primary antero-inferior TWI
Impression: acute RV strain. CT showed large PE
Case 10: secondary TTS with classic deep T waves and long QT
- H: borderline sinus bradycardia
- E: long QT
- A: normal axis
- R: normal R wave progression
- T: low voltages limb leads
- S: diffuse T wave inversion, deep in anterior leads
Impression: diffuse T wave inversion and QT prolongation phase of TTS, with apical ballooning on echo. Peak trop 500ng/L. Admitted for thyrotoxicosis. Angiogram found only mild coronary artery disease. Subsequent ECGs had even deeper T wave inversion and even long QT, which improved by discharge.

Take home points for this ECG Cases on Takotsubo Syndrome
- Takotsubo Syndrome is usually triggered by an emotional or physical stress leading to acute catecholaminergic myocardial stunning
- The initial ST elevation phase of Takotsubo Syndrome mimics Occlusion MI, can’t be distinguished by patient factors or POCUS findings, and requires immediate angiogram
- The subsequent phase of Takotsubo Syndrome has T wave inversion in apical distribution, which can mimic reperfusion but often has very deep T wave inversion and very long QT interval
- Antero-inferior T wave inversion can also be seen in apical hypertrophic cardiomyopathy, pulmonary embolism, or wraparound/distal LAD reperfusion
- Takotsubo Syndrome is a retrospective diagnosis of exclusion—with an angiogram ruling out occlusion, a ventriculogram showing apical ballooning, and a follow up echo showing recovery of LV function.
- Complications of Takotsubo Syndrome include LV failure, apical thrombus, and polymorphic VT from long QT
References for ECG Cases 35 – ECG Approach to Takotsubo Syndrome
- Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a position statement from the task force on Takotsubo syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2016;18:8-27
- Dias A, Nunez Gil IJ, Santoro F, et al. Takotsubo syndrome: state-of-the-art review by an expert panel – Part 1. Cardiovasc Revasc Med 2019 Jan;20(1):70-79
- Ghadri JR, Wittstein IS, Prasad A, et al. International expert consensus document on takotubo syndrome (Part I): clinical, characteristics, diagnostic criteria, and pathophysiology. Eur Heart J 2018;39:2032-46
- Ghadri JR, Wittstein IS, Prasad A, et al. International expert consensus document on takotubo syndrome (Part II): clinical, characteristics, diagnostic criteria, and pathophysiology. Eur Heart J 2018;39:2047-62
- Namgung J. Electrocardiographic findings in Takotsubo cardiomyopathy: ECG evolution and its difference from the ECG of acute coronary syndrome. Clin Med Insights Cardiol 2014;8:29-34
- Haider A, Bengs S, Luu J, et al. Sex and gender differences in cardiovascular medicine: presentation and outcomes of acute coronary syndrome. Eur Heart J 2020 Apr;41(13):1328-1336
- Veaat FE, Christensen TE, Smeijers L, et al. Is it possible to differentiate between Takotsubo cardiomyopathy and acute anterior ST-elevation myocardial infarction? J of Electrocardiol 2015 Jul-Aug;48(4):512-519
- Duran-Cambra A, Sutil-Vega M, Fiol M, et al. Systematic review of the electrocardiographic changes in the Takotsubo syndrome. Ann Noninvasive Electrocardiol 2015 Jan;20(1):1-6
- Kosuge M, Ebina T, HIbi K, et al. Differences in negative T waves among acute coronary syndrome, acute pulmonary embolism, and Takotsubo cardiomyopathy. Eur Heart J Acute Cardiovasc Care 2012 Dec;1(4):349-357
- Chhabra L, Butt N, Ahmad SA, et al. Electrocardiographic changes in Takotsubo cardiomyopathy. J of Electrocardiol 2021 Mar-Apr;65:28-33



Leave A Comment