
Topics in this EM Quick Hits podcast
Anand Swaminathan on GI balloon tamponade preparation and indications (1:30)
Jesse McLaren on why troponin is rarely useful in SVT (8:45)
Christina Shenvi on why we should not use the term “mechanical fall” in older patients (15:25)
Nour Khatib & Jonathan Wallace on rural vertical vertigo case (25:24)
Reuben Strayer on VAFEI – Video-Assisted Flexible Endoscopic Intubation (32:56)
Podcast: Play in new window | Download (Duration: 43:05 — 39.5MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Reuben Strayer & Anton Helman
Cite this podcast as: Helman, A. Swaminathan, A. McLaren, J. Shenvi, C. Khatib, N. Wallace, J. Strayer, R. EM Quick Hits 40 – GI Balloon Tamponade, SVT and Troponin, Falls in Older Patients, Vertical Vertigo, VAFEI Airway. July, 2022. https://emergencymedicinecases.com/em-quick-hits-july-2022/. Accessed August 5, 2026.
GI balloon tamponade preparation and indications
- Employ mental preparation with deliberate practice well before the procedure
- If your ED does not have a GI balloon tamponade kit with all the necessary gear, consider getting involved in creating one for your ED
- Airway control is usually necessary before placing the GI balloon
- Potential indications for placing GI balloon tamponade before the patient decompensates include:
- Recurrent hemodynamic instability
- Activation of massive transfusion
- Recurrent or active hematemesis
- Delay to endoscopy
Overview of Linton, Blakemore and Minnesota GI tube video
Placement of Blakemore tube video
Placement of Minnesota tube video
Placement of Linton tube video
- Bridwell RE, Long B, Ramzy M, Gottlieb M. Balloon Tamponade for the Management of Gastrointestinal Bleeding. J Emerg Med. 2022 Apr;62(4):545-558.
- Morgenstern, J. Balloon tamponade of GI bleeding, First10EM, May 23, 2016. Available at:
https://doi.org/10.51684/FIRS.2147
Is there any value in troponin for SVT?
- Evidence suggests that troponin testing in patients with paroxysmal SVT who present to the ED with an episode of SVT does not improve outcomes and may increase length of stay, admission rates and increase potentially harmful downstream testing
- The palpitations and chest pain in patients with SVT are rarely symptoms of ACS
- ST depression in multiple ECG leads is common in SVT and is thought to be rate related/demand ischemia unless it persists after cardioversion; when the ST depression resolves after cardioversion this confirms the diagnosis of SVT and essentially rules out ACS as a cause of ST depression
- The pathophysiology of SVT is sufficient to explain a bump in troponin without the presence of CAD
- The prognosis of SVT is not significantly changed with an elevated troponin level compared to a normal troponin level
 Update 2024: A systematic review and meta-analysis of 7 studies (500 patients) found that troponin elevation is common in ED patients with SVT (pooled prevalence 46%), while overall MACE was uncommon (6%). Among patients with elevated troponin, the pooled prevalence of MACE was 11%, suggesting that troponin elevation is common in SVT but has limited prognostic value for identifying patients at risk of adverse outcomes. Abstract
Update 2024: A systematic review and meta-analysis of 7 studies (500 patients) found that troponin elevation is common in ED patients with SVT (pooled prevalence 46%), while overall MACE was uncommon (6%). Among patients with elevated troponin, the pooled prevalence of MACE was 11%, suggesting that troponin elevation is common in SVT but has limited prognostic value for identifying patients at risk of adverse outcomes. Abstract
- Allen R, deSouza IS. Troponin Testing in Patients With Supraventricular Tachycardia—Are We Overtesting? A Teachable Moment. JAMA Intern Med. 2021;181(6):842–843.
- Ben Yedder N, Roux JF, Paredes FA. Troponin elevation in supraventricular tachycardia: primary dependence on heart rate. Can J Cardiol. 2011 Jan-Feb;27(1):105-9. doi: 10.1016/j.cjca.2010.12.004.
- Chow GV, Hirsch GA, Spragg DD, Cai JX, Cheng A, Ziegelstein RC, Marine JE. Prognostic significance of cardiac troponin I levels in hospitalized patients presenting with supraventricular tachycardia. Medicine (Baltimore). 2010 May;89(3):141-148.
- Ghersin I, Zahran M, Azzam ZS, Suleiman M, Bahouth F. Prognostic value of cardiac troponin levels in patients presenting with supraventricular tachycardias. J Electrocardiol. 2020 Sep-Oct;62:200-203.
- Carlberg DJ, Tsuchitani S, Barlotta KS, Brady WJ. Serum troponin testing in patients with paroxysmal supraventricular tachycardia: outcome after ED care. Am J Emerg Med. 2011 Jun;29(5):545-8.
Why should we abandon the term “mechanical fall” in older patients
- Falls are the leading cause of trauma related admissions and mortality in older adults
- One approach to falls in older patients is to consider what happened before, during and after the fall which will help assess for acute medical illnesses and injuries as a result of the fall
- After ruling out acute medical events related to falls (eg. stroke, syncope, seizure, volume depletion, GI bleed etc), rather than attributing falls in older patients to whatever mechanical stimulus that might have been present at the time of the fall, it behooves the ED doc to identify and address the potential long standing underlying causes/falls risk factors such as: polypharmacy, cognitive impairment, visual/hearing deficits, postural hypotension, poor muscular tone, to help prevent future falls
- Consider referrals to physiotherapy/occupational therapy, geriatric medicine for further assessment of the above issues
- A gait test (there are multiple validated ones such as ‘Timed up and go‘) is essential in older patients who present to the ED after a fall to help in disposition decisions
- The term “mechanical fall” minimizes the importance of addressing the contributing factors to falls in older adults; consider, instead, “multi-factorial ground level fall” or “non-syncopal fall”
- Goldberg EM, Marks SJ, Ilegbusi A, Resnik L, Strauss DH, Merchant RC. GAPcare: The Geriatric Acute and Post-Acute Fall Prevention Intervention in the Emergency Department: Preliminary Data. J Am Geriatr Soc. 2020 Jan;68(1):198-206. doi: 10.1111/jgs.16210. Epub 2019 Oct 17.
- Goldberg EM, Marks SJ, Resnik LJ, Long S, Mellott H, Merchant RC. 2020. Can an Emergency Department–Initiated Intervention Prevent Subsequent Falls and Health Care Use in Older Adults? A Randomized Controlled Trial. Annals of Emergency Medicine. 76(6):739–750.
Can vertical vertigo be from a peripheral cause?
- Vertical vertigo (patient reports their visual environment moving in the vertical plane) and nystagmus have traditionally been associated with a central cause of vertigo, however vertical vertigo may have a peripheral cause such as BPPV of the posterior canal
Dr. Walter Himmel’s summary of vertigo talk from EMU 2017
- Ibekwe TS, Rogers C. Clinical evaluation of posterior canal benign paroxysmal positional vertigo. Niger Med J. 2012 Apr;53(2):94-101.
- Ohle R et al. Can Emergency Physicians Accurately Rule Out a Central Cause of Vertigo Using the HINTS Examination? A Systematic Review and Meta-analysis. AEM 2020.
VAFEI – Video-Assisted Flexible Endoscopic Intubation
- Video-assisted flexible endoscopic intubation is a powerful two-operator airway technique that will allow relatively straightforward intubation of patients with very difficult anatomy by taking advantage of the strengths of video laryngoscopy and flexible endoscopy while diminishing their drawbacks
- VAFEI can be incorporated into a breathing intubation approach such as topicalized awake or ketamine only but can also be performed quickly enough to be used with paralysis and RSI
- Especially useful when combined with hyperangulated geometry blades
- Consider VAFEI in the patient with challenging anatomy and as a rescue technique when video laryngoscope (VL) has failed due to difficulty with tube delivery
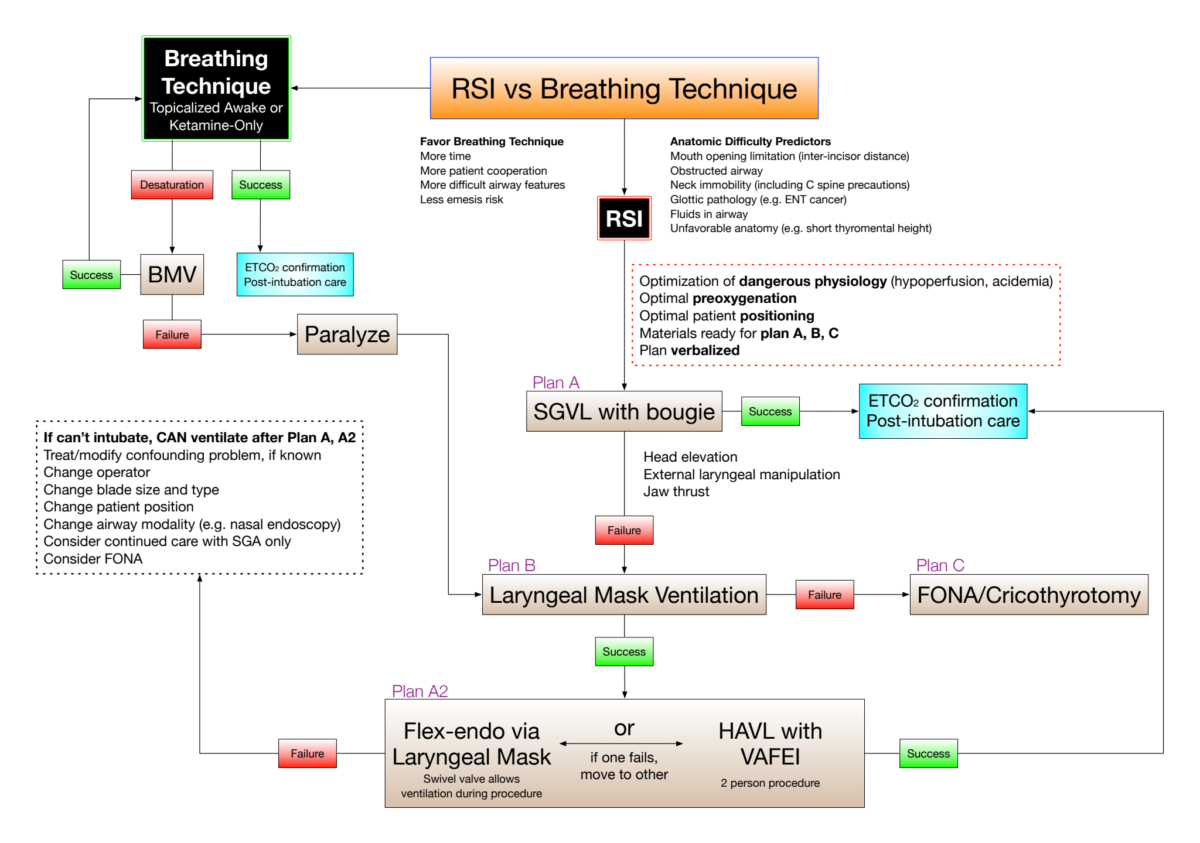
Six Steps of VAFEI:
- VL operator performs laryngoscopy as usual to obtain an adequate view (or, if difficult anatomy prevents an adequate view, obtain best possible view)
- VL operator, maintaining the laryngoscope position with their left hand, readies suction in right hand, in preparation for flexible endoscopy
- Flexible endoscopy operator looks in mouth, places the endoscope in the patient’s mouth and advances the endoscope to the end of the VL blade under direct visualization
- Endoscope operator looks at VL screen to guide the endoscope to the vocal cords and advances the scope through the cords, usually looking at the VL screen but, occasionally, if really difficult anatomy, the VL screen view may be inadequate, in which case the scope can be guided to and through the cords while looking at the flexible endoscope screen
- Once the scope is through the cords, the endoscopy operator looks at the endoscope screen to advance the scope down to above the carina
- Endoscopist or an assistant railroads the preloaded ETT to just above the carina, at which point the endoscope is removed, the ETT is attached to ventilation with capnography to confirm placement
- Mazzinari G, Rovira L, Henao L, Ortega J, Casasempere A, Fernandez Y, Acosta M, Belaouchi M, Esparza-Miñana JM. Effect of Dynamic Versus Stylet-Guided Intubation on First-Attempt Success in Difficult Airways Undergoing Glidescope Laryngoscopy: A Randomized Controlled Trial. Anesth Analg. 2019 Jun;128(6):1264-1271. doi: 10.1213/ANE.0000000000004102. Erratum in: Anesth Analg. 2019 Oct;129(4):e141.
- Airway Choices in the Era of Many Choices from EM Updates https://emupdates.com/choices/
None of the authors have any conflicts of interest to declare



Thanks for Nour Khatib and Jonathan Wallace for bringing up a vertigo case in the rural setting.
Some points I’d like to make.
It’s great that Jonathan realized that dizziness described as light-headedness can still be caused by a vestibular disorder,and doesn’t necessarily mean a pre-syncope kind of differential.
Patients with BPPV often endorse having a baseline of lesser dizziness/lightheadedness/not quite right feeling between the paroxysmal attacks.
The patient’s dizziness came on with looking up, very typical with posterior canal BPPV, which is the commonest form of BPPV seen. But mostly commonly they describe it coming on when getting in, out, or turning over in bed.
Headache is not typical for BPPV, but it sounds incidental in this case. If a new significant and persistent headache was accompanied by new persistent vertigo, and difficulty with gait, this would be concerning for posterior circulation stroke.
If the patient had a history of migraine headaches, and had 5 or more episodes of dizziness over a period of weeks/months/years and had either headache/photophobia/phonophobia/visual blurring or flashing lights associated with half the episodes of dizziness, then vestibular migraine is the most likely diagnosis. And it can seem very positional in nature also.
Although horizontal nystagmus is most commonly cause by horizontal canal BPPV, or vestibular neuritis affecting the horizontal canal, it can also occur in stroke.
Although Jonathan did look for nystagmus at rest, which is great because it is often not done or charted on dizzy patients, so well done! He also noted the patient could sit upright. But a gait assessment was not mentioned. This is a very important thing in the dizzy patient. Almost all patients with a non-serious cause for their vertigo can walk unaided, but stroke patients may not be able to.
Jonathan also correctly noted that HINTS exam was not applicable, because the patient was no longer symptomatic. Again, well done, but also you should not perform the HINTS exam on patients without nystagmus at rest.
The patient described mild subjective nystagmus when the right side was tested with the Dix-Hallpike test. There is a thing called “subjective BPPV” where the patient has all the features of BPPV, including a latency of few seconds before the patient complains of dizziness in the Dix-Hallpike test. In my experience, this is fairly rare. It’s probably important to not have the patient look at anything particular during the Dix-Hallpike test, as fixation on any object will tend to lessen or completely supress peripheral nystagmus from BPPV.
It’s also a good idea to repeat the Dix-hallpike test, and ensure you get the patient from sitting to lying down with neck extended 20 degree all in about 2 seconds. You may see nystagmus the second time.
In any case, this certainly could have been a case of subjective posterior canal BPPV.
Posterior canal BPPV is the most common variant of BPPV. I’ve spent decades trying to get ED docs to understand this that seeing vertical nystagmus is a good thing during the Dix-Hallpike test. Here is a 10 min long video I made about this topic. https://youtu.be/V4C_BRNf1EI
And here is another video showing you multiple positive Dix-Hallpike tests
https://youtu.be/88dPK4_8kj8
I agree no imaging is necessary for cases of BPPV, but posterior canal BPPV is the easiest variant to cure with the Epley maneuver.
https://youtu.be/kvVnEsGVLUY
Horizontal canal is much more common than we used to think. Probably 20-30% of all cases of BPPV in the ED.
https://youtu.be/VRjRTnIw9YE
Anterior is fairly rare (2-5% of all BPPV). But if you see a case of what sounds exactly like BPPV and see vertical downward nystagmus, it’s worth trying to cure it. If you can’t cure it, make sure you refer the patient for reassessment.
https://youtu.be/2TAYDp3vVTU
TIA can mimic BPPV rarely. But then again, you won’t see the typical nystagmus of posterior canal BPPV.
Thanks again to Nour and Jonathan for this interesting case.
Peter Johns
https://www.youtube.com/c/PeterJohns/videos