
Topics in this EM Quick Hits podcast
Justin Morgenstern on the evidence for nasogastric tubes in small bowel obstruction (0:52)
Jesse MacLaren on hyperacute T-waves and occlusion myocardial infarction (7:53)
Brit Long on malignant otitis externa (12:14)
Salim Rezaie on coronary CT angiography vs. invasive angiography in NSTEMI patients (18:23)
Justin Morgenstern on coronary CT angiography in low-risk chest pain (26:17)
Hans Rosenberg on Canadian syncope score (33:08)
Podcast: Play in new window | Download (Duration: 40:11 — 36.9MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman.
Podcast content, written summary & blog post by Raymond Cho and Anton Helman
Cite this podcast as: Helman, A. Morgenstern, J. MacLaren, J. Long, B. Rezaie, S. Rosenberg, H. EM Quick Hits 31 – NG Tubes in SBO, Hyperacute T Waves, Malignant Otitis Externa, CCTA, Syncope. Emergency Medicine Cases. August 2021. https://emergencymedicinecases.com/em-quick-hits-august-2021/. Accessed [date].
Is there evidence for nasogastric tube placement in management of small bowel obstruction?
- Nasogastric (NG) tubes are routinely placed in the ED to decompress the stomach when a small bowel obstruction (SBO) is diagnosed; however, there is no good evidence for the routine use of NG tubes in this situation, and they are rated as one of the most painful procedures in EM by patients
- There are no RCTs looking at the use of NG tubes in SBO; however, observational data suggests worse outcomes with NG tubes than without
- Fonseca 2013: 290 patients admitted with an SBO, 20% of them were managed without an NG tube. Use of an NG tube resulted in longer time to resolution, longer stay in hospital and higher rates of complications. Non-operative management was successful in 2/3 of patients regardless of NG tube placement
- Berman 2015: 181 patients admitted with an SBO, 1/2 were managed without an NG tube. No association between use of an NG tube and mortality, surgery or bowel resection. NG tube placement was associated with longer hospital stay
- Prophylactic NG tubes in post-op ileus is also a common practice; however, a systematic review of 28 studies found that ileus resolved faster in patients without NG tubes
Bottom Line: there is no high-quality evidence for the routine use of NG tubes in SBO. Observational data suggests that routine NG tube placement in SBO and post-op ileus results in worse outcomeEM s. Patients also report that NG tubes are among the most painful procedures done in the ED.
- Berman, D. J., Ijaz, H., Alkhunaizi, M., Kulie, P. E., Vaziri, K., Richards, L. M., & Meltzer, A. C. (2017). Nasogastric decompression not associated with a reduction in surgery or bowel ischemia for acute small bowel obstruction. The American Journal of Emergency Medicine, 35(12), 1919-1921.
- Fonseca, A. L., Schuster, K. M., Maung, A. A., Kaplan, L. J., & Davis, K. A. (2013). Routine Nasogastric decompression in small bowel obstruction: Is it really necessary? The American Surgeon, 79(4), 422-428.
- Nelson, R., Tse, B., & Edwards, S. (2005). Systematic review of prophylactic nasogastric decompression after abdominal operations. British Journal of Surgery, 92(6), 673-680.
Hyperacute T-waves and occlusion MI
Background
- Hyperacute T-waves are among the first signs of an acute coronary occlusion and NSTEMI, which helps with rapid diagnosis and may prevent delayed reperfusion
- T-waves can also be tall due to early repolarization, left bundle branch block, left ventricular hypertrophy, and hyperkalemia, so it is important to distinguish hyperacute T waves from other causes
Hallmarks of hyperacute T-waves
- Hyperacute T-waves are relative to the size of the QRS complex. These T waves are dynamic and generally as tall as or bigger than the preceding R-wave. For example, high-amplitude T-waves do not necessarily imply hyperacuity if the preceding QRS complex is also large; however, smaller T-waves may be hyperacute if the preceding QRS complex is also small
- Morphology, distribution, and associated changes can differentiate between occlusion MI and hyperkalemia. Hyperacute T-waves have broad bases and rounded peaks, are localized to an ischemic territory, and have other signs of occlusion MI (e.g., ST elevation, reciprocal ST depression). Hyperkalemia has peaked T-waves, which have a narrow base with a sharp symmetric peak, are diffuse, and have other signs of hyperkalemia (e.g., prolonged PR and QRS intervals)

Hyperacute T-waves of early MI. Note the broad-based, rounded peaks of T-waves to help distinguish from peaked T waves of hyperkalemia. Care of Life in The Fast Lane blog.

Peaked T-waves of Hyperkalemia. Note the narrow base, symmetric, and pointy peak and that the amplitude of the T exceeds the amplitude of the R. Care of Life in The Fast Lane blog.
Bottom Line: If you see tall T-waves in a patient with ischemic symptoms, compare the T-wave to the preceding QRS, assess the morphology and compare to an old ECG. If the T-wave is hyperacute and in a regional distribution with reciprocal changes, you can make a provisional diagnosis of an occlusion MI.
ECG Cases 21 for more examples of hyperacute T-waves
- Dressler, W., & Hugo, R. (1947). High T waves in the earliest stage of myocardial infarction. American Heart Journal, 34(5), 627-645.
- Goldberger, A. L. (1982). Hyperacute T waves revisited. American Heart Journal, 104(4), 888-890.
- MacLaren, J., & Helman, A. (2021, May 4). ECG cases 21: Hyperacute T-waves and occlusion MI. Emergency Medicine Cases. https://emergencymedicinecases.com/hyperacute-t-waves-occlusion-mi/
- Somers, M. P., Brady, W. J., Perron, A. D., & Mattu, A. (2002). The prominent T wave: Electrocardiographic differential diagnosis. The American Journal of Emergency Medicine, 20(3), 243-251.
Malignant otitis externa
- Malignant otitis externa is “swimmer’s ear” that spreads outside of the ear – a progressive infection of the external auditory canal that spreads to the skull base leading to osteomyelitis, cerebral abscess, and death (20% mortality rate)
- Risk factors: age > 65, diabetes and immunocompromise
- Pseudomonas is the dominant microbe, but klebsiella and MRSA account for 15% of cases
- Patients present with severe ear pain out of proportion to exam, but often do not have a fever
- The tympanic membrane is generally normal (if it is not visually blocked by severe canal swelling), but you may see a swollen and tender external auditory canal with purulent otorrhea, granulation tissue and even exposed bone
- More extensive disease may cause cranial nerve deficits; CN7 palsy occurs in 25% of patients

Severe otorrhea of malignant otitis externa (source: AJEM)
- Lab: WBC is typically normal, but inflammatory markers such as CRP/ESR may be elevated; cultures of the purulent material is critical for subsequent management
- Imaging: CT temporal bones with contrast may show bony erosion, decreased density of the skull base or abscess formation. If the CT is negative but you have a high pretest probability, consider MRI as this may show early soft tissue involvement
- Antibiotics: consider pseudomonal coverage with fluoroquinolones (eg., ciprofloxacin) in patients who appear well; in those who appear toxic, broader agents with pseudomonal coverage like cefepime, meropenem or pip-tazo may be used. Consider discussing the case with your ID colleagues and ensure that a culture is obtained
- Disposition: patients who appear systemically well, are not immunocompromised, have no facial palsy, pain is well-controlled, ID is on board and have ENT follow-up can be considered for discharge
- Long, D. A., Koyfman, A., & Long, B. (2020). An emergency medicine-focused review of malignant otitis externa. The American Journal of Emergency Medicine, 38(8), 1671-1678.
Coronary CT angiography vs. invasive angiography in NSTEMI patients
- Invasive coronary angiography (ICA) is the gold standard to assess the level of obstructive coronary artery disease (CAD) in NSTEMI. However, a routine invasive strategy is associated with increased bleeding, iatrogenic injury and prolonged hospital stay. Coronary CT angiography (CCTA) is a non-invasive test that can potentially rule out CAD. However, the prognosis and extent of CAD in patients with NSTEMI using CCTA compared to an invasive strategy is unknown
- Paper: Kofoed KF et. al. Prognostic Value of Coronary CT Angiography in Patients with Non-ST-Segment Elevation Acute Coronary Syndromes. JACC 2021.
- Definitions
- Obstructive: > 1 coronary artery with ≥ 50% stenosis (i.e., CAD severity)
- High-risk: obstructive left main or proximal LAD stenosis, and/or multivessel disease (i.e., CAD extent)
- Clinical Question: Is CCTA equivalent to ICA for risk assessment in NSTEMI patients?
- This data is an observational component of the VERDICT trial, in which 978 patients received a CCTA prior to invasive coronary angiography
- Primary outcome: composite of all-cause mortality, non-fatal recurrent MI, hospital admission for refractory ischemia, hospital admission for heart failure
Results
- 978 patients had CCTA and angiography performed, and primary endpoint happened in 208 patients (21.3%)
- Rate of primary endpoint was 1.7x higher in patients with obstructive CAD (HR: 1.74; 95% CI 1.22 to 2.49; p = 0.002) and 1.5x higher in patients with high-risk CAD (HR 1.56; 95% CI 1.18 to 2.07; p = 0.002), as defined by the CCTA. Subsequent ICA did not identify patients at increased risk among patients with non-obstructive or non-high-risk CAD by CCTA
- There was no difference in mortality based on CAD severity or CAD extent using ICA or CCTA
- CCTA was equivalent but not identical to ICA for assessment of long-term risk in patients with NSTEMI as more obstructive disease was identified in CCTA than in ICA.
Bottom Line: CCTA can identify severity and extent of CAD in an equivalent fashion to ICA when assessing the long-term risk in patients with NSTEMI. However, without individual patient data, this observational study does not guide decision-making at the bedside and we should not substitute CCTA for ICA based on this data.
- Kofoed, K. F. (2021). Prognostic Value of Coronary CT Angiography in Patients with Non-ST-Segment Elevation Acute Coronary Syndromes. Journal of the American College of Cardiology, 77(8), 1044-1052.
- Long, D. A., Koyfman, A., & Long, B. (2020). An emergency medicine-focused review of malignant otitis externa. The American Journal of Emergency Medicine, 38(8), 1671-1678.
Coronary CT angiography in low-risk chest pain
- For patients who present to the ED with chest pain and have normal ECGs and negative troponin(s), the risk of death or MI in the next 3-6 months in these low-risk patients is 2/1000
- Patients are likely to benefit from risk factor modification, however studies suggest that low-risk patients in whom we use CCTA do not benefit from invasive angiography
- None of the trials looking at the utility of CCTA in low-risk patients showed improved patient-oriented outcomes
- In the 6 RCTs looking at CCTA in ED patients (n = ~4500), there was 1 death (in CCTA group) and 12 MIs (4 in CCTA group and 8 in standard of care group); there was no statistically significant difference in outcomes
- A meta-analysis in 2018 looking at 10 trials showed no statistical benefits of CCTA.; more patients are sent for invasive management in the CCTA group which may cause harm due to radiation and additional interventions
Bottom Line: CCTA should not be used routinely in low-risk patients as it does not improve outcomes and may lead to harm. There may be a role for CCTA in higher-risk patients (i.e., NSTEMI) but further research is required before widespread implementation.
- Dedic, A., Lubbers, M. M., Schaap, J., Lammers, J., Lamfers, E. J., Rensing, B. J., Braam, R. L., Nathoe, H. M., Post, J. C., Nielen, T., Beelen, D., Le Cocq d’Armandville, M., Rood, P. P., Schultz, C. J., Moelker, A., Ouhlous, M., Boersma, E., & Nieman, K. (2016). Coronary CT angiography for suspected ACS in the era of high-sensitivity troponins. Journal of the American College of Cardiology, 67(1), 16-26.
- Goldstein, J. A., Chinnaiyan, K. M., Abidov, A., Achenbach, S., Berman, D. S., Hayes, S. W., Hoffmann, U., Lesser, J. R., Mikati, I. A., O’Neil, B. J., Shaw, L. J., Shen, M. Y., Valeti, U. S., & Raff, G. L. (2011). The CT-STAT (Coronary computed tomographic angiography for systematic triage of acute chest pain patients to treatment) trial. Journal of the American College of Cardiology, 58(14), 1414-1422.
- Gongora, C. A., Bavishi, C., Uretsky, S., & Argulian, E. (2017). Acute chest pain evaluation using coronary computed tomography angiography compared with standard of care: A meta-analysis of randomised clinical trials. Heart, 104(3), 215-221.
- Hamilton-Craig, C., Fifoot, A., Hansen, M., Pincus, M., Chan, J., Walters, D. L., & Branch, K. R. (2014). Diagnostic performance and cost of CT angiography versus stress ECG — A randomized prospective study of suspected acute coronary syndrome chest pain in the emergency department (CT-COMPARE). International Journal of Cardiology, 177(3), 867-873.
- Hoffmann, U., Truong, Q. A., Schoenfeld, D. A., Chou, E. T., Woodard, P. K., Nagurney, J. T., Pope, J. H., Hauser, T. H., White, C. S., Weiner, S. G., Kalanjian, S., Mullins, M. E., Mikati, I., Peacock, W. F., Zakroysky, P., Hayden, D., Goehler, A., Lee, H., Gazelle, G. S., … Udelson, J. E. (2012). Coronary CT angiography versus standard evaluation in acute chest pain. New England Journal of Medicine, 367(4), 299-308.
- Litt, H. I., Gatsonis, C., Snyder, B., Singh, H., Miller, C. D., Entrikin, D. W., Leaming, J. M., Gavin, L. J., Pacella, C. B., & Hollander, J. E. (2012). CT angiography for safe discharge of patients with possible acute coronary syndromes. New England Journal of Medicine, 366(15), 1393-1403.
- Morgenstern, J. (2019, November 4). CCTA doesn’t help: The evidence. First10EM. https://first10em.com/ccta-evidence/
Canadian Syncope Score validated in Canada
When to use the Canadian Syncope Risk Score
- Ensure that the patient had a syncopal episode rather than a mimic (e.g., vertigo)
- Ensure that there are no other serious underlying conditions that require further investigation
Canadian Syncope Risk Score
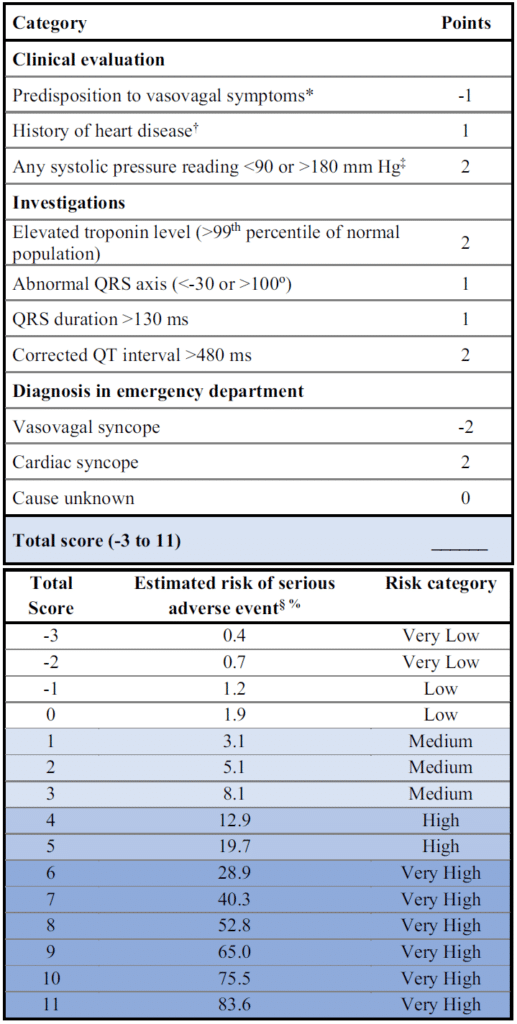
Canadian Syncope Risk Score (source: CJEM)
- The Canadian Syncope Risk Score calculates the 30-day risk of a serious outcome, which includes death, arrhythmias, MI, dissection, structural heart disease and noncardiac syncope (e.g. PE, subarachnoid hemorrhage, bleed, sepsis).
- Very low-risk (0.2% risk of serious outcome) and low-risk (0.7%): can be safely discharged home after 2 hours of ED observation
- Medium-risk (8% risk of serious outcome, 1% risk of death): consideration for discharge home can be made after 6 hours of ED cardiac monitoring, outpatient cardiac rhythm monitoring and good return to ED instructions
- High-risk (30.6% risk of serious outcome): may benefit from admission and at minimum, requires 6 hours of ED monitoring and outpatient cardiac rhythm monitoring.
- A subsequent multicenter external validation study in Italy published in May 2021 suggested that in their patient population the Canadian Syncope Score performed no better than physician gestalt, highlighting the need for further study and the need for questioning whether your patients are similar to the patients in the studies (REBELEM interpretation of this study)
Ep 172 Syncope Simplified with David Carr
- Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. CMAJ. 2016;188(12):E289-98.
- Thiruganasambandamoorthy V, Sivilotti MLA, Le sage N, et al. Multicenter Emergency Department Validation of the Canadian Syncope Risk Score. JAMA Intern Med. 2020.
- Rosenberg, H., Nath, A., & Thiruganasambandamoorthy, V. (2021). Just the facts: How to assess a patient presenting to the emergency department with syncope. Canadian Journal of Emergency Medicine, 23(3), 286-290.
- Solbiati M, et al. Multicentre external validation of the Canadian Syncope Risk Score to predict adverse events and comparison with clinical judgement. Emerg Med J. May 2021.
- Mark Ramzy, “External Validation of the Canadian Syncope Risk Score”, REBEL EM blog, July 8, 2021. Available at: https://rebelem.com/external-validation-of-csrs/.
None of the authors have any conflicts of interest to declare



What do you do with new onset angina that occured 6 hours ago in a smoking with a family history of heart disease ?
If the pain lasted 10 minutes there will be likely no ECG changes or troponin 0 and 3 hour elevation .
Do you cath him or is CCTA plus or minus stress test better .
The other is the 60 year old with a 5 year risk of cardiovascular disease greater than 20% on the Risk Scores and with a family histoty .
Wait for angina or infarct or sudden death or do a CCTA .