
In Part 1 of our 2-part series on bradycardia and bradydysrhythmias we discussed a practical approach with electrophysiologist Paul Dorian and EM doc Tarlan Hedayati. In this, part 2, we discuss details of treatment. We answer questions such as: When should pacing be prioritized over medications and vice versa? What are the latest recommendations about dosing of atropine and when is atropine likely to be detrimental? How is the treatment of bradycardia different in the patient with hypothermia? Cardiac ischemia? Myxedema coma? AV nodal blocker overdose? What are the most common pitfalls in utilizing transcutaneous and transvenous pacing? and many more…
Podcast: Play in new window | Download (Duration: 47:32 — 43.5MB)
Subscribe: Apple Podcasts
Podcast production & editing by Anton Helman, sound design by Yuang Chen
Written Summary and blog post by Anton Helman April 2021
Cite this podcast as: Helman, A. Dorian, P. Hedayati, T. Episode 155 Treatment of Bradycardia and Bradydysrhythmias. Emergency Medicine Cases. April, 2021. https://emergencymedicinecases.com/treatment-bradycardia-bradydysrhythmias. Accessed [date]
Go to part 1 of this 2-part podcast on bradycardia and bradydysrhythmias
Suggested Treatment Algorithm for Crashing Bradycardic Patient Without an Obvious Cause
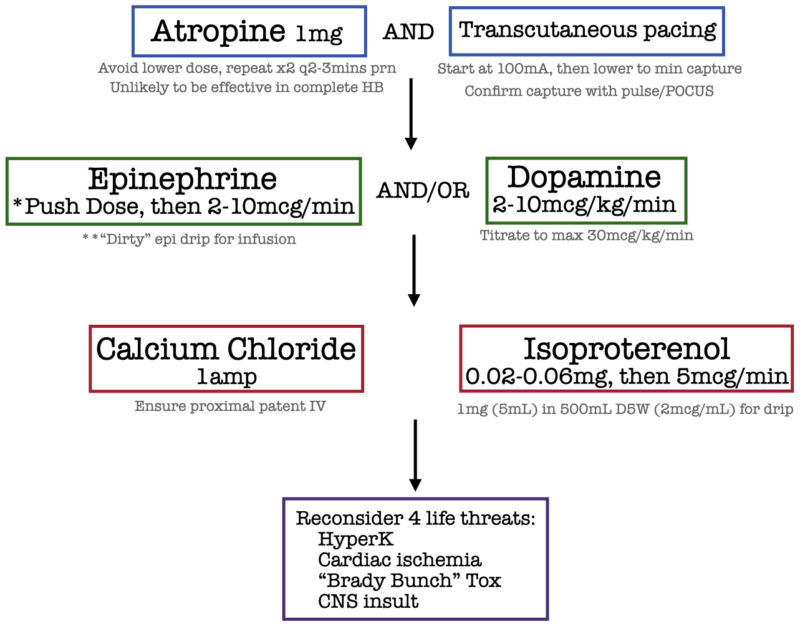
- For the crashing patient administer drugs/fluids and start transcutaneous pacing simultaneously
- There is a paucity of randomized trials for medications to treat bradycardia; these recommendations are based on the ACLS guidelines, weak observational data and expert opinion
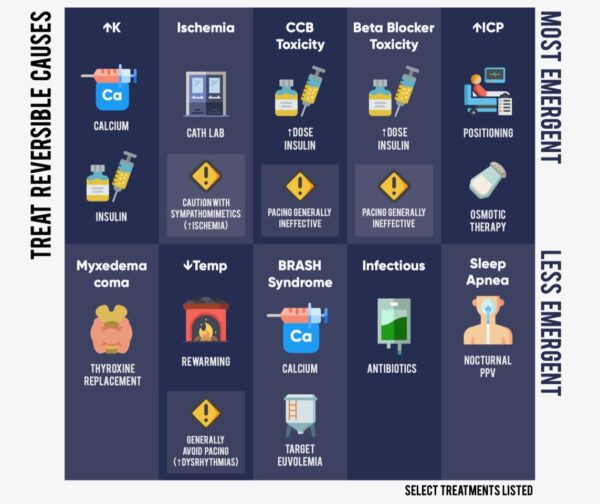
- The underlying cause needs to be taken into consideration (i.e., for B-blocker overdose or Calcium channel blocker overdose, consider high dose insulin, for digoxin overdose consider digiFab, for the hypothermic patient rewarming is usually required before consideration of medications or pacing, for myxedema coma, consider thyroxine)
Atropine for bradycardia and bradydysrhythmias
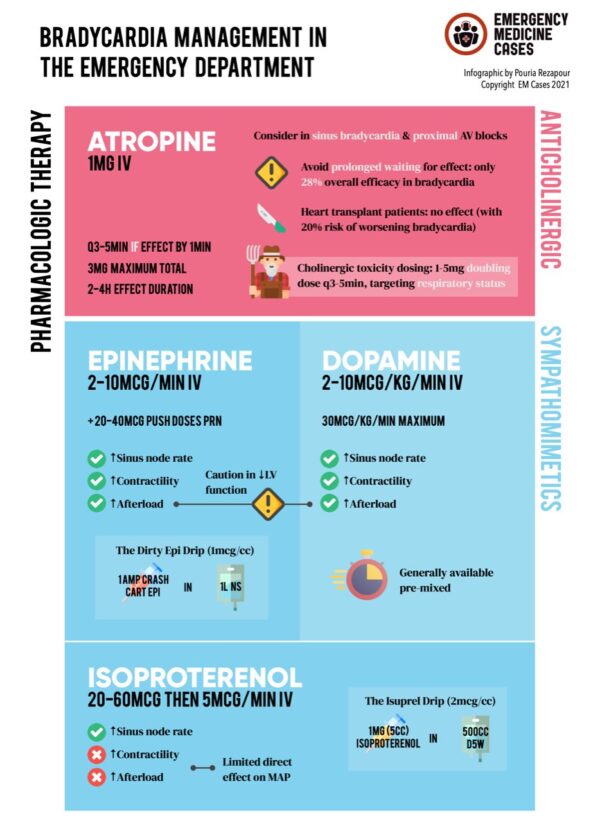
Atropine essentially fires up the SA node by poisoning the vagus nerve; it therefore is effective only if the distal conduction system is conducting normally. Overall, only 28% of patients with bradycardia have been shown to respond to atropine.
Appropriately dosed atropine is usually effective for proximal AV block, sinus bradycardia and junctional rhythms but is not useful (nor particularly harmful) in distal AV block (idioventricular rhythms and second-degree type II and third-degree AV block).
In the latest 2020 AHA update the recommended single dose administration of atropine was increased from 0.5 mg to 1 mg based on data suggesting that at low doses, atropine may cause paradoxical bradycardia. At low doses, atropine decreases heart rate by blocking M1 acetylcholine receptors in the parasympathetic ganglion controlling the SA node. At higher doses, atropine increases heart rate by blocking M2 acetylcholine receptors on the myocardium itself. Atropine-induced bradycardia may be especially difficult to manage in patients who are morbidly obese or post cardiac transplantation.
Atropine dosing: 1mg IV q3 mins, max 3mg (cholinergic poisoning may require higher doses using a doubling approach: 1mg, then 2mg, 4mg, 8mg etc.)
Beware: cardiac transplant patients may have paradoxical worsening of bradycardia with atropine; atropine should generally be avoided in cardiac transplant patients
Most sick bradycardia patients will not respond to atropine, so it is important to move quickly to chronotropic drugs such as epinephrine if atropine is not effective.
Pitfall: underdosing atropine and waiting for it to work too long before moving onto a chronotropic drug is a common pitfall in the treatment of bradycardia
Epinephrine and dopamine for bradycardia and bradydysrhythmias
If the first dose of 1mg atropine IV is ineffective, move quickly to chronotropic drugs – dopamine and/or epinephrine – while concurrently administering additional 1mg doses of atropine q3 mins (max 3mg). The advantage of dopamine is that it comes premixed and so can be started quickly, while epinephrine push-dose or infusion both require mixing.
Epinephrine dosing: 2-10 mcg/min infusion (it is safe to use a proximal peripheral line initially with frequent limb checks)
Temporize with push dose epinephrine boluses of ~20-50 mcg
*Push dose epinephrine recipe from EMCrit
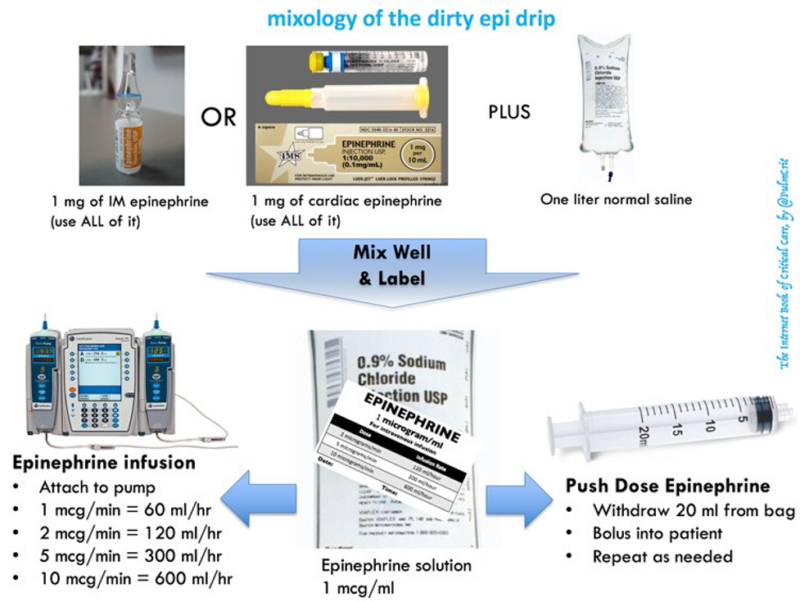
Source: Internet Book of Critical Care, Jan, 2017 Josh Farkas
Calcium for bradycardia and bradydysrhythmias
If atropine, dopamine, epinephrine and pacing are ineffective, and the cause of bradycardia is unclear, consider IV calcium chloride or calcium gluconate.
Calcium-responsive bradycardias
- Hyperkalemia
- Hypocalcemia
- Hypermagnesemia
- Calcium-channel blocker overdose
Dosing: Calcium chloride 1g OR Calcium gluconate 3g
![]() Update 2021: Double-blind, placebo-controlled RCT with 397 adult patients with out-of-hospital cardiac arrest in Denmark, assessing IV/IO doses of calcium chloride versus sodium chloride. With regards to impact on sustained ROSC and outcomes of survival and favorable neurological outcomes at 30 and 90 days, found no significant improvement of sustained ROSC in IV/IO calcium group, and study was halted early due to concerns about harm in calcium group. Abstract
Update 2021: Double-blind, placebo-controlled RCT with 397 adult patients with out-of-hospital cardiac arrest in Denmark, assessing IV/IO doses of calcium chloride versus sodium chloride. With regards to impact on sustained ROSC and outcomes of survival and favorable neurological outcomes at 30 and 90 days, found no significant improvement of sustained ROSC in IV/IO calcium group, and study was halted early due to concerns about harm in calcium group. Abstract
Reverse any other underlying cause of bradycardia
Cardiac ischemia – primary goal is cardiac catheterization/revascularization; transfer patient to cath lab ASAP, consider bradycardia medications/transcutaneous pacing only as a bridge to catheterization; use minimal doses of dopamine and/or epinephrine as either drug may exacerbate cardiac ischemia
Hypothermia – warming measures usually preclude the need for bradycardia medications/pacing; rewarming is the first line treatment for bradycardia in patients with severe hypothermia; pacing may precipitate ventricular fibrillation in severely hypothermic patients
Myxedema coma – thyroxine
Pearl: inferior MIs tend to cause narrow complex, transient, vagal-type bradycardia that is likely to respond to atropine vs anterior MIs tend to cause wide complex bradydysrhythmias that require pacing
Pearls on treatment of “The Brady Bunch” toxicologic causes of bradycardia
- Pacing is unlikely to be successful in B-blocker and Ca-blocker poisonings
- For B-blocker and Ca-blocker consider high dose insulin and lipid emulsion
- Glucagon should be reserved as a last resort and should not be given routinely
- Digoxin toxicity can cause almost any bradyarrhythmia from junctional bradycardia to complete heart block
- One clue to differentiate calcium blocker toxicity from B-blocker toxicity is that Ca-blocker poisoning tends to cause hyperglycemia vs B-blocker poisoning tends to be normoglycemic or hypoglycemic
- Consider bicarb for propranolol toxicity as it has NA channel blocking properties; QRS widens as the toxic effects progress
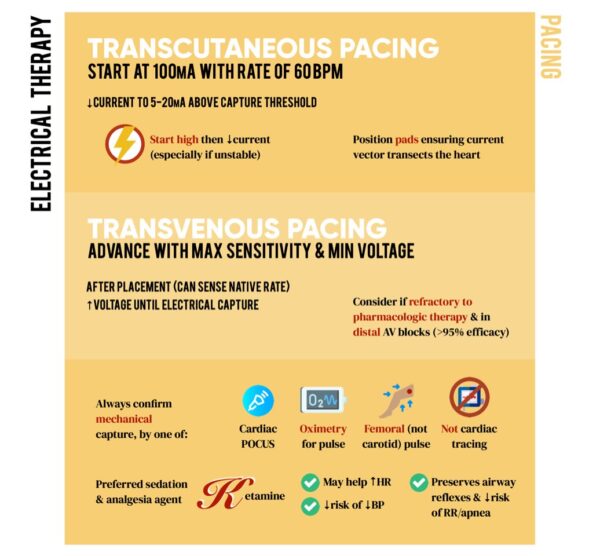
Transcutaneous pacing for bradycardia and bradydysrhythmias
In the crashing bradycardic patient, transcutaneous pacing should be started in parallel with medications. Transcutaneous pacing is a temporizing measure to definite care in the crashing bradycardia patient; when one has more than a few minutes to correct the bradycardia, transvenous pacing is preferred.
Pitfalls in transcutaneous pacing
- When employing transcutaneous or transvenous pacing, confirm real capture that results in a ventricular beat with femoral pulse checks (ideally using POCUS) and pulse oximetry wave. Do not rely solely on the monitor/ECG.
- Do not use a carotid pulse check for the assessment of circulation as TCP can create muscular movements that may feel like a carotid pulse. Assess circulation using the femoral pulse (with POCUS ideally).
- If the patient is crashing start the output high (i.e.,100mA); do not start at 5mA and increase as one would for more stable patients
Setting the output on the pacer
- In the crashing patient, start at 100mA and titrate downward to 5-20mA above the minimum energy required for capture; if not capturing, increase to max 130mA and if still not capturing, move the pads to improve the vector through the heart and try again.
- Patients with obesity and COPD typically require ~40-80 mA more than other patients to capture
- Our experts suggest to set the rate of pacing at 60 bpm
Video transcutaneous pacing procedure
Consider ketamine as your first line analgesic for the patient undergoing transcutaneous pacing as it is least likely to cause hypotension, may help increase the heart rate and it helps maintains respirations
![]() Update 2022: A prospective trial with 20 patients in an electrophysiology lab scheduled to undergo elective cardioversion found that AP pacing was more likely to capture than the AL position (78% versus 42%), and also required 33mA less current than the AL position (P=0.0001, 95% CI 20-45). Abstract
Update 2022: A prospective trial with 20 patients in an electrophysiology lab scheduled to undergo elective cardioversion found that AP pacing was more likely to capture than the AL position (78% versus 42%), and also required 33mA less current than the AL position (P=0.0001, 95% CI 20-45). Abstract
Transvenous pacing for bradycardia and bradydysrhythmias
- Transvenous is much more effective than transcutaneous pacing with success rates of >95%
- Transvenous pacing is indicated when drugs fail and for high degree AV blocks
- Start at 5mA output in stable patients and titrate upwards until capture; then set output at 5-20mA above the minimal capture output
- Use POCUS to follow the wire to make sure the tip sits in the IVC
Video transvenous pacing procedure
Indications for permanent pacemaker for bradycardia and bradydysrhythmias
The decision to place a permanent pacemaker is almost never made in the ED; nonetheless it is important for the EM physician to be aware of which patients are likely to require permanent pacemaker at a later date.
The AHA guidelines state: “In sinus node dysfunction, there is no established minimum heart rate or pause duration where permanent pacing is recommended. Establishing temporal correlation between symptoms and bradycardia is important when determining whether permanent pacing is needed. In patients with acquired second-degree Mobitz type II atrioventricular block, high-grade atrioventricular block, or third-degree atrioventricular block not caused by reversible or physiologic causes, permanent pacing is recommended regardless of symptoms. For all other types of atrioventricular block, in the absence of conditions associated with progressive atrioventricular conduction abnormalities, permanent pacing should generally be considered only in the presence of symptoms that correlate with atrioventricular block.”
Dr. Dorian has found in practice that patients with sinus node disease or with AV nodal block not infrequently inappropriately receive pacemakers, while patients with bundle branch block with seemingly innocuous syncope who should receive a permanent pacemaker, sometimes do not, even though they may be at risk for life-threatening distal block.
Learn more about transvenous pacemaker placement at EM Quick Hits 20 (skip to 24:48)
Learn more about the ED approach to bradycardia at Ep 154: 4-Step Approach to Bradycardia and Bradydysrhythmias
References
- F.M. Kusumoto, M.H. Schoenfeld, C. Barrett, J.R. Edgerton, K.A. Ellenbogen, M.R. Gold, et al.2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay. J Am Coll Cardiol (2018) Oct 31. pii: S0735-1097(18)38984-8.
- Carron M, Veronese S. Atropine sulfate for treatment of bradycardia in a patient with morbid obesity: what may happen when you least expect it. BMJ Case Rep. 2015;2015
- Ufberg JW, Clark JS. Bradydysrhythmias and atrioventricular conduction blocks. Emergency Medicine Clinics of North America. 2006;24(1):1-9.
- Sodeck GH, Domanovits H, Meron G, et al. Compromising bradycardia: Management in the emergency department. Resuscitation. 2007;73(1):96-102.
- Bernheim A, Fatio R, Kiowski W, Weilenmann D, Rickli H, Brunner-La R. Atropine often results in complete atrioventricular block or sinus arrest after cardiac transplantation: an unpredictable and dose-independent phenomenon. Transplantation. 2004;77(8):1181-1185.
- Carron M, Veronese S. Atropine sulfate for treatment of bradycardia in a patient with morbid obesity: what may happen when you least expect it. BMJ Case Rep. 2015;2015.
- Brady W, Swart G, DeBehnke D, Ma O, Aufderheide T. The efficacy of atropine in the treatment of hemodynamically unstable bradycardia and atrioventricular block: prehospital and emergency department considerations. Resuscitation. 1999;41(1):47-55.
- Deal N. Evaluation and management of bradydysrhythmias in the emergency department. Emerg Med Pract. 2013;15(9):1-15.
- Sidhu, S., & Marine, J. E. (2020). Evaluating and managing bradycardia. Trends in Cardiovascular Medicine, 30(5), 265-272.
Other FOAMed resources on Bradycardia and Bradydysrhythmias
Low and Slow Poisoning EM Cases (B-blocker, Ca-blocker, Digoxin toxicity recognition and management)
Bradycardia Atropine vs. Epinephrine for bradycardic periarrest (https://emcrit.org/pulmcrit/epinephrine-atropine-bradycardia/) (PulmCrit)
Bradycardia (https://lifeinthefastlane.com/resources/bradycardia-ddx/) (Chris Nickson, LITFL)
Managing unstable bradycardia (https://first10em.com/bradycardia/) (First 10 EM, Justin Morgenstern)
Symptomatic Bradycardia (http://www.emdocs.net/em3am-symptomatic-bradycardia/) (Erica Simon, emDocs)
An approach to bradycardia in the emergency department (http://www.emdocs.net/approach-bradycardia-ed/) (Patrick Ng, emDocs)
BRASH syndrome & failure of the ACLS bradycardia algorithm (https://emcrit.org/pulmcrit/brash-syndrome-bradycardia-renal-failure-av-blocker-shock-hyperkalemia/) (PulmCrit)
Drs. Helman, Dorian and Hedayati have no conflicts of interest to declare
Now test your knowledge with a quiz.



Well taught. Very interactive and interesting!
Id like to comment on the provided update conserning a study with the reported lack of benefit for iv calcium in cardiac arrest. in the study setting, all patients with an identified indication for calcium (e.g. hyperkalemia) were excluded and what was actually studied was whether iv calcium should be used as an empiric medication in all cardiac arrest patients. No conclusions on neither whether calcium is beneficial in the setting of a known indication for it nor whether it should be used as an empiric treatment for bradyarrythmias should be made.