

In part 1 of our 2 part series on cardiac arrest with Sara Gray, Bourke Tillman, Scott Weingart and Rob Simard we delved into the core components of cardiac arrest care: chest compressions, defibrillation, medications and airway. In this part 2 we discuss some of the finer art of cardiac arrest care and answer questions such as: how should we best communicate to EMS, the ED team and the family of the patient to keep the team focused, garner the most important info and keep the flow of the code going? How should we integrate PoCUS into cardiac arrest care so we do not interrupt the core components, yet we gain valuable data? What are the indications for consideration of ECPR/ECMO in cardiac arrest? What factors need to be taken into consideration to decide on when to terminate resuscitation of the cardiac arrest patient – when to call the code? and many more…
Podcast: Play in new window | Download (Duration: 1:03:18 — 58.0MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Saswata Deb, edited by Anton Helman June, 2022
Cite this podcast as: Helman, A. Episode 170 Cardiac Arrest – PoCUS Integration, Communication Strategies, E-CPR, Calling the Code. Emergency Medicine Cases. June, 2022. https://emergencymedicinecases.com/cardiac-arrest-pocus-integration-communication-strategies-e-cpr. Accessed [date]
Go to part 1 of this 2-part podcast on cardiac arrest care
Intergration of PoCUS into cardiac arrest resuscitation
PoCUS pulse checks
Pulse checks are only needed if an organized rhythm is seen on the monitor.
Manual pulse checks have been shown to be insensitive, not specific and have poor inter-rater reliability. One study showed that rescuer pulse palpation was only 78% accurate. Even if a pulse is felt, this does not guarantee adequate perfusion to vital organs.
Have a dedicated experienced provider look on PoCUS for a carotid pulse during chest compressions so that as soon as a pause in chest compressions to assess for cardiac rhythm occurs at the end of 2 minutes of compressions, the pulse can be rapidly assessed along with the cardiac rhythm in less than 5 seconds (as opposed to less than 10 seconds as recommended in the guidelines).
Several observational studies have shown that use of PoCUS during cardiac arrest prolongs pauses in chest compressions, however a recent study showed that with minimal training PoCUS pulse checks were more accurate than manual pulse checks and completed accurately within 5 seconds.
The REASON Trial was a multicenter prospective observational study of 793 patients with out-of-hospital cardiac arrest comparing arrests run with PoCUS performed at the beginning and end of the arrest and without. While survival to hospital admission and hospital discharged looked promising for the PoCUS group, it is unclear whether PoCUS improved neurologically intact long term survival.
![]() Update 2022: A prospective study found that pulse checks using carotid artery compression with an ultrasound probe was faster compared to manual palpation (1.62 seconds vs 3.5 seconds respectively), and the time to determine ROSC was significantly shortened to 0.44 times the manual palpation time (P<0.001). Abstract
Update 2022: A prospective study found that pulse checks using carotid artery compression with an ultrasound probe was faster compared to manual palpation (1.62 seconds vs 3.5 seconds respectively), and the time to determine ROSC was significantly shortened to 0.44 times the manual palpation time (P<0.001). Abstract
How to prevent long pauses in chest compressions using POCUS
- Generate the image during chest compressions
- Team member counts down from 10 before pause in chest compressions while PoCUS team member prepares to interpret and record image
- Record a video for 4-5 seconds during the chest compression pause and watch it after chest compressions have resumed if further interpretation is required
Step-wise approach to integration of PoCUS in cardiac arrest care
1st pause in chest compressions: perform a PoCUS pulse check at the femoral (or carotid) artery (maximum 10 seconds, usually takes 5 seconds)
If no PoCUS pulse seen, resume chest compressions, administer epinephrine 1 amp, assess ETCO2 (as per ACLS guidelines) and/or place arterial line and set up for cardiac PoCUS for the second rhythm/pulse check, draw and send STAT electrolytes from a blood gas.
If PoCUS pulse seen, treat as profound shock state: do not resume chest compressions, hold epinephrine 1 amp, assume cardiac contractility and assess for brain and heart perfusion by persistent presence of oxygen saturation waveform and/or ETCO2>40 and/or arterial line DBP>40 and/or cuff MAP ≥50-60; maintain or start norepinephrine 10-50 micrograms via well running antecubital peripheral IV and titrate to MAP of ≥60, correct hypoxemia and hypovolemia and search for causes of PEA using cardiac, lung and abdominal PoCUS, ECG, electrolytes from a blood gas and EMS/collateral history.
2nd pause in chest compressions: perform a cardiac PoCUS (subxiphoid or alternate view) by generating an image at least 10 seconds prior to pausing chest compressions and as chest compressions are stopped hit the video record button, attempt interpretation of the image in 5-10 seconds maximum, resume CPR and, if need be, watch the video clip for further interpretation looking for: vigorous cardiac contractility (not only valve motion), and clues to anatomical causes of PEA to be interpreted appropriately in the specific clinical setting – collapsed RV (cardiac tamponade or tension pneumothorax), enlarged RV with septal bowing (pulmonary embolism), severe poor LV function (MI).
If vigorous cardiac activity on PoCUS but no PoCUS pulse (based on the first PoCUS pulse check), this is most likely due to profound hypovolemia. There are 2 options:
- Resume CPR, administer 1 amp epinephrine if <3 have been administered, while aggressively searching for and reversing causes as per ACLS guidelines (with focus on causes of profound hypovolemia), or
- Treat as profound shock state: pause chest compressions and repeat the PoCUS pulse check to see if a pulse has been generated in the interim, assess for other signs of ROSC (oxygen saturation waveform, ETCO2 and DBP on arterial line) and administer or titrate vasopressor (see vasopressor choices below).
3rd and 4th pauses in chest compressions: (ideally using 2 ultrasound machines – one for PoCUS pulse and other searching for PEA causes) perform a lung PoCUS during one pause in compressions while assessing for manual pulse (or PoCUS pulse with a second machine) and signs of end-organ perfusion, and an abdominal PoCUS during another pause in compressions, the order depending on the clinical scenario, looking for clues to anatomical causes of PEA – tension pneumothorax (collapsed RV, lack of lung sliding, lack of power slide, absence of normal comet tail or reverberation artifacts, presence of a “lung point” or “transition point”), ruptured AAA, severe hypovolemia (flat IVC, free fluid).
Learn more about how performing lung PoCUS can be used to rule out pneumothorax in PoCUS Cases 2 Pneumothorax
Learn more about using PoCUS to diagnose ruptured/leaking AAA in POCUS Cases 10 AAA
Pearl: IVC PoCUS – while CPR is ongoing, it is feasible to check the IVC as well as the lungs for pneumothorax. If the IVC is plethoric, then obstructive causes of the arrest should be considered.
Example of algorithm to integrate POCUS into cardiac arrest resuscitation
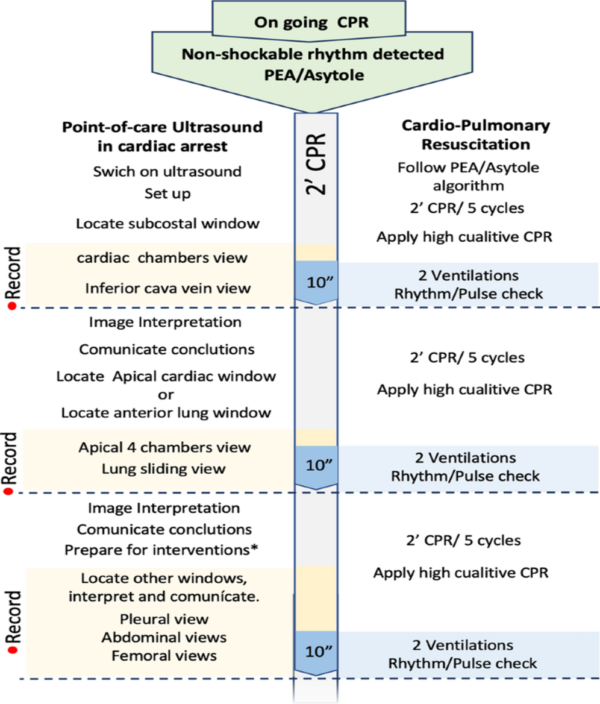
Source: Ávila-Reyes, D., Acevedo-Cardona, A.O., Gómez-González, J.F. et al. Point-of-care ultrasound in cardiorespiratory arrest (POCUS-CA): narrative review article. Ultrasound J 13, 46 (2021). https://doi.org/10.1186/s13089-021-00248-0
PoCUS for prognostication in cardiac arrest
The American Heart Association, 2020 guidelines recommends against the use of PoCUS for prognostication during CPR. However, in the hands of an experienced PoCUS user, findings on PoCUS may provide an ancillary data point that may aid in the decision to continue or terminate CPR. The REASON 1 prospective observational trial showed that survival to discharge was 0.6% for patients in cardiac standstill and 3.8% for patients with cardiac activity; intermittent “flickering” of the heart on PoCUS should not be considered cardiac standstill.
![]() Update 2025: In a multi-center prospective study of adults presenting to the emergency department after out-of-hospital cardiac arrest (OHCA), occult ventricular fibrillation (VF) (defined as VF seen on echocardiography despite a non-shockable ECG rhythm) occurred in a clinically significant minority, and identifying it may have important implications for resuscitation and survival outcomes. Abstract
Update 2025: In a multi-center prospective study of adults presenting to the emergency department after out-of-hospital cardiac arrest (OHCA), occult ventricular fibrillation (VF) (defined as VF seen on echocardiography despite a non-shockable ECG rhythm) occurred in a clinically significant minority, and identifying it may have important implications for resuscitation and survival outcomes. Abstract
- Primary outcomes:
- Incidence of occult VF: percentage of patients with echocardiography-detected VF despite a non-shockable ECG rhythm.
*In the study cohort, ~5.0–5.3% of resuscitation pauses demonstrated occult VF not identified on ECG alone.
- Incidence of occult VF: percentage of patients with echocardiography-detected VF despite a non-shockable ECG rhythm.
- Secondary outcomes:
- Survival to hospital discharge associated with occult VF and myocardial activity patterns.
*Patients with echocardiographic positive myocardial activity (PMA) had higher survival to admission (≈29.1%) compared with those classified as PEA on ECG alone (≈21.4%).
- Survival to hospital discharge associated with occult VF and myocardial activity patterns.
TEE in cardiac arrest: Is there a role?
- During and post cardiac arrest, transesophageal echo (TEE) may have a role in improving chest compressions quality, shorten pulse check times, guiding differential diagnosis and allowing adequate cardiac views in a small subset of patients where no window exists subxiphoid or transthoracically
- However, there is no patient-oriented outcome data to date.
- Compared to transthoracic/subxyphoid POCUS, TEE often generates better quality images and does not take up important space on the patient’s chest needed for compressions, defibrillator pads etc.
- TEE requires a dedicated physician during cardiac arrest.
- There exist descriptions of effective simulator-based training strategies as well as workshops for TEE skill learning
EM Quick Hits on TEE in Cardiac Arrest (skip to 18:43)
Episode 131 PEA arrest, PseudoPEA and PREM with Rob Simard and Scott Weingart
Approach to PEA Arrest – Beyond ACLS with Rob Simard
ACLS Guidelines 2015- Cardiac Arrest Controversies Part 1
Communication skills in cardiac arrest
The quality of resuscitation of a patient in cardiac arrest hinges on strong communication. There are 4 pertinent stages where this is key; pre-arrival, handover from emergency medical services (EMS), during the resuscitation, and speaking with the family.
Throughout each of the stages, resuscitation leaders should have a tone and body language that demonstrates respect and inclusiveness, listen meticulously, and practise closed-loop communication. This may further enhance team performance during an arrest which is often a stressful situation.
Pre-arrival cardiac arrest team communication skills
During the few precious minutes before a cardiac arrest patient arrives in the resuscitation bay, in addition to preparing the necessary equipment and resources, this time should be spent preparing the team.
4 points to discuss with the team are:
- What do we know? The stem received from the EMS call can be summarized to the team.
- What do we expect to see?
- What do we do? This can include discussing all the resources required, and contingency plans,
- Role assignment. This can also include asking members of the team to prepare, monitor, and manage the patient in the first few minutes while the resuscitation leader is getting handover from the EMS.
Communication skills during EMS handover of cardiac arrest patient
Pertinent information to gather from EMS include:
- symptoms prior to arrest,
- initial rhythm,
- total ‘down-time’,
- number of shocks administered,
- medications given,
- pertinent past medical history, home medications and allergies,
- social history including known code status and substitute decision maker
Closed-loop communication is key when receiving handover. Some ways to do this include summarizing back to the EMS the information received or writing down the pertinent points on a white-board.
Communication skills during the resuscitation of cardiac arrest patient
While running the resuscitation of the cardiac arrest patient, constant sharing of the mental model with the team can help to optimize team performance. This can include a short synopsis of the current status, next step and priorities (ie., continue with great CPR), and ask for any suggestions. Consider doing this every 5 minutes. While going through these steps, keeping a positive tone and reinforcing positive actions (ie., excellent CPR) can enhance team performance. If time permits, ask for feedback from your team on your communication skills after the code is terminated.
Communicating the family of the cardiac arrest patient
This can be done during the resuscitation (ie., discussion prior to terminating the resuscitation) or after the resuscitation.
SPIKES mnemonic for breaking bad news
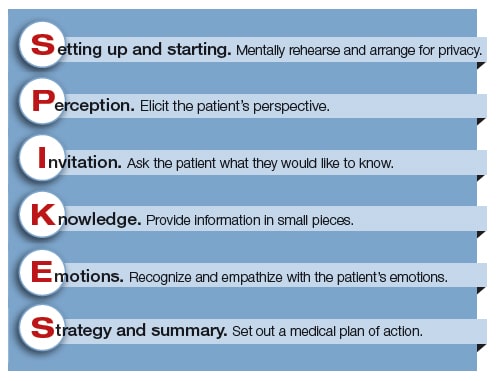
Some of the key elements to communicating with the family of a cardiac arrest patient include:
- Bring a social worker or nurse or someone who can spend time with the family after you leave the room
- Invite everyone to sit down, and sit down yourself
- Have tissue paper available in the room and offer it prn
- Use the words “died” or “dead” rather than “passed away” or “is no longer with us” early in the conversation
- Explain in simple, clear terms the events that transpired in as few sentences as possible
- After you tell the family that their relative has died pause and wait until they say something rather than rushing to the next steps
- Assure them that everyone involved (witnesses, EMS, ED staff) did everything they could
- Ask them if they have any questions
- When you leave the room tell them how long you will be in the department for and who to direct any further questions to
Mike Winters’ Best Case Ever on Communication skills in cardiac arrest
Dr. Weingart’s recommended reading to enhance communication skills: Non-violent Communication
The nurse-led code
Having a dedicated nurse leading the cardiac arrest code has been shown to improve time to defibrillator application (23.5 s vs 59 s), time to correction of ineffective compressions (7.5 s vs 14 s), compression fraction (91.3 vs 89.9), and time to address reversible causes (107.1 s vs 209.5 s).
Other advantages of nurse-led code:
- physician cognitive offload for advanced diagnostic and therapeutic decision making
- reduction in room crowding
Implementing nurse-led codes requires prior team simulation training.
Extra-Corporeal CPR (ECPR)
ECPR is a consideration when ROSC is not achieved despite standard ACLS. ECPR is the initiation extracorporeal membrane oxygenation (ECMO) while a patient is in cardiac arrest. The standard insertion of ECMO in this situation is usually a Veno-Arterial (V-A) ECMO which takes over the function of the heart and lungs.
The most recent (2019) American Heart statements on ECPR are that there is insufficient evidence to recommend its routine use in patients in cardiac arrest. However, it can be considered for selected patients when standard CPR is failing and ECPR can be started quickly by experienced ECMO providers.
Much of the ECPR data stem from observational studies. There are however a few promising RCTs. The ARREST trial reported improved survival to discharge time in patients that underwent early ECPR compared to standard ACLS. Another trial from Prague reported an absolute risk difference of approximately 10% for survival at 180 days with good neurological outcome (ECPR 31.5% vs 22% in standard ACLS), however this did not reach statistical significant as the study was underpowered.
Indications for consideration of ECPR
- Witnessed arrest AND
- Less than 5-10 minutes of CPR (Consider the decision for ECPR early) AND
- Physiologically young (relatively healthy) AND
- No end-stage co-morbidities AND
- Short transport time to cardiac center with ECMO expertise or timely ECMO team arrival at base hospital
![]() Update 2022: A multicenter study from Japan using registry data on 517 patients with OHCA who underwent ECPR between 2012 and 2019 found that age <75, time from emergency call to hospital arrival within 45 minutes, and initial shockable rhythm were predictive of good neurological outcome and survival at one month (CRITICAL study). Abstract.
Update 2022: A multicenter study from Japan using registry data on 517 patients with OHCA who underwent ECPR between 2012 and 2019 found that age <75, time from emergency call to hospital arrival within 45 minutes, and initial shockable rhythm were predictive of good neurological outcome and survival at one month (CRITICAL study). Abstract.
![]() Update 2024: An updated meta-analysis and trial sequential analysis including 13 studies with 14 pairwaywise comparisons (6336 extracorporeal CPR and 7712 conventional CPR) found that ECPR was associated with greater precision in reducing overall in-hospital mortality (OR 0.63, 95% CI 0.50-0.79), as well as a significant decrease in mortality in OHCA (OR 0.62, 95% CI 0.45-0.84). Abstract
Update 2024: An updated meta-analysis and trial sequential analysis including 13 studies with 14 pairwaywise comparisons (6336 extracorporeal CPR and 7712 conventional CPR) found that ECPR was associated with greater precision in reducing overall in-hospital mortality (OR 0.63, 95% CI 0.50-0.79), as well as a significant decrease in mortality in OHCA (OR 0.62, 95% CI 0.45-0.84). Abstract
When to Terminate CPR – “Calling the Code”
There exists a wide practice variation in the length of time a cardiac arrest code is run.
A variety of factors need to be taken into consideration in deciding when to “call a code”; there is no single factor that predicts survival to good neurologic outcome and a common pitfall is to call a code based on one of these factors only.
- Pre-existing status prior to the cardiac arrest – age, baseline co-morbidities and frailty
- Initial cardiac rhythm – VF/pulseless VT and pseudoPEA generally have better outcomes than true PEA/asystole
- Time to chest compressions/time to first epinephrine dose
- End-tidal CO2 (< 10 mmHg at 20 minutes since downtime portends poor prognosis)
- Absence of adequate blood pressure on an arterial line
- Duration of CPR
- PoCUS cardiac contractility – The REASON 1 prospective observational trial showed that survival to discharge was 0.6% for patients in cardiac standstill and 3.8% for patients with cardiac activity; intermittent “flickering” of the heart on PoCUS should not be considered cardiac standstill
- Underlying cause – it is advisable to continue CPR in young people who have persistent VF until all attempts have been made to treat reversible causes, hypothermia, asthma (correction of dynamic hyperinflation), arrest due to toxic overdose (may require prolonged time for hemodynamic and neurological recovery), thrombolytics given during CPR (should continue up to 1.5-2 hours post-administration), pregnancy prior to perimortem caesarean section.
- The wishes of the patient’s family based on the patient’s values
Pitfall: A common pitfall is to assume cardiac standstill on PoCUS if the heart is “flickering” intermittently. When cardiac “flickering” is present, consider continuing resuscitation efforts
There is no evidence that severe hyperkalemia in all comer cardiac arrest patients portends a poor prognosis, however, hyperkalemia has been a factor considered in terminating resusctiation of patients suffering from hypothermia.
How long should a cardiac arrest code be run for?
As a general guide, there is a near zero likelihood of survival to hospital discharge with good neurologic outcome after 45-55 minutes of high quality CPR in cardiac arrest patients who have no ROSC during their resuscitation. When ECPR is employed this time frame may be extended to 90 minutes.
Pitfall: a common pitfall is to “call a code” after a predetermined amount of time such as 45-55 minutes when there has been intermittent or recurrent ROSC during this time. The 45-55 minute guide applies only to patients when no ROSC has been achieved.
Go to part 1 of this 2-part podcast on cardiac arrest care
References
- Ávila-Reyes D, Acevedo-Cardona AO, Gómez-González JF, et al. Point-of-care ultrasound in cardiorespiratory arrest (POCUS-CA): narrative review article. The Ultrasound Journal. 2021;13(1):46.
- Eberle B, Dick WF, Schneider T, Wisser G, Doetsch S, Tzanova I. Checking the carotid pulse check: diagnostic accuracy of first responders in patients with and without a pulse. Resuscitation. 1996; 33(2):107-116.
- Germanoska B, Coady M, Ng S, Fermanis G, Miller M. The reliability of carotid ultrasound in determining the return of pulsatile flow: A pilot study. Ultrasound. 2018;26(2):118-126.
- Ochoa FJ, Ramalle-Gómara E, Carpintero J., Garcıá A, Saralegui I. Competence of health professionals to check the carotid pulse. Resuscitation. 1998; 37(3):173-175.
- Moule P. Checking the carotid pulse: diagnostic accuracy in students of the healthcare professions. Resuscitation. 2000; 44(3):195-201.
- SchonbergerRB, LampertRJ, MandelEI, FeinleibJ, GongZ, HonidenS. Handheld Doppler to Improve Pulse Checks during Resuscitation of Putative Pulseless Electrical Activity Arrest: Anesthesiology. 2014; 120(4):1042-1045.
- Badra K, Coutin A, Simard R, Pinto R, Lee JS, Chenkin J. The POCUS pulse check: A randomized controlled crossover study comparing pulse detection by palpation versus by point-of-care ultrasound. Resuscitation. 2019;139:17-23.
- Simard RD, Unger AG, Betz M, Wu A, Chenkin J. The POCUS Pulse Check: A Case Series on a Novel Method for Determining the Presence of a Pulse Using Point-of-Care Ultrasound. J Emerg Med. 2019;56(6):674-679.
- Zengin S, Gümüşboğa H, Sabak M, Eren ŞH, Altunbas G, Al B. Comparison of manual pulse palpation, cardiac ultrasonography and Doppler ultrasonography to check the pulse in cardiopulmonary arrest patients. Resuscitation. 2018;133:59- 64.
- Volpicelli G. Usefulness of emergency ultrasound in nontraumatic cardiac arrest. The American Journal of Emergency Medicine. 2011; 29(2):216-223.
- Clattenburg EJ, Wroe P, Brown S, et al. Point-of-care ultrasound use in patients with cardiac arrest is associated prolonged cardiopulmonary resuscitation pauses: A prospective cohort study. Resuscitation. 2018; 122:65-68.
- Huis in ’t Veld MA, Allison MG, Bostick DS, et al. Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions. Resuscitation. 2017; 119:95-98.
- Wu C et al. The Predictive Value of Bedside Ultrasound to Restore Spontaneous Circulation in Patients with Pulseless Electrical Activity: A Systematic Review and Meta-Analysis. PLos one 2018.
- Atkinson P, Bowra J, Milne J, et al. International Federation for Emergency Medicine Consensus Statement: Sonography in hypotension and cardiac arrest (SHoC): An international consensus on the use of point of care ultrasound for undifferentiated hypotension and during cardiac arrest – CORRIGENDUM. CJEM. 2017;19(4):327.
- Gaspari R et al. Emergency Department Point-Of-Care Ultrasound in Out-Of-Hospital and in-ED Cardiac Arrest. Resuscitation 2016; 109: 33 – 39.
- Merchant RM, Topjian AA, Panchal AR, et al. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142(16_suppl_2):S337-S57.
- Kaplan M. SPIKES: a framework for breaking bad news to patients with cancer. Clin J Oncol Nurs. 2010 Aug;14(4):514-6.
- Pittman J, Turner B, Gabbott DA. Communication between members of the cardiac arrest team–a postal survey. Resuscitation. 2001 May;49(2):175-7.
- Calder LA, Mastoras G, Rahimpour M, et al. Team communication patterns in emergency resuscitation: a mixed methods qualitative analysis. Int J Emerg Med. 2017;10(1):24.
- Meisel ZF, Shea JA, Peacock NJ, et al. Optimizing the patient handoff between emergency medical services and the emergency department. Ann Emerg Med. 2015:65(3);310—317.
- Gilligan P. To lead or not to lead? Prospective controlled study of emergency nurses provision of advanced life support team leadership. Emergency Medicine Journal. 2005;22(9):628-632.
- Clements A, Curtis K, Horvat L, Shaban RZ. The effect of a nurse team leader on communication and leadership in major trauma resuscitations. International Emergency Nursing. 2015;23(1):3-7.
- Pallas JD, Smiles JP, Zhang M. Cardiac Arrest Nurse Leadership (CANLEAD) trial: a simulation-based randomised controlled trial implementation of a new cardiac arrest role to facilitate cognitive offload for medical team leaders. Emerg Med J. 2021 Aug;38(8):572-578. doi: 10.1136/emermed-2019-209298. Epub 2021 Jan 26.
- Gilligan P, Bhatarcharjee C, Knight G, Smith M, Hegarty D, Shenton A, Todd F, Bradley P. To lead or not to lead? Prospective controlled study of emergency nurses’ provision of advanced life support team leadership. Emerg Med J. 2005;22(9):628-632. doi:10.1136/EMJ.2004.015321.
- Leary M, Schweickert W, Neefe S, Tsypenyuk B, Falk SA, Holena DN. Improving providers’ role definitions to decrease overcrowding and improve in-hospital cardiac arrest response. Am J Crit Care. 2016;25(4):335-339. doi:10.4037/AJCC2016195.
- Panchal AR, Berg KM, Hirsch KG, et al. 2019 American Heart Association Focused Update on Advanced Cardiovascular Life Support: Use of Advanced Airways, Vasopressors, and Extracorporeal Cardiopulmonary Resuscitation During Cardiac Arrest: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2019;140(24):e881-e94.
- Link MS, Berkow LC, Kudenchuk PJ, et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132(18 Suppl 2):S444-64.
- Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396(10265):1807-16.
- Belohlavek J, Smalcova J, Rob D, et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2022;327(8):737-47.
- Klee TE, Kern KB. A review of ECMO for cardiac arrest. Resusc Plus. 2021;5:100083.
- Part 7.2: Management of Cardiac Arrest. Circulation. 2005;112(24_supplement):IV-58-IV-66.
- Nagao K, Nonogi H, Yonemoto N, et al. Duration of Prehospital Resuscitation Efforts After Out-of-Hospital Cardiac Arrest. Circulation. 2016;133(14):1386-96.
- Nickson C. Cessation of CPR. LITF: Life In The Fastlane 2020 [Available from: https://litfl.com/cessation-of-cpr/. Accessed: June 5, 2022.
- Tsou P, Kurbedin J, Chen Y et al (2017) Accuracy of point-of-care focused echocardiography in predicting outcome of resuscitation in cardiac arrest patients: a systematic review and meta-analysis. Resuscitation 114:92–99.
- Atkinson P, Beckett N, French J, et al. Does point-of-care ultrasound use impact resuscitation length, rates of intervention, and clinical outcomes during cardiac arrest? A study from the sonography in hypotension and cardiac arrest in the Emergency Department (SHoC-ED) Investigators. Cureus 2019;11(4):e4456. 8.
- Blaivas M, Fox J (2001) Outcome in cardiac arrest patients found to have cardiac standstill on the bedside emergency department echocardiogram. Acad Emerg Med 8:616–621.
- Lalande E, Burwash-Brennan T, Burns K, et al. Is point-of-care ultrasound a reliable predictor of outcome during atraumatic, non-shockable cardiac arrest? A systematic review and meta-analysis from the SHoC Investigators. Resuscitation 2019;139:159–66.
Drs. Helman, Gray, Tillmann and Weingart have no conflicts of interest to declare
Now test your knowledge with a quiz.



AMAZING TALK! Great podcast!
I just wanted to add that given that we suck at pulse checks, perhaps we could use POCUS to confirm mechanical capture while pacing post ROSC (ie overdrive pacing etc).
Does anyone have any experience with this?