

Topics in this EM Quick Hits podcast
Anand Swaminathan on optimizing RSI medication timing (1:08)
Brittany Ellis on ED boarding challenges in older patients and improving ED overcrowding and ED flow (7:30)
Dave Jerome on managing prolonged tourniquet application (30:21)
Nour Khatib and Phil Gillick on a rural peer support program case (39:20)
Jesse McLaren on ECG reciprocal changes in acute occlusion myocardial infarction: the mirror image (54:43)
Melody Ng on practical nutrition tips for shift workers (best of University of Toronto EM) (1:01:23)
Podcast: Play in new window | Download (Duration: 1:26:10 — 78.9MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Brandon Ng, edited by Anton Helman, January, 2025
Cite this podcast as: Helman, A. Swaminathan, A. Ellis, B. Jerome, D. Khatib, N. Gillick, P. McLaren, J. Ng. M. EM Quick Hits 62 – Optimizing RSI Medication Timing, ED Boarding of Older Patients, Prolonged Tourniquet Use, Rural Peer Support Programs, ECG Reciprocal Changes, Nutrition for Shift Workers. Emergency Medicine Cases. January, 2025. https://emergencymedicinecases.com/em-quick-hits-january-2025/. Accessed August 6, 2026.
Optimizing RSI Medication Timing
- Much of recent airway research relates to RSI preparation and tube delivery: Resuscitate prior to intubation, improve hemodynamics to decrease risk of peri-intubation hemodynamic collapse, improve oxygenation to increase safe apneic time, positioning, ramping, airway alignment, bed up, head elevated, and bougie first approach etc.
- Typical approach to RSI involves near simultaneous administration of induction and paralytic agents to rapidly result in ideal intubating condition. However, this approach often results in an induced but not paralyzed patient, causing difficulties with tube delivery as medication onset times differ:
- Succinylcholine: 45-60 seconds
- Rocuronium (1.2 mg/kg): ~60 seconds
- Etomidate: 30-40 seconds
- Ketamine: 30-45 seconds
- Propofol: 20-25 seconds
- As such, consider aiming for simultaneous onset rather than simultataneous administration of induction and paralytic agent.
- In studies by Driver et al. 2019 and Catoire et al. 2024, administering paralytic prior to induction agent is associated with lower first attempt intubation failure.
Bottom line => Consider administering paralytic first, then induction agent ~20-30 seconds later, ensuring simultaneous onset for optimal RSI while averting awake paralysis.
- Driver BE, Klein LR, Prekker ME, Cole JB, Satpathy R, Kartha G, Robinson A, Miner JR, Reardon RF. Drug Order in Rapid Sequence Intubation. Acad Emerg Med. 2019 Sep;26(9):1014-1021. doi: 10.1111/acem.13723. Epub 2019 Mar 19. PMID: 30834639.
- Catoire P, Driver B, Prekker ME, Freund Y. Effect of administration sequence of induction agents on first-attempt failure during emergency intubation: A Bayesian analysis of a prospective cohort. Acad Emerg Med. 2024 Oct 18. doi: 10.1111/acem.15031. Epub ahead of print. PMID: 39425254.
ED Boarding for Older Patients
This segment is the first part of our series on The Best of The International Conference of Emergency Medicine (ICEM) in anticipation of the ICEM Conference in Montreal May 2025
Strategies to Relieve ED Crowding, Improve Flow & Decrease Morbidity/Mortality Related to Boarding of Older Patients
ED boarding is often associated with delayed care, prolonged wait times, and physical and psychological stress
Older patients suffer from ED crowding and access block, and boarding older patients prolongs their hospital stay by exacerbating risks and underlying conditions such as delirium, functional decline, and pressure ulcers:
- Delirium is often exacerbated in the ED environment, thereby increasing mortality, length of stay, and risk of dementia
- Pressure ulcers can start within hours of immobility, and often have protracted courses leading to longer hospital stay and recurrent ED visits
- The increased comorbidities and length of stay, further contributes to ED and systemic over capacity as well as access block
Systems solutions to minimize complications of boarding older patients and improve ED flow
- Use of electronic health records and AI to better prioritize admissions and bed assignments
- Geriatric-focused hospital teams and units, or involvement of interprofessional teams
- Improved communication and care tools between hospital and community settings to have quick access to accurate past medical history, medications
- Start discharge planning early and better coordination with community resources
- Improved access to home care services, availability of alternative models of care (e.g. home hospital programs, transitional care spaces), PT/OT, and timely access to primary or specialist care to help prevent patients from needing to visit the ED
Local ED solutions to minimize complications of boarding older patients and improve ED flow
- Consider routinely implementing tools and scoring systems that identify the needs of older patients in the ED (e.g. frailty modifier for the CTAS system, inter IED screener, frailty scoring, delirium screeners)
- Utilizing tools to identify delirium in the ED (e.g. Delirium Triage Screen, Brief Confusion Assessment method)
- Implementing multi-component delirium preventions such as attention to mobilization, nutrition, sleep, and reorientation
- Early mobilization with physiotherapy to decrease hospital acquired disability and falls
- Prioritizing quiet spaces with beds, doors, windows, and lights for older patients
- Prioritizing the need for older patients to stay in a single treatment space
- Timely access to specialist care and services for older patients in the ED
Bottom line => Early identification and simple coordinated interventions for at-risk elderly patients can reduce boarding-related complications, improve ED flow and help curb ED crowding.
Deep dive main episode EM Cases podcast and post on ED Overcrowding and Access Block
- Lee S, Howard MA 3rd, Han JH. Delirium and Delirium Prevention in the Emergency Department. Clin Geriatr Med. 2023 Nov;39(4):535-551. doi: 10.1016/j.cger.2023.05.006. Epub 2023 Jun 14. PMID: 37798064; PMCID: PMC10719942.
- Brown CL, Tittlemier BJ, Tiwari KK, Loewen H. Interprofessional Teams Supporting Care Transitions from Hospital to Community: A Scoping Review. Int J Integr Care. 2024 Apr 2;24(2):1. doi: 10.5334/ijic.7623. PMID: 38618048; PMCID: PMC11012160.
- Hshieh TT, Yang T, Gartaganis SL, Yue J, Inouye SK. Hospital Elder Life Program: Systematic Review and Meta-analysis of Effectiveness. Am J Geriatr Psychiatry. 2018 Oct;26(10):1015-1033. doi: 10.1016/j.jagp.2018.06.007. Epub 2018 Jun 26. PMID: 30076080; PMCID: PMC6362826.
- Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in Older Persons: Advances in Diagnosis and Treatment. JAMA. 2017 Sep 26;318(12):1161-1174. doi: 10.1001/jama.2017.12067. PMID: 28973626; PMCID: PMC5717753.
- Picard A. Neglected no more: The urgent need to improve the lives of Canada’s elders in the wake of a pandemic. Random House Canada; 2021 Mar 2.
- Hshieh TT, Yue J, Oh E, Puelle M, Dowal S, Travison T, Inouye SK. Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis. JAMA Intern Med. 2015 Apr;175(4):512-20. doi: 10.1001/jamainternmed.2014.7779. Erratum in: JAMA Intern Med. 2015 Apr;175(4):659. doi: 10.1001/jamainternmed.2015.0994. PMID: 25643002; PMCID: PMC4388802.
- Wallis M, Marsden E, Taylor A, Craswell A, Broadbent M, Barnett A, Nguyen KH, Johnston C, Glenwright A, Crilly J. The Geriatric Emergency Department Intervention model of care: a pragmatic trial. BMC Geriatr. 2018 Dec 3;18(1):297. doi: 10.1186/s12877-018-0992-z. PMID: 30509204; PMCID: PMC6276263.
Managing Prolonged Tourniquet Application
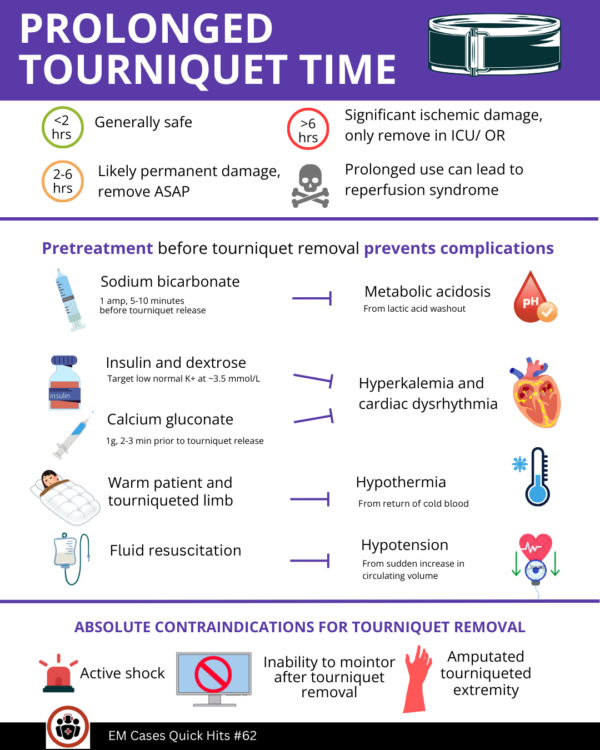
Tourniquets are generally safe for up to 2 hours; risks of prolonged tourniquet application include ischemic damage and reperfusion syndrome.
Reperfusion syndrome 4 key prevention treatment strategies
Reperfusion syndrome involves 4 key elements which can be managed with various strategies before removing the tourniquet:
- Sodium bicarbonate (1 amp, 5-10 min prior tourniquet release) for metabolic acidosis from lactic acid washout
- Insulin and dextrose (target low normal K+ at ~3.5mmol/L) for cardiac dysrhythmia from hyperkalemia and metabolic acidosis
- Calcium gluconate (1g, 2-3 min prior tourniquet release) to stabilize myocardium
- Having cardiac monitoring and defibrillation pads on
- Warming of tourniqueted limb and core body for hypothermia from cold limb acting as a heat sink and the return of cold blood
- Resuscitate to accommodate hypotension from sudden increase in circulating volume
Contraindications to tourniquet removal
Absolute contraindications for tourniquet removal include active shock, amputated tourniqueted extremity, and inability to monitor the patient after removal of tourniquet (TCCC Guidelines)
Tourniquet time may help risk stratify patients:
- < 2 hours: limb likely salvageable with minimal reperfusion syndrome risk
- 2-6 hours: likely permanent ischemic damage, pre-treat as above and remove tourniquet as soon as possible
- >6 hours: significant ischemic damage, significant reperfusion syndrome. Risk > benefit of releasing tourniquet. Remove tourniquet in a critical care environment
Bottom line => Proper treatment and monitoring are critical for safe tourniquet removal after prolonged application. Consider tourniquet time in making decisions on when it is appropriate to remove a tourniquet.
- Reperfusion Toolbox: https://cove.army.gov.au/article/reperfusion-toolbox
- TCCC Guidelines: https://tccc.org.ua/files/downloads/clinical-guidelines-2024-en.pdf
- Kragh JF Jr, Wade CE, Baer DG, Jones JA, Walters TJ, Hsu JR, Wenke JC, Blackbourne LH, Holcomb JB. Fasciotomy rates in operations enduring freedom and iraqi freedom: association with injury severity and tourniquet use. J Orthop Trauma. 2011 Mar;25(3):134-9. doi: 10.1097/BOT.0b013e3181e52333. PMID: 21321506.
- Kue RC, Temin ES, Weiner SG, Gates J, Coleman MH, Fisher J, Dyer S. Tourniquet Use in a Civilian Emergency Medical Services Setting: A Descriptive Analysis of the Boston EMS Experience. Prehosp Emerg Care. 2015 Jul-Sep;19(3):399-404. doi: 10.3109/10903127.2014.995842. Epub 2015 Feb 9. PMID: 25665102.
- Joarder M, Noureddine El Moussaoui H, Das A, Williamson F, Wullschleger M. Impact of time and distance on outcomes following tourniquet use in civilian and military settings: A scoping review. Injury. 2023 May;54(5):1236-1245. doi: 10.1016/j.injury.2023.01.031. Epub 2023 Jan 18. PMID: 36697284.
Rural EM Quick Hits Case
An otherwise healthy 65-year-old female presents to a rural ED with diarrhea, shortness of breath and a significantly elevated lactate. With the support of a peer physician support program a diagnosis of pulmonary embolism was clinched. Based on an elevated D-dimer and initial ECG findings of right heart strain an intermediate risk pulmonary embolism (PE) was the working diagnosis.
The classic ECG findings in acute pulmonary embolism are seen in a minority of patients, and are nonspecific as they can be seen in patients with chronic right heart strain as a result of pulmonary hypertension. The classic S1Q3T3 has an especially poor accuracy for the diagnosis of PE. Conversely, new flipped T waves in both the inferior and anterior leads are highly suggestive of acute PE.
- Sinus tachycardia (44%)
- Complete or incomplete right bundle branch block (18%)
- Right axis deviation (16%)
- Flipped T waves in both the inferior and right precordial leads is the most specific finding in favour of PE, with reported specificities of up to 99% in one study.
- S1Q3T3 pattern (low sensitivity and specificity for PE)

ECG of patient with acute pulmonary embolism with right axis deviation and flipped Ts in both inferior and anterior leads which is highly suggestive of acute PE

- Co I, Eilbert W, Chiganos T. New Electrocardiographic Changes in Patients Diagnosed with Pulmonary Embolism. J Emerg Med. 2017 Mar;52(3):280-285
- Ferrari E, Imbert A, Chevalier T, Mihoubi A, Morand P, Baudouy M. The ECG in pulmonary embolism. Predictive value of negative T waves in precordial leads–80 case reports. Chest. 1997 Mar;111(3):537-43.
- Rodger M, Makropoulos D, Turek M, Quevillon J, Raymond F, Rasuli P, Wells PS. Diagnostic value of the electrocardiogram in suspected pulmonary embolism. Am J Cardiol. 2000 Oct 1;86(7):807-9.
ECG Reciprocal Changes in OMI: Mirror Image
Reciprocal ECG changes, like a mirror, can help identify subtle occlusion myocardial infarctions (OMI). Steps to help identify OMI using the concept of mirror image include:
- Determine the ECG change, and where its mirror image is
- ST elevation may just be the mirror image of a secondary ST depression. For example:
- Abnormal depolarization in LVH, LBBB produces secondary ST depression and T wave inversion in V5-6, resulting in mirror image ST elevation in V1-2.
- Non-specific primary ST depression may lead to mirroring ST elevation, such as when ST elevation in AVR is the mirror image of global subendocardial ischemia (a high risk but non-specific pattern)
- Look for primary ischemic ST elevation or hyperacute T waves from acute coronary occlusion and its mirror ST depression and T wave inversion (which can be more obvious)
- Remember where the mirrors are
- “PAILS” is a confusing mnemonic that does not account for mid or distal LAD occlusions (anterior ST elevation without reciprocal inferior ST depression)
- Instead, recall how the leads related to the heart and which leads mirror each other:
- Limb leads (frontal plane) mirrors:
- right inferior (III) and high lateral (aVL)
- aVR and apex (II)
- Chest leads (horizontal plane) mirrors:
- Anterior (V2-4) and posterior (V8-9)
- Right anterior/septal (V1) and left lateral (V6)
- Limb leads (frontal plane) mirrors:

- Identify subtle occlusion MI using ECG changes or its mirror images
- Inferior OMI: Minimal ST elevation & hyperacute T wave ↔ mirror ST depression and T wave inversion in AVL
- High lateral OMI: subtle aVL changes ↔ mirror changes in lead III
- Posterior OMI: mirror ST depression in V2-4 (12 lead ECG only shows mirror image)
- Anterior OMI:
- Mid LAD: mirror images in posterior leads with ST depression (no changes on 12-lead ECG)
- Distal LAD: anterior & inferior ST elevation (easily mistaken for diffuse ST elevation of pericarditis)
- Proximal LAD: subtle ischemic changes in high lateral (aVL) or right anterior (V1) ↔ mirror inferior (III) ST depression or left lateral (V6)
Bottom line => Look beyond STEMI criteria to identify acute coronary occlusion; reciprocal changes and mirror-image interpretation are key in identifying OMIs.
For case examples and discussion on reciprocal changes and mirror image: ECG Cases 52 – The Art of Occlusion MI, part 1: Mirror Image
Register for Dr. McLaren’s HEARTS ECG Course to master your ECG interpretation skills.
Nutrition Tips for Shift Workers (ie EM Providers!)

As part of our best of University of Toronto EM series Anton interviews Dr. Melody Ng, an EM physician at North York General Hospital with a degree in nutrition who gives talks to EM providers on nutrition for shift workers…
What do we need to understand about how we metabolize food and drink as shift workers to inform what we ingest before shift, on shift and after shifts?
- Like how sunlight acts as a signal of daytime to the central nervous system, food also acts as a signal to the enteric nervous system. Shift work can lead to meals late night (or early morning) which can lead to misalignment of the central and peripheral circadian rhythm, resulting in metabolic derangements and chronic disease.
- Leptin (appetite suppressant) decreases and ghrelin (signals hunger) increases when sleep deprived even if it is not an accurate reflection of the calories you need.
- Each night of shift work increases insulin resistance, which in the long term can result in diabetes.
- Timing of meals are important: shift workers who only ate during the day had better health outcomes than those that ate during all their shifts.
- Insulin resistance also naturally varies throughout the day:
- No history of diabetes: less insulin resistant in the morning, more insulin resistant as the day goes on
- Diabetes: more insulin resistant in the morning, less as the day goes on
Why should I care about glycemic index?
- Glycemic index indicates how quickly and how high a food will spike your blood glucose, and glycemic load incorporates the glycemic index with the amount of carbohydrates. These can be used to estimate the stress of a meal on the pancreas to secrete insulin to regulate blood glucose.
- Information on glycemic index is available on the Diabetes Canada website.
- The glycemic index does not necessarily correlate with its healthiness, although processed foods generally have a higher glycemic index.
- Incorporating fiber in your diet helps with slowing the absorption and subsequent spike of carbohydrates.
What do you suggest we eat when we get home after a shift in the middle of the night or early morning? What are some healthy choices?
- Consider hydrating before reaching for food, as shift work often leads to thirst which can feel similar to hunger
- Example foods that may be considered include nuts (contains fibers and healthy fats), boiled egg (contains amino acids, vitamin D, choline), cheese, or avocado.
How do you prep your food around shifts so that it’s easy, efficient and healthy?
Some strategies used by Dr. Ng:
- Prepare food ahead of time
- Instant Pot/slow cookers for low glycemic index meals, such as meals with lentils and beans
- Easy and healthy snacks (such as nuts, cheese, avocado etc.); avoid protein or granola bars as they are high in sugar
- Bring a portable blender to make smoothies during a shift, incorporating elements such as yoghurt, fruits, and seeds
Matcha as an alternative to coffee?
- Matcha is a potential alternative to coffee before and during shifts; while they both contain antioxidants and caffeine, matcha contains L-theanine , which helps enhance calm alertness and cognitive enhancement without the caffeine crash that some coffee drinkers experience.
- Importantly, dairy may inhibit the antioxidant effect of matcha, so avoid drowning your matcha in milk.
What’s your take on restrained use of alcohol after a shift to wind down – good, bad or neutral?
- Alcohol has been shown to disrupt and fragment sleep, especially when used within a few hours of sleep onset; avoid alcohol after a shift as a ‘night cap’ before sleep
- The evidence for red wine in reducing cardiovascular risk is weak and the WHO recommends that no amount of alcohol is safe.
- Alcohol is classified as a group 1 carcinogen (on par with asbestos, tobacco, radiaton) by the International Agency for Research on Cancer.
Bottom line => Nutrition strategies for shift workers include avoiding eating large meals at night to prevent metabolic disruption, focus on low-glycemic foods to prevent insulin spikes and/or pair high glycemic index foods with fiber, fat, or protein. Consider switching from coffee to matcha to enhance calm alertness on shift, and minimize/eliminate alcohol use after shift.
None of the authors have any conflicts of interest to declare



Swami, as you know I love your content and your contributions to education in the field, but I have to keep pushing back on this. There are some potential pitfalls in the logic here, and I think we need to pump the brakes a little.
The effect size on first pass success in the 2024 Driver paper was small: 95.6% first pass success with NMB first vs 94.1% with sedative first, a 1.5% absolute difference in first pass success
You mention time of onset of these neuromuscular blockers, but what I think you’re really referring to is time to peak effect, meaning time to dense paralysis of large central muscles and respiratory muscles, resulting in optimal intubating conditions. This does indeed take about 45-60 seconds for succinylcholine or 60-70 seconds for high-dose rocuronium. But that’s not the onset. NMBs paralyze in a sequential manner, beginning with smaller groups like ocular and laryngeal, then limbs, then torso, then pharynx, then diaphragm. The onset of this process, and the time at which neuromuscular blockade is appreciable both by the patient and objective measurements, is as early as 15 seconds (PMID 21828347)
Awareness of paralysis, laryngoscopy, intubation, and ventilation are not meaningfully addressed in the above papers. The 2019 Driver paper does not assess it as an outcome, and calls awareness with paralysis “theoretical, albeit unlikely”, with which I would disagree. The ED AWARENESS study in 2021 (PMID 33485698) reported a recall of paralysis of 2.6%, and Driver himself in a larger 2024 study (PMID 36089069) found that 7.4% of patients were adjudicated to have possibly or definitely been aware during paralysis.
While we can likely never get these awareness and recall numbers to zero, or even achieve the very low levels of awareness and recall that can be achieved in the OR, I think at least most of us can agree that awareness during paralysis rates of 2.6%-7.4% in the ED are unacceptably high. I, for one, am going to have a VERY high bar to change my practice in a way that might increase that risk. A 1.6% improvement in first pass success, itself only a surrogate outcome (albeit an important one), just doesn’t tip that balance for me. If we had evidence that actual patient-oriented outcomes were meaningfully improved with a paralytic first strategy, that might be a different story.
Curious to hear other peoples’ thoughts. Thanks again for all the work you do!
I hear your caution and all reasonable. I would mention that in the Catoire article, they do reference OR studies looking at this offering additional data. The article also notes that, “the hypothetical risk of awake paralysis during paralytic-first induction has not been supported by experimental data either in the operating theater.” I share the concern about awareness during paralysis but I think it’s a greater issue of poor post-intubation sedation particularly with rocuronium.
While the benefit of paralytic first may be small, marginal gains in airway management are important.
Alternatively, you could simply provide good BVM or NIV during the apneic period. If you are following PREOXI, you probably don’t need to worry as much about this. That being said, many folks are reluctant to bag or provide NIV during apena for fear of aspiration though this concern appears overblown based on best data. I also see many folks attempting RSI well before the paralytic fully kicks in in the attempt to avoid a longer apneic time but this just invites more issues.