
Topics in this EM Quick Hits podcast
Anand Swaminathan on LAST prevention, recognition and management (0:54)
Emily Austin on sodium nitrite suicide kit poisoning, methemoglobinemia and methylene blue (10:51)
Hans & Erin Rosenberg on post-intubation analgesia and sedation (17:29)
Salim Rezaie on short-term tetracaine for corneal abrasions new evidence (25:58)
Jesse MacLaren on differentiating ST deviation in occlusion MI from other causes (33:03)
Robert Maunder on a 3 step approach to coping and building resilience during the COVID pandemic (40:52 )
Podcast: Play in new window | Download (Duration: 52:01 — 47.7MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Anand Swaminathan, Hans Rosenberg and Anton Helman
Cite this podcast as: Helman, A. Swaminathan, Austin, E. M. Rosenberg, H. Rezaie, S. MacLaren, J. Maunder, R. EM Quick Hits 26 – LAST, Sodium Nitrite Poisoning, Post-intubation Care, Tetracaine for Corneal Abrasion, ST depression, Coping with COVID. Emergency Medicine Cases. February, 2021. https://emergencymedicinecases.com/em-quick-hits-february-2021/. Accessed [date].
LAST prevention, recognition and management
- LAST (Local Anesthetic Systemic Toxicity) is an iatrogenic life-threatening acute neurologic/cardiac adverse reaction resulting from infiltration of local anesthetic that enters the systemic circulation
- The best treatment is prevention! Preventative measures include aspirating before injection of anesthetic to ensure that the needle is not in a blood vessel and using less than the toxic dose of the anesthetic (see table below)
- Consider LAST in any patient coming from outpatient surgical center in cardiac arrest
- Initial symptoms/signs include perioral numbness and other paresthesias, tinnitus, muscle fasciculations, hypertension, tachycardia progressing to tonic-clonic seizures, decreased LOA, apnea, hypotension, bradycardia, dysrhythmias and cardiac arrest
- Neurologic symptoms typically precede cardiovascular symptoms in lidocaine toxicity while cardiovascular symptoms typically present first in bupivacaine toxicity
- Treatment in addition to withdrawal of anesthetic and usual CABs may include epinephrine, bicarb, lipid emulsion therapy

Local anesthetic maximum doses adapted from Core EM

- Schwartz DR, Kaufman B. Local Anesthetics. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e New York, NY: McGraw-Hill; 2015.
- Neal JM et al, American Society of Regional Anesthesia and Pain Medicine. American Society of Regional Anesthesia and Pain Medicine checklist for managing local anesthetic systemic toxicity: 2012 version. Reg Anesth Pain Med 2012;37:16–8.
- Cao D et al. Intravenous lipid emulsion in the emergency department: a systematic review. J Emerg Med 2015; 48(3): 387-97.
Sodium Nitrite suicide kit poisoning, methemoglobinemia and methylene blue
- Sodium nitrite (a yellow-white crystalline powder food preservative/additive) “suicide kits” can be purchased online resulting in ED presentations with massive overdose
- Sodium nitrite causes toxicity through smooth muscle relaxation resulting in vasodilalatory shock and by producing methemoglobin, shifting the oxygen-Hb dissociation curve to the left resulting in cyanosis, low oxygen saturation despite maintained respiratory status and chocolate brown coloured blood
- Workup includes co-oximetry for methemoglobin on a VBG or AGB; methemoglobin is normally <1.5% in healthy individuals; >10% methemoglobin results in cyanosis, >20% results in headache, dizziness, nausea and >50% results in tissue ischemia with seizures, dysrhythmias, acidosis
- For intentional suicide attempts of sodium nitrite suggested dosing is IV Methylene blue 2mg/kg push, repeated if methemoglobin level has not decreased at 15 minutes to a maximum of 7mg/kg and consideration for red cell or exchange transfusions
- Durão C, Pedrosa F, Dinis-Oliveira RJ. A fatal case by a suicide kit containing sodium nitrite ordered on the internet. J Forensic Leg Med. 2020 Jul;73:101989. doi: 10.1016/j.jflm.2020.101989. Epub 2020 Jun 2.
- Dean, D.E., Looman, K.B. and Topmiller, R.G. (2021), Fatal methemoglobinemia in three suicidal sodium nitrite poisonings. J Forensic Sci. https://doi.org/10.1111/1556-4029.14689
- Katabami, K., Hayakawa, M., & Gando, S. (2016). Severe Methemoglobinemia due to sodium nitrite poisoning. Case Reports in Emergency Medicine, 2016, 1-3. https://doi.org/10.1155/2016/9013816
Post-intubation sedation and analgesia
- Under-treatment or over-treatment of pain and agitation of the post-intubation patient in the ED may increase the likelihood of the patient developing acute delirium, which has been associated with an increased mortality rate in ICU patients suffering from severe sepsis or septic shock and may prolong ICU stay
- For patients who are aggressively attempting to pull out their ETT and require immediate sedation and analgesia, consider Ketamine 0.7mg/kg IV (approx. 50mg IV), then 0.15-0.25mg/kg q5-10 mins prn titrated to effect.
- Benzodiazepines may increase the incidence of delirium and prolong the time on the ventilator, and so are not favored as a first line for sedation; if you choose to use benzodiazepines, be sure to control pain first with fentanyl before any benzodiazepine is administered, and use small doses (eg: 1-2mg Midazolam)
![]() Update 2022: A secondary analysis of the SPICE-III (Sedation Practice in Intensive Care Evaluation) open label RCT found that patients under the age of 65 sedated with dexmedetomidine and propofol combination had increased mortality with increasing dexmedetomidine dose, whereas increasing the dose of propofol was associated with decreased adjusted 90-day mortality. Abstract
Update 2022: A secondary analysis of the SPICE-III (Sedation Practice in Intensive Care Evaluation) open label RCT found that patients under the age of 65 sedated with dexmedetomidine and propofol combination had increased mortality with increasing dexmedetomidine dose, whereas increasing the dose of propofol was associated with decreased adjusted 90-day mortality. Abstract

With permission Canadian Journal of Emergency Medicine
Episode 55: Fluids in Sepsis, Post-intubation Analgesia and Sedation
- Rosenberg H, Hendin A, Rosenberg E. Just the Facts: Postintubation sedation in the emergency department. CJEM. 2020 Nov;22(6):764-767.
Short term topical tetracaine for corneal abrasions
- A 2020 single center, prospective RCT of 111 adults with uncomplicated corneal abrasions who all received Polymyxin B sulfate/trimethoprim sulfate 2 drops q4hrs and Percocet 1-2 q6h prn for breakthrough pain, were randomized to topical tetracaine 0.5% 1 drop q30min prn x24hr vs artificial tear solution 1 drop q30min prn x24hrs
- Topical 0.5% tetracaine significantly reduced pain scores at 24 to 48 hours and was opioid sparing for breakthrough pain compared to placebo
- No significant difference in harms
- Larger trials are required to assess for rare adverse events such as corneal scarring, ulceration, perforation etc.
- Ensure follow-up, short-term use, and return precautions in these patients to avoid long-term use of these medications
REBELEM Corneal Abrasions and Short Term Topical Tetricaine
Journal Jam 6 – Outpatient Topical Anesthetics for Corneal Abrasions
- Shipman S, Painter K, Keuchel M, Bogie C. Short-Term Topical Tetracaine Is Highly Efficacious for the Treatment of Pain Caused by Corneal Abrasions: A Double-Blind, Randomized Clinical Trial. Ann Emerg Med. 2020 Oct 27:S0196-0644(20)30739-3. doi: 10.1016/j.annemergmed.2020.08.036. Epub ahead of print.
- Erdem E, Undar IH, Esen E, Yar K, Yagmur M, Ersoz R. Topical anesthetic eye drops abuse: are we aware of the danger? Cutan Ocul Toxicol. 2013 Sep;32(3):189-93. doi: 10.3109/15569527.2012.744758. Epub 2013 Feb 15.
- Puls HA, Cabrera D, Murad MH, Erwin PJ, Bellolio MF. Safety and Effectiveness of Topical Anesthetics in Corneal Abrasions: Systematic Review and Meta-Analysis. J Emerg Med. 2015;49(5):816-24.
- Ball IM, Seabrook J, Desai N, Allen L, Anderson S. Dilute proparacaine for the management of acute corneal injuries in the emergency department. CJEM. 2010;12(5):389-96.
- Waldman N, Densie IK, Herbison P. Topical tetracaine used for 24 hours is safe and rated highly effective by patients for the treatment of pain caused by corneal abrasions: a double-blind, randomized clinical trial. Acad Emerg Med. 2014;21(4):374-82.Calder LA, et al. Topical Nonsteroidal Anti-Inflammatory Drugs for Corneal Abrasions: Meta-analysis of Randomized Trials. Academic Emergency Medicine 12(5) 2005.
Differentiating ST segment deviation of occlusion MI from other causes
- Interpret ST segments in context of the preceding Q wave and T wave that follows to help differentiate ST deviation as are result of LBBB, RBBB, LVH, pericarditis, hyperkalemia, hypokalemia, early repolarization from occlusion MI where ST deviation is often preceded by Q waves (or loss of R waves), followed by hyperacute or inverted T waves
- Look for the presence and reciprocity of ST elevation and depression as well as Q and T wave changes in the reciprocal leads, understanding however, that reciprocal changes may not be present, for example, in mid/distal LAD occlusion
For examples of this approach and the differential diagnosis of ST elevation and depression visit ECG Cases:
ECG Cases 17 ST Elevations Mnemonic & Occlusion MI
ECG Cases 18 ST Depressed Mnemonic & Occlusion MI
- Pollehn T, Brady WJ, Perron AD, et al. The electrocardiographic differential diagnosis of ST segment depression. Emerg Med J 2002 Mar;19(2):129-35.
- Phibbs B, Nelson W. Differential classification of acute myocardial infarction into ST- and non-ST segment elevation is not valid or rational. Ann of Noninvas Electrocardiol 30 June 2010,15(3):191-99.
- Meyers HP, Bracey A, Lee D, et al. Comparison of the ST-elevation myocardial infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs NOMI paradigms of acute MI. J of Emerg Med 2020 Dec 8;S0736-4679(20)31070-2.
- Miranda DF, Lobo AS, Walsh B, et al. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergency department. Can J Cardiol 2018 Feb;34(2): 132-145
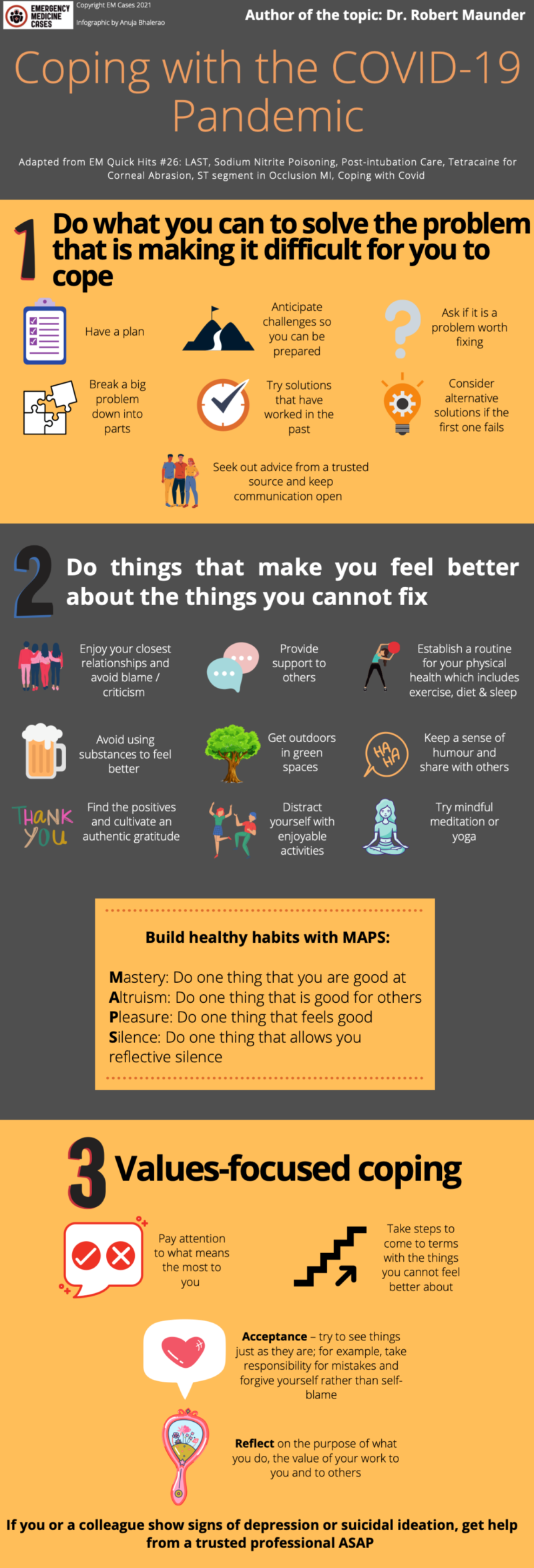
3 step approach to coping and building resilience during the COVID pandemic
- Do what you can to solve the problem: have a plan/strategy, anticipate challenges so you can be prepared, make sure it is a problem worth fixing, break a big problem down into parts, try solutions that have worked in the past, consider alternative solutions if the first one fails, seek out advice from a trusted source/person/team and keep communication open/respectful/clear
- Do things that make you feel better about the things you cannot fix:
- find support in your personal relationships, enjoy/maintain/repair your closest relationships, accept support, take advantage of enjoyable times with others, avoid blame and criticism (being right is often not as important being connected),
- provide support to others which feels good,
- establish a routine for your physical health (exercise/diet/sleep),
- avoid using substances to feel better even if your stress makes you feel like you deserve it,
- get outdoors in green spaces often as doing this reduces stress,
- keep a sense of humour and share it with others,
- find the honest positives and cultivate authentic gratitude,
- distract yourself with enjoyable activities,
- for some, mindful meditation/yoga may help if you can invest the time, but they are not for everyone
- Build healthy habits with MAPS: Matstery, Altruism, Pleasure, Silence so that everyday you: do one thing that you are good at, one thing that is good for others, one thing that feels good, and one thing that allows you reflective silence
- Meaning/values-focused coping: pay attention to what means the most to you and take steps to come to terms with the things you cannot feel better about
- Acceptance – try to see things just as they are; for example take responsibility for mistakes and forgive yourself rather than self-blame
- Reflect on the purpose of what you do, the value of your work to you and to others
If you or a colleague show signs of depression/suicidal ideation get help from a trusted professional ASAP
None of the authors have any conflicts of interest to declare
Ep 198 Understanding and Improving Culture in Emergency Medicine: Key Insights
Ep 103 Preventing Burnout and Promoting Wellness in Emergency Medicine
View Larger Image



It seems that even with opiates pain relief with corneal ulceration was poor .
Does not padding and testing of the eye with chloramphenicol ointment produce relief by the ointment protecting nerve fibres from pain .
Lousy placebo .