

In this bonus EM Cases podcast, The Stiell Sessions 2 – Update in Atrial Fibrillation, we have Dr. Ian Stiell discussing an update in Atrial Fibrillation 2014 management including the age-old question of rate control vs rhythm control, the new CHADS-65 algorithm for oral anticogulant therapy, the need to initiate anticoagulant therapy in the ED, the more aggressive use of the Ottawa Aggressive Protocol, the dangers of attempting to cardiovert unstable patients who are in permanent Atrial Fibrillation, the new 150 rule to help determine the likelihood of successful cardioversion and much more.
Podcast: Play in new window | Download (Duration: 29:39 — 27.2MB)
Subscribe: Apple Podcasts
Published December 2014
Cite this podcast as: Helman, A, Stiell, I. The Stiell Sessions 2 – Update in Atrial Fibrillation 2014. Emergency Medicine Cases. December, 2014. https://emergencymedicinecases.com/episode-57-stiell-sessions-2-update-atrial-fibrillation-2014/. Accessed [date].
Link to Episode 20 on Atrial Fibrillation with Dr. Clare Atzema, Nazanin Meshkat & Bryan Au on the pearls, pitfalls, ins and outs of Atrial Fibrillation to 2012.
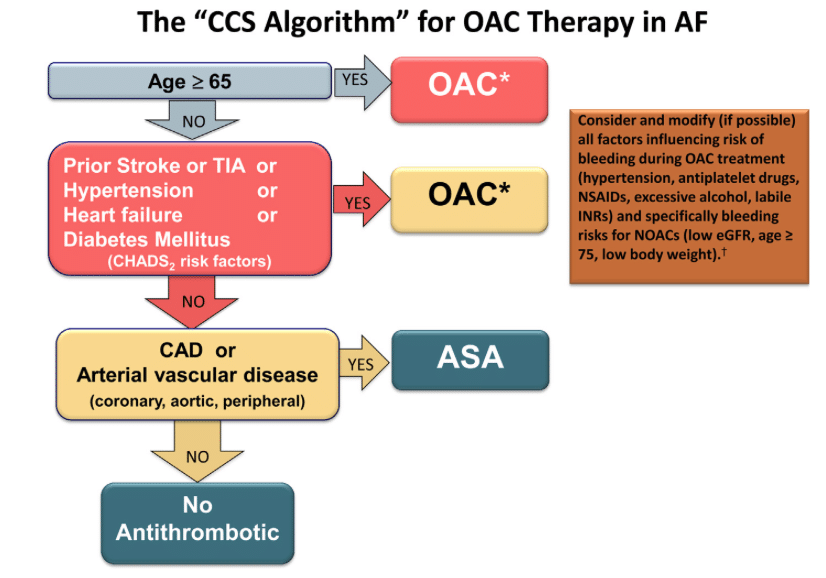
Dr. Stiell’s blog post on the Canadian Cardiovascular Society CHADS-65 Risk Stratification Algorithm
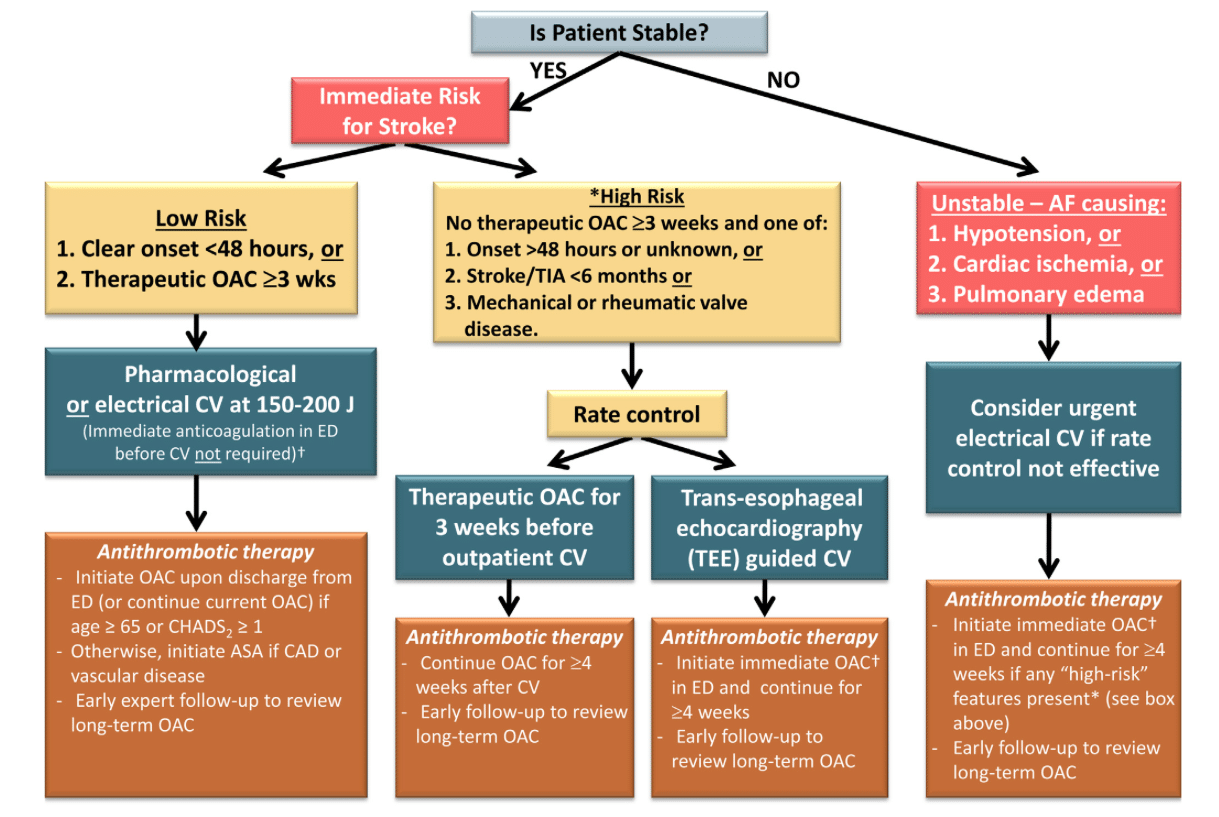
Dr. Stiell’s blog post on ED Treatment Algorithm for Anticoagulants in Atrial Fibrillation
Dr. Stiell’s blog post on Unstable Patients with Atrial Fibrillation
Canadian Atrial Fibrillation Guidelines 2014 Full PDF
American Heart Association Atrial Fibrillation Guidelines 2014 Full PDF
AFFIRM trial on rate control vs rhythm control
JACC Finnish study on Thromboembolic Complication After Cardioversion of Acute Atrial Fibrillation that challenges the 48 hour safety rule
The Ottawa Aggressive Protocol for cardioversion of Atrial Fibrillation with Procainamide
![]() Update 2015: A viewpoint article in the Canadian Journal of Cardiology by Stiell et al. on the safety of urgent cardioversion in recent onset atrial fibrillation and flutter, in light of the Finnish study. Abstract
Update 2015: A viewpoint article in the Canadian Journal of Cardiology by Stiell et al. on the safety of urgent cardioversion in recent onset atrial fibrillation and flutter, in light of the Finnish study. Abstract
![]() Update 2015: Study in Annals of Emergency Medicine suggests that patients given a prescription for warfarin in the ED may have better rates of long-term anti-coagulation. Abstract
Update 2015: Study in Annals of Emergency Medicine suggests that patients given a prescription for warfarin in the ED may have better rates of long-term anti-coagulation. Abstract
![]() Update 2015: Patients with atrial fibrillation or flutter and an acute underlying medical illness may not benefit from rate or rhythm control. Article
Update 2015: Patients with atrial fibrillation or flutter and an acute underlying medical illness may not benefit from rate or rhythm control. Article
![]() Update 2015: A 30-day mortality clinical decision instrument for patients who present to the ED with AFib. Abstract
Update 2015: A 30-day mortality clinical decision instrument for patients who present to the ED with AFib. Abstract
For Clare Atzema’s Best Case Ever on Atrial Fibrillation go to Best Case Ever 7
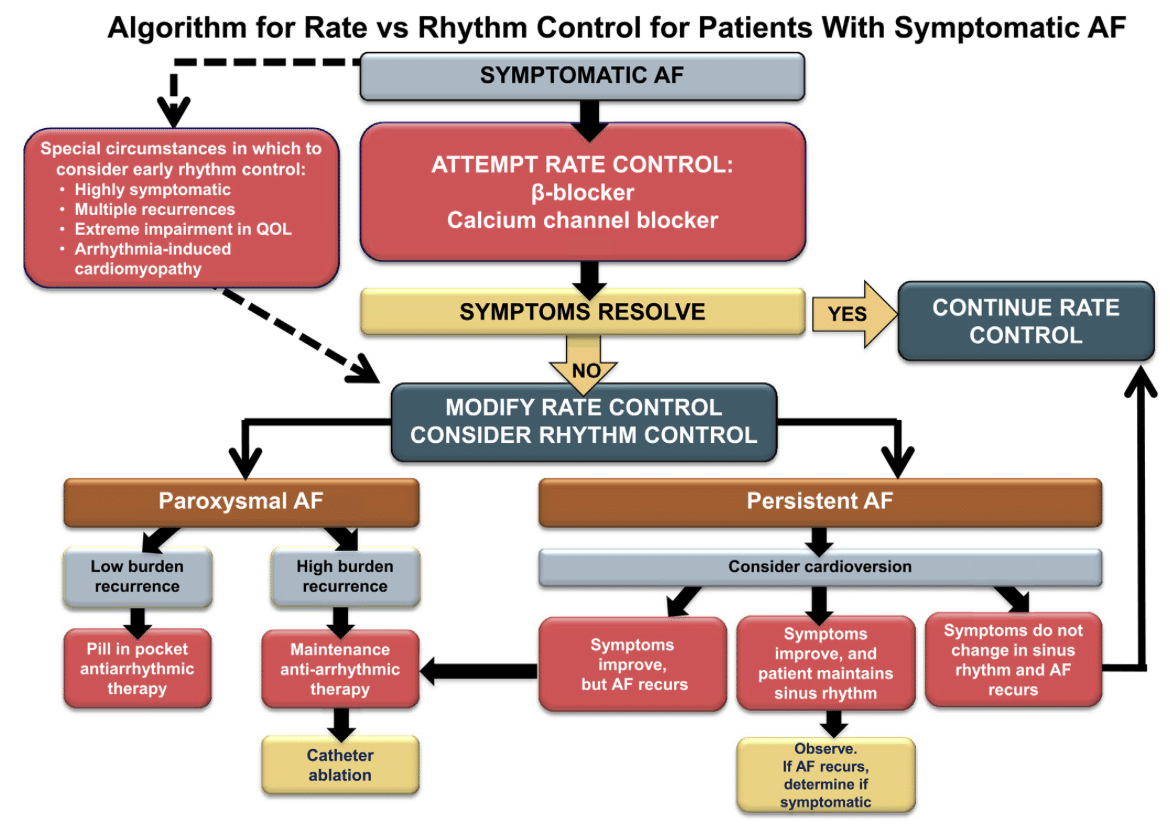
2014 Atrial Fibrillation Algorithms – Canadian Guidelines
![]() For more on atrial fibrillation on EM Cases:
For more on atrial fibrillation on EM Cases:
Episode 20: Atrial Fibrillation
Best Case Ever 7: Atrial Fibrillation
Key Reference
Verma, A et al. 2014 Focused Update of the Canadian Cardiovascular Society Guidelines for the Management of Atrial Fibrillation. Canadian Journal of Cardiology. 30(2014):114-1130. Full PDF
Other References
Stiell IG, Clement CM, Perry JJ, Vaillancourt C, Symington C, Dickinson GE et al. An aggressive protocol for rapid management and discharge of emergency department patients with recent-onset episodes of atrial fibrillation and flutter. Can J Emerg Med 2010; 12(3):181-191.
Airaksinen, J et al. Thrombolembolic Complications After Cardioversion of Acute Atrial Fibrillation. The FinCV (Finnish CardioVersion) Study. J Am Coll Cardiol. 2013;62(13):1187-1192
Wyse, D. et al. A Comparison of Rate Control and Rhythm Control in Patients with Atrial Fibrillation. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. N Engl J Med 2002;347:1825-1833.
January, C. et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64(21):2246-2280.
Dr. Helman and Dr. Stiell have no conflicts of interest to disclose except that Dr. Stiell is funded by the Ottawa Research Institute for his research



[…] discussion of everything you need to know about AFib from EM Cases featuring Ian Stiell. […]
[…] Emergency medicine cases podcast summary of above […]
[…] Please note: The posts on this blog are oriented towards critically ill patients who develop AF as a complication of their critical illness. If you’re looking for information about outpatients who presents to the ED with AF as their primary problem, look at other FOAM resources e.g. ERCastand EMCases. […]