
In this EM Cases Best Case Ever podcast, Dr. Kari Sampsel, Emergency Physician at Ottawa Hospital and Assistant Professor at University of Ottawa, Medical Director of Sexual Assault and Partner Abuse Care Program guides us through an example of a perimortem C-section – a resuscitative hysterotomy at Janus General. She and Rajiv discuss preparation, indications, the procedure, team dynamics and debriefing for this HALO procedure…
Podcast: Play in new window | Download (Duration: 19:31 — 17.9MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Rajiv Thavanathan and Richard Hoang.
Blog post by Anton Helman, June, 2020.
Prepare two resuscitation areas: one for the mother and one for the neonate.
Call obstetrics and pediatrics/NICU for assistance early.
Prepare yourself, your team and your gear.
The indications for perimortem c-section are maternal cardiac arrest with gravid uterus above the umbilicus* or known to be >20 weeks gestational age up to 30 minutes after cardiac arrest started.
*Estimate gestational age by palpating the uterus. If the fundus is above the umbilicus, assume at least 20 weeks gestation.
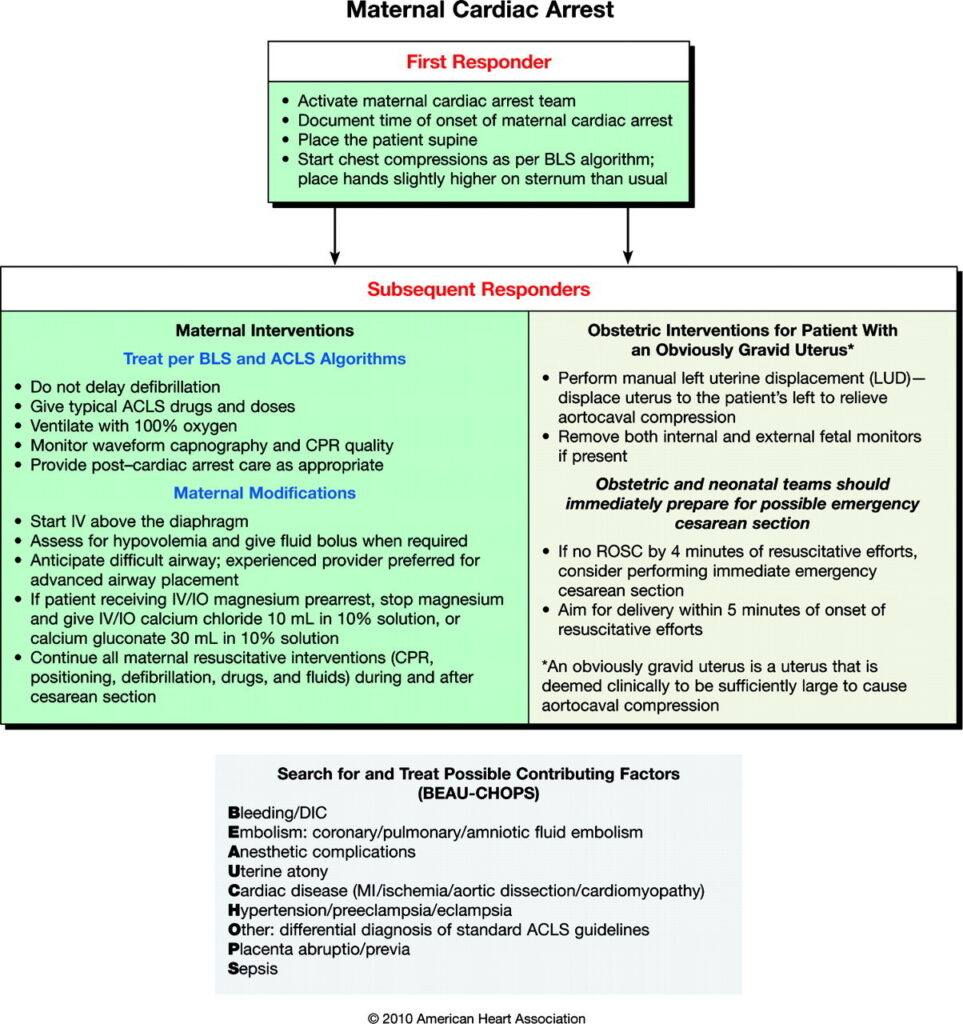
ACLS modifications for maternal resuscitation in perimortem c-section
- Chest compressions 2-3 cm higher on the sternum
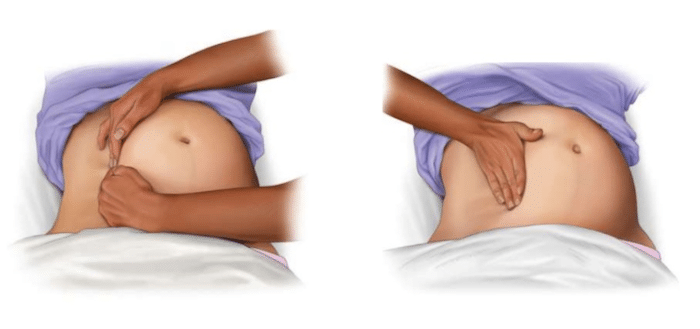
- Manually displace the uterus to the left*
- Avoid femoral lines and obtain IV access above the diaphragm
*To help relieve pressure on the mother’s IVC/aorta the current recommendation is to have the patient lying supine and apply leftwards pressure (rather than the old recommendation to have the patient in 30 degrees left lateral decubitus) to help facilitate high quality chest compressions that may be difficult with the old 30 degree lateral decubitus recommendation:
Excellent summary table of resuscitative hysterotomy by Lauren Westafer of FOAMcast
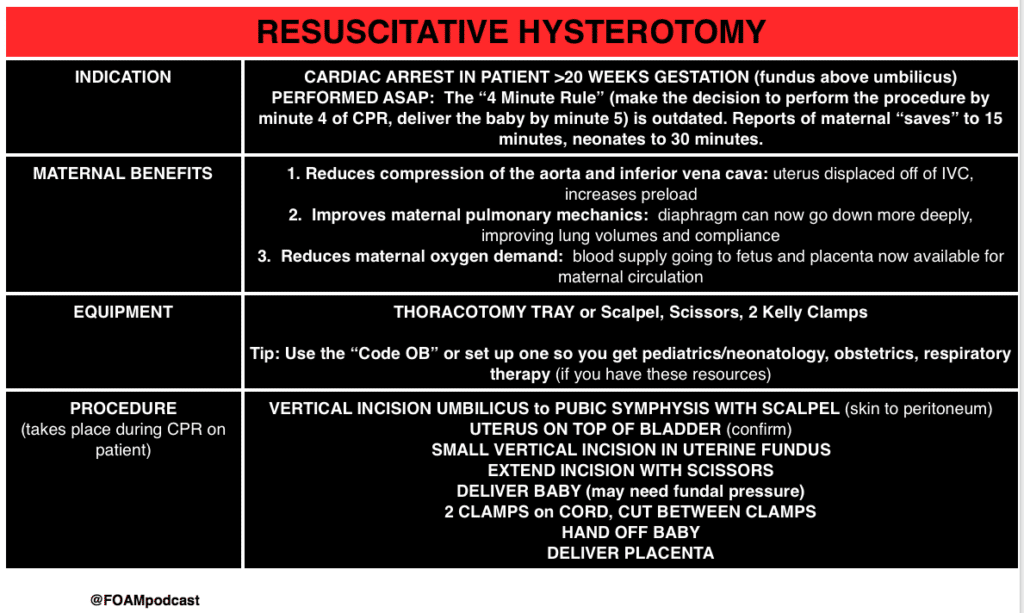
From FOAMcast Episode 60 https://foamcast.org/2016/11/25/episode-60-resuscitative-hysterotomy-first-trimester-emergencies/ (creative commons)
Sara Gray at Essentials of EM on perimortem c-section
Procedural video on perimortem c-section
Pitfall: The most common pitfall in maternal cardiac arrest is delaying the resuscitative hysterotomy. The sooner the procedure is initiated, the more likely maternal and neonatal survival.
References
- Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S829.
- Benson MD, Padovano A, Bourjeily G, Zhou Y. Maternal collapse: Challenging the four-minute rule. EBioMedicine. 2016 Apr;6:253-257.
- Parry R et al. Perimortem caesarean section. Emerg Med J. 2016 Mar;33(3):224-9.
- Healy ME, Kozubal DE, Horn AE, Vilke GM, Chan TC, Ufberg JW. Care of the Critically Ill Pregnant Patient and Perimortem Cesarean Delivery in the Emergency Department. J Emerg Med. 2016;51(2):172-7.
- Stokes N, Kikucki J. Management of Cardiac Arrest in the Pregnant Patient. Curr Treat Options Cardiovasc Med. 2018 Jun 19;20(7):57.
- Campbell, Tabitha A, and Tracy G Sanson. Cardiac Arrest and Pregnancy. Journal of Emergencies, Trauma and Shock. 2009;2(1):34–42.
Other FOAMed Resources on Perimortem C-section
Sara Gray at Essentials of EM on perimortem c-section
Procedural video on perimortem c-section
First10EM on perimortem c-section
EMCrit on perimortem c-section
St. Emlyns on perimortem c-section
Sim Cases series on perimortem c-section on ALiEM



This is great presentation. This happens once in a life time. We should all prepare for this.
If you are skilled ,mother is not responding compressions. You can go throw diaphragm do cardiac massage. Try your luck to save both mother and child
thank you for this post, well described case and excellent literature review.