

In Part 1 of this Episode on Acute Coronary Syndromes Risk Stratification Dr. Eric Letovksy, Dr. Mark Mensour and Dr. Neil Fam discuss common pearls and pitfalls in assessing the patient who presents to the ED with chest pain. They review atypical presentations to look out for, what the literature says about the value of traditional and non-traditional cardiac risk factors, the diagnostic utility of recent cardiac testing, and which patients in the ED should have a cardiac work-up. Finally, in the ED work up of Acute Coronary Syndromes Risk Stratification, they highlight some valuable key points in ECG interpretation and how best to use and interpret cardiac biomarkers like troponin.
Drs. Letovksy, Mensour & Fam address questions like: How useful are the traditional cardiac risk factors in predicting ACS in the ED? How does a negative recent treadmill stress test, nuclear stress test or angiogram effect the pre-test probability of ACS in the ED? What does recent evidence tell us about the assumption that patients presenting with chest pain and a presumed new LBBB will rule in for MI and require re-perfusion therapy? How can we diagnose MI in the patient with a ventricular pacemaker? What is the difference between Troponin I and Troponin T from a practical clinical perspective? Is one Troponin ever good enough to rule out MI in the patient with a normal ECG? Should we be using a 2hr delta troponin protocol? How will the new ultra-sensitive Troponins change our practice? and many more…..
Podcast: Play in new window | Download (Duration: 1:04:09 — 51.4MB)
Subscribe: Apple Podcasts
Written Summary and blog post by Lucas Chartier, edited by Anton Helman June 2011
Cite this podcast as: Letovsky, E, Mensour, M, Fam, N, Helman, A. Part 1: Acute Coronary Syndromes Risk Stratification. Emergency Medicine Cases. June, 2011. https://emergencymedicinecases.com/episode-15-p1-acute-coronary-syndromes-risk-stratification/. Accessed [date].
Go to part 2 of this 2-part podcast on acute coronary syndromes
ACUTE CORONARY SYNDROMES RISK STRATIFICATION
Canadian AMI miss rate is 0.8-8% depending on practice location
ED differential diagnosis for immediately life-threatening causes of CP: ACS, PE, pericarditis with tamponade, tension pneumothorax, aortic dissection, esophageal rupture (Boerhaave’s Syndrome)
Atypical Presentations of Acute Coronary Syndromes
- 1/3 of pts with ACS have no CP and risk factors for No CP: elderly, women, DM, Hx of CVA or CHF
- Most frequent anginal equivalents: SOB>weakness>unusual fatigue>sweats>dizziness
- Therefore, elderly & diabetic pts with SOB should get ECG within lOmin of arrival in ED just like CP pts
- Associated symptoms most predictive of MI: ED observed sweating>vomiting>radiation to both arms>radiation to R arm
- Radiation to the left arm did not increase the likelihood of MI in recent study in Resuscitation, 2010
- 7% of patients with ACS will have pleuritic chest pain & 7% of patients with ACS have their pain partially or fully reproduced on chest wall palpation
Conclusion: “Atypical is Typical ” ie. Atypical presentations of ACS are common
Diagnostic Value of ED Medications for Acute Coronary Syndromes
- ‘Pink Lady’ (Maalox & Lidocaine mixture) improving chest pain has no predictive value in ACS
- GERD is the most common misdiagnosis of missed MI (20% of patients describe their pain as “burning” or “heartburn” , 8% of MI begin while eating, and 15% of pts with MI will respond to ‘Pink Lady’)
- Response to Nitroglycerin has no predictive value in ACS
ACS Risk Factors
- In the ED, traditional cardiac risk factors are poor predictors of ACS in patients >40y/o: the only traditional risk factors that predict ACS in the ED patient with CP are DM & Family History of premature MI in male patients (not obesity, smoking, hypertension, hyperlipidemia)
- Patients < 40y/o in whom the absence of all traditional risk factors makes the pre-test probability of ACS very low and the presence of >4 risk factors, does help predict ACS
- Important Non-traditional Risk Factors (esp in young patients): Pregnancy, CRF, HIV (esp if on protease inhibitors), Cocaine/Amphetamine use, chronic steroid use, Lupus (50x risk from Framingham data)
Diagnostic Utility of Recent Cardiac Testing for ED Patients with Chest Pain
- Up to 2/3 of AMIs caused by stenotic plaques <50% occlusive, so that tests based on stenosis can be misleading
- Treadmill stress test has only 68% sensitivity and 77% specificity for single vessel disease
- A recent “negative” angiogram does not rule out ACS in the ED patient
Value of Physical Examination in Chest Pain Patients
- Exclude other diagnoses
- pulse deficit, new aortic regurg murmur and neuro deficit in aortic dissection
- unilateral decreased air entry and JVD in tension pneumothorax
- friction rub, muffled heart sound and JVD in pericarditis with tamponade
- Prognostication
- look for signs of AHF (JVD, HJR, S3, crackles and peripheral edema) as worse prognosis
- aortic stenosis murmur (critical AS with ischemia carries very poor prognosis)
- new mitral regurg murmur (ominous sign of papillary muscle rupture/flail leaflet)
For updated podcast on chest pain risk stratification go to Episode 64 in which Chris Hicks explains the HEART Score
![]() Update 2017: The HEART score is a useful way to risk stratify patients with chest pain, but effect on health care resources is limited due to lack of adherence to management recommendations. Abstract
Update 2017: The HEART score is a useful way to risk stratify patients with chest pain, but effect on health care resources is limited due to lack of adherence to management recommendations. Abstract
ACS ECG Pearls from our experts
- 7% of pts with MI will have a normal ECG & 1/3 of pts with MI will have ‘non-specific changes’
- Elderly patients more likely to have LBBB, LVH and non-diagnostic ECG
Indications for 15 lead ECG: All inferior STEMI to rule out RV infarct, ST depression in V1/V2 with or without tall R wave in V1 to rule out Posterior MI
- Some experts extend indications to any pts with non-specific changes (literature is mixed)
Differentiating the ECG of Pericarditis from AMI: ST elevation Lead ll > Lead lll in pericarditis and vice versa in MI, diffuse concave (as apposed to convex in MI) STE without reciprocal changes, PR depression in lead ll + V6 and PR elevation in aVR, maintain T wave morphology (as apposed obliteration of T wave morphology in ACS), ST elevation in Lead l and Lead ll at the same time
![]() Update 2016: Inferior ST segment elevation with ST segment depression in aVL suggests STEMI as opposed to pericarditis. Abstract
Update 2016: Inferior ST segment elevation with ST segment depression in aVL suggests STEMI as opposed to pericarditis. Abstract
![]() Update 2021: A retrospective case-control study of 808 patients with suspected ACS demonstrated that pre-defined occlusive MI (OMI) ECG criteria may be superior to the current STEMI ECG criteria for the diagnosis of OMI. Full text
Update 2021: A retrospective case-control study of 808 patients with suspected ACS demonstrated that pre-defined occlusive MI (OMI) ECG criteria may be superior to the current STEMI ECG criteria for the diagnosis of OMI. Full text
LBBB & Acute Coronary Syndromes
- New LBBB in the setting of a good clinical story for MI is an indication for re-perfusion therapy according to the AHA guidelines, however only 1/3 of these pts will rule in for MI, and only a small minority of patients will fulfill Sgarbosa’s criteria making the diagnosis of MI more likely
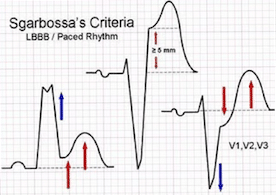
Sgarbosa’s criteria (see image below) that make MI more likely in the setting of LBBB and Ventricular-Paced Rhythm
- STE 1mm or more and concordant (in the same direction as the main deflection) with the QRS
- STD 1mm or more in leads V1 V2 or V3
- STE 5mm or more and discordant (in the opposite direction) with the QRS complex
Pearl: New RBBB has worse prognosis than new LBBB in the setting of ACS
New vs old LBBB: Patients with CP or CP equivalent and new LBBB or old LBBB have same rate of MI (Am Heart J. 2011;161(4):698-704)
For Amal Mattu’s review of LBBB in MI go to Episode 45
aVR ST Elevation
- STE in aVR > STE in V1 with ST diffuse ST depression in other leads suggests Left Main or Triple Vessel Disease in the setting of ACS which carries a poor prognosis
- Also consider pulmonary embolism, WPW in CP patients with STE in aVR
- While STE in aVR is not part of most STEMI protocols for transfer for immediate PCI, our exp
 erts believe that pts with STE in aVR and ACS should be considered very high risk and transferred immediately for PCI via a STEMI protocol
erts believe that pts with STE in aVR and ACS should be considered very high risk and transferred immediately for PCI via a STEMI protocol
Right Ventricular Infarction
- Clinical diagnosis: triad of elevated JVP, clear chest and low BP + 15 lead shows V4R elevation on ECG
- Preload dependent, so avoid nitrates, morphine and B-blockers and consider fluid bolus
Cardiac Biomarkers
- 2 sets of Troponins (6-8hrs apart) are indicated for all patients (except those that have isolated CP >12hrs prior to ED visit and are symptom free for 12hrs prior to their ED visit, who only need 1 Troponin)
- Always repeat a detectable Troponin leak even if below the cut-off level for MI
- New 4th generation ultra-sensitive Troponins turn positive sooner than older Troponins and a 3hr & 6hr post CP ultra-sensitive Troponin has a near 100% sensitivity to rule out MI in low risk patients, however they are less specific than the traditional Troponins (N Engl J Med. 2009;361(9):913-5)
- Troponin levels reflect increased risk of death/MI regardless of renal dysfunction (N Engl J Med 2002; 346:2047-2052)
- Adverse outcomes increase with increased Troponin even at values below the cut-off regardless of cause
- Differential of elevated Troponin: PE, myocarditis, sepsis, post-cardioversion, CHF, RF
![]() Update 2021: Prospective, observational cohort study of non-traumatic chest pain (without ST-elevation myocardial infarction), involved paramedics obtaining blood sample that is sent for troponin measurement. EMS blood samples resulted in mean potential reduction of length of stay by 72.5 +/- SD 35.7 minutes and appeared safe from a diagnostic performance perspective. Abstract
Update 2021: Prospective, observational cohort study of non-traumatic chest pain (without ST-elevation myocardial infarction), involved paramedics obtaining blood sample that is sent for troponin measurement. EMS blood samples resulted in mean potential reduction of length of stay by 72.5 +/- SD 35.7 minutes and appeared safe from a diagnostic performance perspective. Abstract
For more on acute coronary syndromes on EM Cases:
Episode 15 Part 2: Acute Coronary Syndromes Management
Best Case Ever 1 Is Thrombolysis Better Than PCI for STEMI?
Best Case Ever 4 Acute Coronary Syndrome From Venous Source
Journal Jam 5 One Hour Troponin to Rule Out and In MI
Key References
Body R, Carley S, Wibberley C, Mcdowell G, Ferguson J, Mackway-jones K. The value of symptoms and signs in the emergent diagnosis of acute coronary syndromes. Resuscitation. 2010;81(3):281-6.
Hockberger RS, Walls RM. Rosen’s Emergency Medicine – Concepts and Clinical Practice, 2-Volume Set,Expert Consult Premium Edition – Enhanced Online Features and Print,7, Rosen’s Emergency Medicine – Concepts and Clinical Practice, 2-Volume Set. Elsevier Health Sciences; 2009.
Tintinalli J, Stapczynski J, Ma OJ et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition (Book and DVD). Mcgraw-hill; 2010.
Kontos MC, et al. Outcomes in patients with chronicity of left bundle-branch block with possible acute myocardial infarction. Am Heart J. 2011;161(4):698-704.
Aviles RJ, Troponin T levels in patients with acute coronary syndromes, with or without renal dysfunction. N Engl J Med. 2002;346(26):2047-52.
Morrow DA. Clinical application of sensitive troponin assays. N Engl J Med. 2009;361(9):913-5.



We need a case of chest pain and and how I can manage it at ER