
This is EM Cases Episode 104 – Emergency Management of Intracerebral Hemorrhage – The Golden Hour with Scott Weingart and Walter Himmel. With special guest appearances by Rob Simard and Peter Brindley.
There exists a kind of self-fulfilling prognostic pessimism when it comes to ICH. And this pessimism sometimes leads to less than optimal care in patients who otherwise might have had a reasonably good outcome if they were managed aggressively. Despite the poor prognosis of these patients overall, there is some evidence to suggest that early aggressive medical management may improve outcomes. As such, the skill with which you manage your patient with ICH in those first few hours could be the most important determinant of their outcome. In this Golden Hour you have a chance to prevent hematoma expansion, stabilize intracerebral perfusion and give your patient the best chance of survival with neurologic recovery. In this podcast, the Weingart-Himmel Sessions Redux, we answer questions such as: Should we attempt to manage blood pressure before ICH is confirmed on CT? What are the best drugs to manage blood pressure in ICH? What is the role of POCUS in emergency management of intracerebral hemorrhage? How do we best reverse the effects of anticoagulants and lytics in ICH patients? Are prophylactic antiepileptic drugs ever indicated in ICH in the ED? How do we best risk stratify patients with ICH? What are the indications for neurosurgical intervention? How do we determine if a patient with ICH has elevated ICP and how do we best manage it in the ED? What are the key elements of a neuro-critical care intubation? What is the preferred hyperosmolar agent for elevated ICP? and many more…
Podcast: Play in new window | Download (Duration: 1:38:32 — 90.3MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Anton Helman December, 2017
Cite this podcast as: Helman, A, Weingart, S, Himmel, W, Simard, R, Brindley, P. Emergency Management of Intracerebral Hemorrhage – The Golden Hour. Emergency Medicine Cases. December, 2017. https://emergencymedicinecases.com/intracerebral-hemorrhage-golden-hour/. Accessed [date].
Can intracerebral hemorrhage vs ischemic stroke be predicted accurately before CT?
Clinical findings that significantly increase the probability of ICH include altered level of awareness, neck stiffness, seizures, DBP>110, bilateral neurologic findings, vomiting and headache. However, no combination of clinical findings can be absolutely diagnostic.
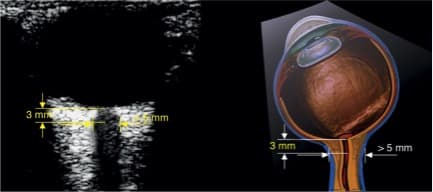
POCUS transcranial doppler and optic nerve sheath diameter may help increase your suspicion for ICH in the setting of abrupt onset neurologic symptoms. Raised ICP is more in keeping with ICH than with ischemic stroke. An optic nerve sheath diameter of >6 mm is highly specific for raised ICP while an optic nerve sheath diameter of <5 mm is highly sensitive for ruling out raised ICP. Transcranial doppler is able to detect both emboli and stenosis of the MCA helping to rule in an ischemic stroke. It can also help predict midline shift from ICH, as well as sometimes identify an ICH lesion. More evidence and experience with transcranial doppler is needed to determine its role in the workup of ICH.
ICH management considerations before CT
Patients with ICH who you deem at risk for aspiration (nausea, retching, vomiting, low GCS, apneic, herniating etc) should be considered for airway control before CT (see airway management below).
![]()
For the patient who presents with stroke symptoms within a few hours of onset, whether you consider them more likely to have ICH vs an ischemic stroke, if SBP is greater than 180, our experts recommend titrating the SBP down to 180 before the diagnosis is confirmed by CT, if time permits.
Differential diagnosis of ICH
While there is a long list of causes of ICH, the most common causes of ICH include hypertension (which tend to cause deep brain basal ganglia, brain stem and cerebellar bleeds) and amyloid angiopathy usually seen in elderly patients (which tend to cause large lobar bleeds).
It is important to identify two other important causes of ICH in the ED, coagulopathy associated ICH and cerebral venous thrombosis, as they require specific time-sensitive treatment.
Learn more about when to consider cerebral venous thrombosis in EM Quick Hits 25 (skip to 00:53)
Imaging considerations in ICH
While many centers will automatically perform plain CT, CT angiogram and perfusion CT for all patients who present to the ED with a clinical picture consistent with stroke, other centers may only perform plain CT in the ED in patients who do not fulfill criteria for a “code stroke” and leave other imaging to be considered by the inpatient team. Our experts recommend that all patients with ICH should receive a CT angiogram in the ED for both diagnostic/therapeutic and risk stratification considerations.
Emergency management of ICH – The Golden Hour
The Big 6 considerations in medical management of ICH in the ED
- BP
- Coagulopathy
- Glucose
- Temperature
- Seizure activity
- ICP
What is the target BP in intracerebral hemorrhage?
Based on the INTERACT2 and ATTACH2 trials our experts suggest that for those patients with ICH with GCS scores >7, lowering BP to 140/80 is not harmful and may be minimally beneficial.
The INTERACT2 trial of 2013 was an RCT of 2839 patients with spontaneous ICH within 6 hours and elevated systolic BP, who were randomized to intensive treatment (<140) vs guideline-recommended therapy (<180). Outcomes were modified Rankin scale of 3-6 (death and major disability) at 90 days. They found no significant different in primary outcomes. Note that this was an ordinal analysis with it’s inherent problems.
The ATTACH-2 RCT compared a lower systolic BP target of 110 to 139 mm Hg with a standard target of 140 – 179 in 1,000 patients using IV labetolol, diltiazem or urapidil. Patients were eligible if they had at least one episode of SBP > 180 mm Hg between symptom onset and 4.5 hours. The trial was stopped early for futility, with no difference in the primary outcome of death or disability (intensive group 38.7% vs control 37.7%). There was also no difference in haematoma expansion (18.9% vs 24.4%) or treatment-related serious adverse events. This trial was criticized for being underpowered.
Hypotension (MAP <75-80) should be avoided at all costs in patients with ICH.
The antihypertensive agents of choice in ICH are nicardipine or labetolol
Nicardipine is the antihypertensive agent of choice in ICH because it does not affect the ionotropy of the heart, and being a pure arterial vasodilator it has no significant effect on cerebral vasodilatation or venous dilatation.
Dosing nicardipine in ICH: Start nicardipine at 5mg/hr and increase q5min by 2.5mg until the target blood pressure is achieved and then immediately titrate down to maintenance infusion of 3mg/hr.
For centers without nicardipine available, labetolol is the antihypertensive agent of choice in ICH.
Dosing labetolol in ICH: Start with labetolol 20mg over 1-2 minutes and then 20mg q3-5 mins until target blood pressure is achieved and then start an infusion of 1-8mg/min.
Learn more about blood pressure management in intracranial hemorrhage in Episode 41: Hypertensive Emergencies
Platelet transfusion trigger for thrombocytopenia in ICH
The absolute indication for platelet transfusion in patients with ICH is a platelet count <50,000.
However, most hematologists and neurosurgeons recommend platelet transfusion for ICH with a platelet count <100,000 despite the lack of evidence for improved outcomes, especially if the patient requires emergency surgery.
Is there any benefit of platelet transfusion for patients taking antiplatelet agents in ICH?
While there are some observational studies suggesting potential benefit from platelet transfusion, the PATCH trial of 2016, a multicenter open label RCT in Netherlands, UK and France randomised 190 patients with supratentorial ICH and GCS >8 who had received antiplatelet therapy (mostly ASA alone) within 7 days to standard care vs care with platelet transfusion. An ordinal analysis looking at modified Rankin Score and death showed an odds ratio of death of 2.05 with the treatment group. More serious adverse events were reported in patients who received platelet transfusion (42 %), compared with 29 % in patients who received standard care alone. They concluded that platelets were associated with poorer clinical outcomes overall.
It is important to note that these patients were primarily nonsurgical ICH patients. For patients requiring emergency surgery most neurosurgeons do recommend platelet transfusion for patients taking antiplatelet agents. It is also important to note that patients with subarachnoid hemorrhage or traumatic intracerebral hemorrhage taking antiplatelet agents may require platelet transfusion as well.
Reversal of blood thinners in ICH
Reversal of Warfarin in ICH
Any patient taking Warfarin who presents to the ED with ICH should receive IV 4 factor PCCs 1,500 units (Octaplex, Beriplex or Kcentra) as soon as possible and IV Vitamin K in 50mL of NS over 10 mins before the INR result comes back, as hematoma expansion typically occurs within the first hour in patients taking Warfarin.
The INR should be repeated 15 mins and 5-6 hours after PCCs are administered to assess for repeat dosing if necessary. Target an INR of 1.5.
Current Canadian recommendations for 4 factor PCCs dosing based on INR:
- INR 1.6-3: 1000 units PCC
- INR 3-5: 2000 units PCC
- INR >5: 3000 units PCC
Reversal of Low Molecular Weight Heparin (LMWH) and UFH with protamine sulphate in ICH
For dalteparin: IV protamine sulphate 1mg for every 100 units dalteparin to maximum dose of 50mg over 15 mins
For enoxaparin taken within 8 hrs: IV protamine sulpahate 1mg of every 1 mg enoxaparin to maximum dose of 50mg over 15 mins. For enoxaparin taken 8-12hrs ago, give protamine sulphate 0.5mg per 1mg of enoxaparin (maximum single dose 50mg).
For UFH: IV protamine sulphate 1mg for every 100 units of UFH given in the previous 2-3hrs to a maximum single dose of 50mg). A repeat dose of 0.5mg of protamine per 100 units of UFH may be given if the PTT remains elevated.
2nd line: Factor Vlla
Reversal of dabigitran in ICH
Idarucizumab 5g over 15-20mins is the reversal agent of choice for dabigitran
If idarucizumab is not available consider FEIBA (Factor Eight Inhibiting Bypass Activity)
If FEIBA is not available consider 4 factor PCC (Octaplex, Beriplex or Kcentra)
Reversal of Xa Inhibitors in ICH
For Xa inhibitors (e.g. apixaban, rivaroxaban) 4-factor PCC (Octaplex, Beriplex, Kcentra) at a dose of 50 IU/kg up to 3,000 units is the reversal agent of choice based on limited evidence.
Note that if you highly suspect a Xa inhibitor intracranial bleed before obtaining a CT head, it is reasonable to give 1,500 units of 4 factor PCC on speculation.
Andexanet Alfa is a decoy antigen; it competitively binds rivaroxaban and apixaban and is given as an ongoing infusion. The evidence is not convincing for its effectiveness and it is currently not available in Canada as of this publication date.
Deeper dive – EM Cases DOACs: Bleeding and Reversal
Reversal of thrombolytics in ICH
Time is of the essence. Careful monitoring of your ICH patient should allow rapid identification of post-lytic ICH. Any change in mental status or signs of increasing ICP should trigger an immediate CT scan to look for ICH. The sooner you start treatment, the better.
The most recent guidelines for treatment of post-thrombolytic ICH are the 2016 Neurocritical Care Society & Society of Critical Care Medicine Guidelines for Reversal of Antithrombotics in ICH. Based on limited evidence, they recommend cryoprecipitate (10 units initial dose). If cryoprecipitate is contraindicated or not available in a timely manner, they recommend tranexamic acid 10–15 mg/kg IV over 20 min. However, our experts recommend caution with the use of tranexamic acid for ICH because of concerns of inducing thrombosis. As such it should be used only as a last resort.
It is important to check the fibrinogen level after administration of reversal agents. If the fibrinogen level is < 150 mg/dL, they suggest administration of additional cryoprecipitate.
![]() Update 2018: A randomized placebo-controlled trial involving 2325 adults with ICH from acute stroke, demonstrated no significant difference in functional status at 90- days between those receiving TXA versus placebo, though there was a reduction in early deaths and adverse events in the TXA group. (TICH-2 trial) Abstract
Update 2018: A randomized placebo-controlled trial involving 2325 adults with ICH from acute stroke, demonstrated no significant difference in functional status at 90- days between those receiving TXA versus placebo, though there was a reduction in early deaths and adverse events in the TXA group. (TICH-2 trial) Abstract
Glucose control in ICH
Hyperglycemia is common in patients presenting with ICH. Hyperglycemia is associated with poor outcomes (hematoma expansion, increased edema, death, or severe disability). The optimal glucose level and the best hyperglycemia management strategy remain to be elucidated. However, both hypoglycemia (<70 mg/dl or < 3.9 mmol/L) and hyperglycemia (>180 mg/dl or 10 mmol/L) should be avoided. A study suggested improved clinical outcomes with tight control of blood sugar to the range of 80–110 mg, but this was found to cause occasional hypoglycemia resulting in increased mortality.
Bottom line: do not treat glucose between 4 and 10 mmol/L.
Temperature control in ICH
So called ‘brain blood fever‘ is common in ICH with 30- 50 % of patients developing fever. The presence of intraventricular hemorrhage is the main risk factor for fever. Fever is independently associated with poor outcomes in ICH with the duration of fever varying inversely with the patient outcome. While there are no available data from RCTs addressing the role of induced normothermia after ICH, current recommendations are to cool febrile ICH patients to a core temperature below 37.5-38 °C.
Bottom line: avoid fever in ICH.
Is there a role for seizure prophylaxis in ICH?
The short answer is no.
About 10-15% of patients will have a seizure with most of those occurring in the first 24hrs, so very possibly in your ED on your watch. Lobar hemorrhages are at particular risk of causing seizures. Prophylactic anticonvulsants are associated with worse clinical outcomes such as modified Rankin Score 1 and 4 months. However, if the patient is comatose “out of proportion” to CT head findings, consider EEG monitoring to pick up subclinical seizures.
![]() Update 2022: A double blind, randomized, placebo controlled trial with 50 patients with mild-to-moderate severity intracerebral hemorrhage found that fewer electrographic seizures were observed in patients who received levetiracetam compared to placebo in the first 72hrs (levetiracetam 16% vs placebo 43%). Note: All seizures were electrographic and not clinical seizures (seen on EEG only), and this trial was stopped after only recruiting 48% of their target due to low recruitment rate and cessation of funding (PEACH trial). Abstract
Update 2022: A double blind, randomized, placebo controlled trial with 50 patients with mild-to-moderate severity intracerebral hemorrhage found that fewer electrographic seizures were observed in patients who received levetiracetam compared to placebo in the first 72hrs (levetiracetam 16% vs placebo 43%). Note: All seizures were electrographic and not clinical seizures (seen on EEG only), and this trial was stopped after only recruiting 48% of their target due to low recruitment rate and cessation of funding (PEACH trial). Abstract
Management of elevated intracranial pressure (ICP) in intracerebral hemorrhage
ED ICP management strategies include:
- Head of the bed elevation between 30 and 45° with the head kept midline
- Appropriate analgesia and sedation
- Normocapneic ventilation or hyperventilation if herniating
- Hypertonic solutions (e.g. hypertonic saline or mannitol)
Airway considerations in ICH: The Neuroprotective Intubation
First divide patients into two categories:
1. Those that require immediate airway protection: herniating, apneic, very low GCS, soiled airway
2. Those that are slowly declining whom you deem candidates for airway protection
For those patients in category one, perform a standard RSI.
For those patients in category two, perform a neurocritical care protective intubation.
Ensure good neurologic exam before paralyzing the patient if time permits.
1. Get equipment to bedside
2. Keep head of bed elevated at least 20 degrees throughout to prevent spike in ICP
3. Have nicardipine or labetolol as well as push dose epinephrine ready at the bedside to manage any extreme deviations in BP
4. Titrate SBP to 140-160 preferably with an arterial line in place
5. Consider fentanyl 3-5micrograms/kg pretreatment 3 minutes before intubation (beware apnea)
6. Etomidate or Ketofol (in a 25% ketamine, 75% propofol mixture) for induction
7. Rocuromium or succinylcholine
8. Post intubation analgesia should start with fentanyl if you haven’t given already and for sedation use propofol or dexmetatomidine
9. Ventilation: Lung protective ventilation 7mL/kg, +/- lowest PEEP to achieve O2sat 95%, normocapnea at PaCO2 of about 40 unless herniating (target PaCO2 30-35 or ETCO2 27-30 if herniating).
Avoid hypoxemia in ICH at all costs
Learn more about post- intubation analgesia and sedation in EM Cases Episode 55
Hyperosmolar Therapy for suspected raised ICP or brain herniation
Based on ICP monitoring, POCUS optic nerve sheath diameter >6mm or clear signs on CT of elevated ICP (not for low GCS alone) consider hypertonic saline, mannitol or sodium bicarbonate.
Hypertonic saline 3% 250mL over 10 minutes is preferred by our experts because there are less concerns with ![]() sodium derangement and changes in hemodynamics.
sodium derangement and changes in hemodynamics.
If you use mannitol it is advisable to place a bladder catheter and match urinary losses with normal saline administration to avoid hypotension.
A simple way to give mannitol to maximize efficiency and decrease cognitive load is to give one big bag (500mL containing 100g as a 20% solution) for a big patient or one small bag (250mL containing 50g as a 20% solution) for a small person. This roughly estimates the 0.5-1g/kg dose that is recommended.
Note that a meta-analysis by Burgess et al (2016) found no difference in outcomes between hypertonic saline and mannitol in traumatic brain injury.
Learn more in CritCases 8 Management of Elevated ICP
Algorithm for diagnosing ICP elevation with ocular ultrasound
Prognostication: What are the predictors of poor outcome in ICH?
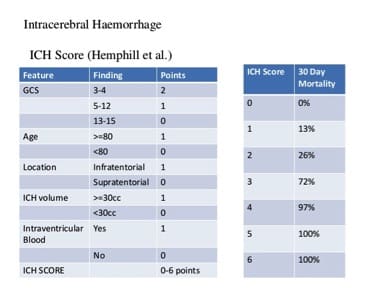
While a high ICH score of 5 or 6 predicts a 100% 30 day mortality at a population level, early prognostication for individual patients is often challenging and difficult to predict. Withdrawal of care should generally not be decided in the ED.
The hematoma volume can be estimated by the following equation: ABC/2 formula
Volume of Hemorrhage = A × B × C × Slices / Hemorrhage Shape
A = Length
B = Width
C = Slice width (# slices with hemorrhage present)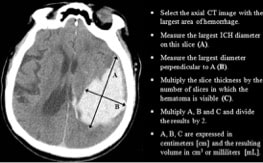
The two most important predictors of early deterioration are hematoma volume and intraventricular hemorrhage.
The spot sign on contrast CT represents contrast extravasation and is an independent predictor of hematoma expansion, functional outcome and mortality. Patients with a spot sign on CT may benefit from more aggressive treatment to reduce hematoma expansion, improve functional outcome and decrease mortality.
Calculate the ICH score at MDCalc
The indications for surgery in ICH are controversial
Surgical intervention in ICH is indicated for all posterior fossa bleeds except those patients with GCS of 14-15 and small hematomas <3cm to prevent acute hydrocephalus and brainstem herniation. Intraventricular hemorrhage requires an intraventricular drain.
For supratentorial bleeds without intraventricular hemorrhage the indications for surgical intervention are controversial and need to be considered on a patient by patient basis. The literature on surgery for supratentorial ICH is summarized here:
The STICH 2 trial randomized patients with superficial lobar hematomas within 1cm of the brain surface with a GCS of 13-15 to early surgery versus medical management with delayed surgery if necessary. Patients with IVH or coma were excluded. They found no difference in mortality or severe disability with early surgery.
The SICHPA trial was a multicenter RCT that compared minimally invasive, stereotactic approaches with low dose tPA for liquefaction and aspiration of clot effective reduction of clot size compared to conservative treatment. They found no differences in 180-day mortality rates.
The MISTIE trials are ongoing. They compare a minimally invasive technique with assistance of low-dose tPA to medical management. Preliminary results of the MISTIE II trial show reduced clots to 50% of the stabilized volume within the first week, compared to a 6% reduction with medical management alone. Significant increases in symptomatic bleeding were not seen with the use of tPA (2.4% in the minimally invasive plus tPA group versus 9.3% in the medical management group), but did increase asymptomatic hemorrhages (22.2% versus 7.1%, p = 0.051).
ICES trial (Intraoperative Stereotactic CT-Guided Endoscopic Surgery) for brain hemorrhage is an RCT with only 20 patients with ICH >20mL volume looking at endoscopic surgery within 48hrs. Forty three percent of surgical patients had functional neurological outcomes defined as a modified Rankin scale score (mRS) of 0–3, compared to 23.7% in the medical management group at 180 and 365 days. Patients with predicted poor prognosis at enrollment (estimated according to a prognostic model taking into account GCS, age, and ICH volumes: 10 x GCS − age − 0.64 x volume) were more likely to have a favorable outcome with early surgery than with initial conservative treatment. Such a benefit with early surgery was not detected in the group of patients with predicted good prognosis at enrollment. In other words, patients with bigger bleeds and lower GCS scores derived the most benefit from surgery. Note that one of the authors received money from the company that manufactures the gear for the procedure.
Suggested checklist for transport of your ICH patient to a neurosurgical center
- Two large bore peripheral IVs with maintanence NS (avoid RL)
- Low threshold to intubate prior to transfer as many patients deteriorate in the first 12hrs, with vent settings addressed; avoid hypoxemia at all costs
- BP approximately 140/80 (consider nicardipine or labetolol infusion)
- Core temperature <37-5-38 °C (consider intra-transport cooling)
- Serum glucose 4-10 mmol/L, frequent finger stick checks, insulin in case >10 mmol/L, D50W in case <4 mmol/L
- Analgesia (fentanyl) and sedation (propofol)
- Lorazepam, phenytoin or levetiracetam in case of seizure
- Hypertonic saline or mannitol as well as increased ventilation in case of herniation
For free CME on ICH go to the ACEP online module based on this podcast
References
De oliveira manoel AL, Goffi A, Zampieri FG, et al. The critical care management of spontaneous intracranial hemorrhage: a contemporary review. Crit Care. 2016;20:272.
Broderick JP, Brott T, Tomsick T, et al. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. J Neurosurg 1993;78(2):188–91.
Stevens RD, Shoykhet M, Cadena R. Emergency neurological life support: intracranial hypertension and herniation. Neurocrit Care. 2015;23 Suppl 2:76–82.
D’andrea A, Conte M, Riegler L, et al. Transcranial Doppler Ultrasound: Incremental Diagnostic Role in Cryptogenic Stroke Part II. J Cardiovasc Echogr. 2016;26(3):71-77.
Schatlo, B Pluta, RM. Clinical applications of transcranial Doppler sonography. Rev Recent Clin Trials. 2007;Jan 2(1): 49-57.
Meyer-Wiethe et al. Diagnosis of ICH with Transcranial ultrasound. Cerbrovasc Dis. 2009;27 Suppl 2:40-7.
Scott Weingart. Podcast 129 – LAMW: The Neurocritical Care Intubation. EMCrit Blog. Published on July 26, 2014.
Scott Weingart. Podcast 78 – Increased Intra-Cranial Pressure (ICP) and Herniation, aka Brain Code. EMCrit Blog. Published on July 22, 2012.
Specogna AV, Turin TC, Patten SB, Hill MD. Factors associated with early deterioration after spontaneous intracerebral hemorrhage: a systematic review and meta-analysis. PLoS One. 2014;9(5):e96743–3. doi:10.1371/journal.pone.0096743.
Hemphill JC 3rd, Greenberg SM, Anderson CS, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2015;46(7):2032–60.
Kate MP, Hansen MB, Mouridsen K, et al. Blood pressure reduction does not reduce perihematoma oxygenation: a CT perfusion study. J Cereb Blood Flow Metab. 2013;34(1):81–6. doi:10.1038/jcbfm.2013.164.
Kothari RU, Brott T, Broderick JP, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996;27(8):1304–5.
Hemphill JC 3rd, Bonovich DC, Besmertis L, et al. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001;32(4):891–7.
Wang CW, Liu YJ, Lee YH, et al. Hematoma shape, hematoma size, Glasgow Coma Scale score and ICH score: which predicts the 30-day mortality better for intracerebral hematoma? PLoS One 2014;9(7):e102326.
Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355-65.
Bourdeaux CP, Brown JM. Randomized controlled trial comparing the effect of 8.4% sodium bicarbonate and 5% sodium chloride on raised intracranial pressure after traumatic brain injury. Neurocrit Care. 2011;15(1):42-5.
Burgess S, Abu-laban RB, Slavik RS, Vu EN, Zed PJ. A Systematic Review of Randomized Controlled Trials Comparing Hypertonic Sodium Solutions and Mannitol for Traumatic Brain Injury: Implications for Emergency Department Management. Ann Pharmacother. 2016;50(4):291-300.
Casaubon LK, Boulanger JM, Blacquiere D, et al. Canadian Stroke Best Practice Recommendations: Hyperacute Stroke Care Guidelines, Update 2015. Int J Stroke. 2015;10(6):924-40.
Qureshi AI, Palesch YY, Barsan WG, et al. Intensive Blood-Pressure Lowering in Patients with Acute Cerebral Hemorrhage. N Engl J Med. 2016;
Raffiz M, Abdullah JM. Optic nerve sheath diameter measurement: a means of detecting raised ICP in adult traumatic and non-traumatic neurosurgical patients. Am J Emerg Med. 2017;35(1):150-153.
Passero S, Ciacci G, Ulivelli M. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Neurology. 2003 Nov 25;61(10):1351-6.
NICE‐SUGAR Study Investigators, Finfer S, Chittock DR, Su SY‐S, Blair D, Foster D, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009 Mar 26;360(13):1283-97.
Frontera JA, Iii JJL, Rabinstein AA, et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit Care. 2016;24(1):6–46. doi:10.1007/s12028-015-0222-x.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology. 2009;72(16):1397–402.
Messé S, Sansing L, Cucchiara B, et al. Prophylactic antiepileptic drug use is associated with poor outcome following ICH. Neurocrit Care. 2009;11(1):38-44.
Frontera JA, Lewin JJ, Rabinstein AA, et al. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: Executive Summary. A Statement for Healthcare Professionals From the Neurocritical Care Society and the Society of Critical Care Medicine. Crit Care Med. 2016;44(12):2251-2257.
Naidech A, Garg R, Liebling S, et al. Anticonvulsant use and outcomes after intracerebral hemorrhage. Stroke. 2009;40(12):3810-3815.
Mendelow AD, Gregson BA, Rowan EN, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet. 2013;382(9890):397–408.
Teernstra OP, Evers SM, Lodder J, Leffers P, Franke CL, Blaauw G. Stereotactic treatment of intracerebral hematoma by means of a plasminogen activator: A multicenter randomized controlled trial (SICHPA). Stroke 2003;34(4):968-974.
Hanley DF, Thompson RE, Muschelli J, et al. Safety and efficacy of minimally invasive surgery plus alteplase in intracerebral haemorrhage evacuation (MISTIE): A randomised, controlled, open-label, phase 2 trial. Lancet Neurol 2016;15(12):1228-1237.
Mould WA, Carhuapoma JR, Muschelli J, et al. Minimally invasive surgery plus recombinant tissue-type plasminogen activator for intracerebral hemorrhage evacuation decreases perihematomal edema. Stroke 2013;44(3):627-634.
Vespa P, Hanley D, Betz J, et al. ICES (intraoperative stereotactic computed tomography guided endoscopic surgery) for brain hemorrhage: A multicenter randomized controlled trial. Stroke 2016;47(11):2749-2755.
Naidech AM, Garg RK, Liebling S, et al. Anticonvulsant use and outcomes after intracerebral hemorrhage. Stroke. 2009;40(12):3810–5.
Kamel H, Navi BB, Nakagawa K, Hemphill JC, Ko NU. Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: a meta‐analysis of randomized clinical trials. Crit Care Med. 2011 Mar;39(3):554-9.
Drs. Helman, Himmel and Weingart have no conflicts of interest to declare
Now test your knowledge with a quiz.



Simple and straightforward approach..super
helpful podcast, written review, outline and reference. Quiz is a great bonus to reinforce/correct. Thanks!
Thank you for this episode+notes. Valuable for students/JMOs.
What about esmolol vs labetalol? Faster onset, shorter half life …