
In this ECG Cases blog we use visual concepts of scale and proportion to identify false positive and subtle Occlusion MI…
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. February 2025
8 patients presented with potential ischemic cardiac symptoms. Using concepts of scale and proportionality, can you identify which were false positive STEMI and which had subtle Occlusion MI?
Case 1: 35 year old with syncope
–
Case 2: 60 year old with chest pain
–
Case 3: 90 year old with chest pain
–
Case 4: 60 year old with chest pain
–
Case 5: 85 year old with chest pain
–
Case 6: 70 year old weak and diaphoretic
–
Case 7: 70 year old, prior MI, with 3 hours of epigastric pain
–
Case 8: 75 year old, no cardiac history, with 2 hours of chest pain
–
The art of scale and proportionality in Occlusion MI
Let’s put the art in heart! This is the second in a series of blog post on the art of Occlusion MI: how we can use visual concepts to identify acute coronary occlusion on ECG, and how art helps explains the science of OMI. The first blog looked at mirror image, and this second post looks at scale and proportionality.
STEMI criteria has high rates of false positives and false negatives (missed occlusions), because it reduces the ECG to the ST segment, dichotomized by millimiters. But you can’t understand any measurements in isolation. For example, if the surrealist painting above was cropped to only show the foot, you could not assess its size . Scale is the size of one object compared to a different object: in the painting, the foot is large compared to the cactus. Similarly, the voltage of one ECG can be large compared to the voltage of a different ECG. Proportionality is the size of one part of an object relative to other parts of the same object: the leg and foot in the painting are large relative to the rest of the body. Similarly, we need to assess ST/T changes relative to their own QRS. Scale and proportionality allow us to identify false positive STEMI in patients with large scale voltage but proportional ST/T changes, and to identify false negative STEMI (subtle Occlusion MI) in patients with small/normal scale voltage but disproportionate ST/T changes.
The art of scale and proportionality has been used for scientific advances in identifying OMI, including
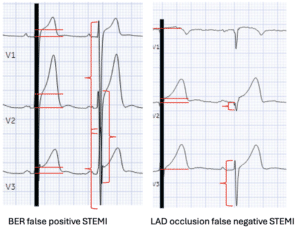
- BER vs LAD occlusion: both can have similar concave STE and T wave amplitude, but in BER it is proportional to QRS and in LAD occlusion it is disproportionate [1]
- hyperacute T waves: while LVH or BER may have large scale QRS and proportionally tall T waves, hyperacute waves have disproportionately large T waves relative to their QRS – not only tall but broad based, bulky and look inflated (like the foot in the painting above) [2]
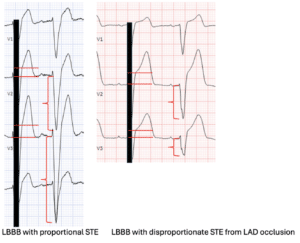
- LBBB +/- OMI: LBBB produces secondary, discordant and proportional ST changes, so LBBB with superimposed OMI can be identified by concordant ST elevation, concordant ST depression V1-3, or disproportionate discordant STE. Whereas Sgarbossa’s original third criteria (discordant STE>5mm) can lead to false positives with large QRS and false negatives with small QRS, the Smith-Modified Sgarbossa criteria uses proportionality (STE/S>25%) to accurately identify Occlusion MI [3]
- Anterior STEMI vs LV aneurysm: both can have anterior QS waves with mild ST elevation, but acute occlusions can be identified by hyperacute T waves large relative to their QRS, with T/QRS> 1/3 [4]
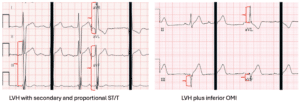
- LVH +/- OMI: while there is no rule, the concepts of scale and proportionality can help differentiate LVH with large scale QRS and proportional secondary ST/T from LVH with disproportionate ischemic ST/T changes
Back to the cases
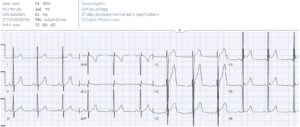
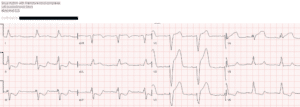
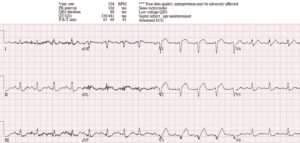
Case 1: 35 year old with syncope
- Heart rate/rhythm: normal sinus
- Electrical conduction: normal PR/QRS/QT
- Axis: normal
- R-wave progression: normal
- Tall/small voltages: tall voltages with J waves
- ST/T: STE and T waves proportional to tall voltages
= early repolarization
–
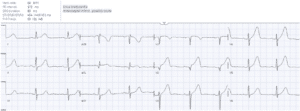
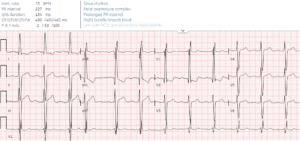
Case 2: 60 year old with chest pain
- H: sinus bradycardia
- E: normal
- A: normal
- R: QS in V2
- T: normal
- S: hyperacute T waves (large relative to QRS, bulky and inflated) anterolateral
= proximal LAD occlusion. Cath lab activated: 99% proximal LAD occlusion. First trop 5 ng/L and peak 200,000.
Here is a comparison of the ECGs above. Using STEMI criteria (measuring STE and ignoring QRS), the first is STEMI positive and the second STEMI negative. But looking at scale, the QRS of the first is much larger than the second; and using proportionality, the first has ST elevation and T waves proportional to its QRS, while the second has hyperacute T waves (disproportionate to its QRS).
–
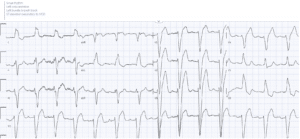
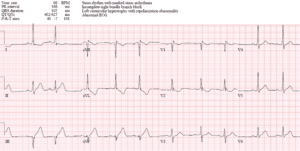
Case 3: 90 year old with chest pain
- H: normal sinus
- E: LBBB
- A: normal
- R: transition V5 from LBBBB
- T: tall voltages V3
- S: discordant and proportional ST changes. V3 has 6mm of STE which would meet the original Sgarbossa criteria, but using Smith-Modified Sgarbossa, amount of STE is proportional to its large QRS, with a ratio much less than 25% (STE/S = 6/37 = 16%)
= LBBB without ECG evidence for OMI. Serial troponin normal.
–
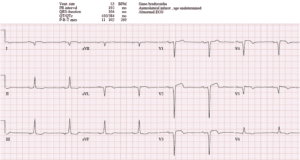
Case 4: 60 year old with chest pain
- H: normal sinus
- E: LBBB
- A: normal
- R: transition V5 from LBBBB
- T: normal
- S: concordant STE in aVL and excess discordant STE in V2-3 (STE/S>25%)
= proximal LAD occlusion. Cath lab activated: 100% proximal LAD occlusion
Here are the two ECGs above measuring the STE in isolation vs with scale and proportionality. Both have similar ST elevation in isolation, but the scale of the QRS is larger in the first compared with the second. As a result, the STE in the first is proportional to its QRS, while in the second it is disproportionate to its QRS.
–
Case 5: 85 year old with chest pain
- H: normal sinus with premature complex
- E: normal PR, RBBB
- A: left axis from LVH
- R: early R wave from RBBB
- T: tall voltages from LVH with strain
- S: discordant and proportional ST/T
= LVH with secondary repolarization abnormalities. Serial troponin normal.
–
Case 6: 70 year old weak and diaphoretic
- H: normal
- E: normal
- A: physiologic left, inferior Q
- R: early R in V2
- T: borderline LVH criteria in aVL
- S: TWI in aVL is disproportionate to its QRS, and reciprocal to hyperacute T waves inferior; as well as STD in V2 from posterior extension and hyperacute T wave in V6 from lateral involvement
= borderline LVH with infero-postero-lateral OMI. Cath lab activated: 100% RCA occlusion.
Here are the two ECGs above. Both have similar inferior T waves and T wave inversion in aVL. But in the first they are proportional and secondary to large QRS, while in the second they are disproportionate from primary ischemia:
–
Case 7: 70 year old, prior MI, with 3 hours of epigastric pain
- H: sinus brady
- E: normal conduction
- A: right axis from lateral Q
- R: late progression from anterior Q
- T: normal voltages
- S: small T waves relative to QRS, with terminal T wave inversion
= old LV aneurysm, false positive STEMI. Cath lab activated: no culprit, troponins negative.
–
Case 8: 75 year old, no cardiac history, with 2 hours of chest pain
- H: sinus tach
- E normal conduction
- A: normal axis
- R: anterior Q
- T: small voltages
- S: hyperacute T waves V1-4, with the T wave in V3 three times the size of its tiny QRS. There’s also STD V5-6 reciprocal to STE in V1-2, and STD inferior reciprocal to STE in aVL
= proximal LAD occlusion. Cath lab activated: 95% proximal LAD occlusi0n, first troponin 2,000 and peak 50,000.
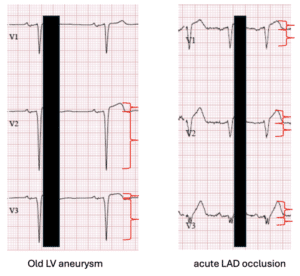
Here are the two ECGs above, both with the anterior QS waves and mild STE, so both were labeled anterior infarct ‘age undetermined’. But in the first the QRS is larger and the T waves are proportionally smaller, resulting in proportionally small T/QRS typical of LV aneurysm; while in the second the QRS is smaller and the T waves proportionally larger, resulting in hyperacute T waves.
–
Take away
- STEMI criteria can be false positive with large scale QRS and proportional ST elevation (eg LVH or BER), or false negative with low/normal scale QRS and disproportionate ST elevation and hyperacute T waves
- Rules for subtle occlusion using proportionality can help differentiate LBBB with or without OMI (Smith-Modified Sgarbossa: STE/S>25%), or LV aneurysm vs anterior STEMI with Q waves (T/QRS>0.36)
For more cases see ECG Cases 11: LBBB + Occlusion MI, and ECG Cases 21: hyperacute T waves and Occlusion MI
For small-group, live and highly interactive ECG courses, visit www.heartsECGcourse.com–including online courses and in-person pre-conference courses at Emergency Medicine Update in April 2025, and International Conference on Emergency Medicine in May 2025.
References
- Smith SW, Khalil A, Henry TD, et al. Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardial infarction. Ann Emerg Med 2012
- Smith SW, Meyers HP. Hyperacute T-waves can be a useful sign of occlusion myocardial infarction if appropriately defined. Ann Emerg Med 2023
- Meyers HP, Limkakeng AT, Jaffa EJ, et al. Validation of the modified Sgarbossa criteria for acute coronary occlusion in the setting of left bundle branch block: a retrospective case-control study. Am Heart J 2015
- Smith SW. T/QRS ratio best distinguishes ventricular aneurysm form anterior myocardial infarction. Am J Emerg Med 2005



Leave A Comment