
Topics in this EM Quick Hits podcast
Deborah Schonfeld on pediatric torticollis (02:33)
Anand Swaminathan on stable wide-complex tachycardia (28:24)
Andrew Petrosoniak on post-intubation neurocritical care considerations (33:45)
Justin Morgenstern on correcting hyponatremia (42:39)
Andrew Tagg on paronychia management (53:09)
Victoria Myers and Judith Tintinalli on Women in EM leaders series (1:00:00)
Podcast: Play in new window | Download (Duration: 1:31:24 — 83.7MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Brandon Ng, edited by Anton Helman, July, 2025
Cite this podcast as: Helman, A. Schonfeld, D. Swaminathan, A. Petrosoniak, A. Morgenstern, J. Tagg, A. Myers, V. Tintinalli, J. EM Quick Hits 66 – Pediatric Torticollis, Stable Stable Wide Complex Tachydysrhythmias, Post-intubation Neurocritical Care, Hyponatremia Correction Rates, Paronychia Management, Women in EM Leader Series with Judith Tintinalli https://emergencymedicinecases.com/em-quick-hits-july-2025/. Accessed August 3, 2026.
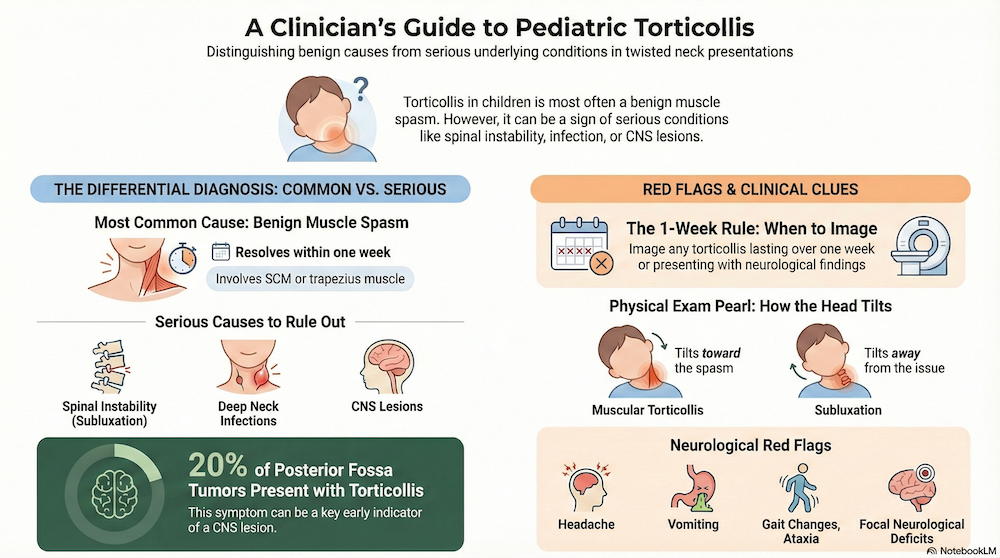
Pediatric torticollis: Not just muscular injury

Broad Categories in the differential diagnosis of pediatric torticollis
-
Muscular (SCM/trapezius): Most common; typically resolves within a week.
-
Atlantoaxial Subluxation: C1/2 instability due to ligamentous or osseous abnormalities.
-
Infectious:
- Viral URTI/Pharyngitis → Referred pain, muscle spasm
- Retropharyngeal Abscess (typically ages 2–4): Limited neck extension, fever, dysphagia, drooling, stridor
- Osteomyelitis/Discitis: Cervical spine tenderness
- Lemierre Syndrome: IJ thrombophlebitis post-oropharyngeal infection → SCM or jugular tenderness/swelling
-
CNS Lesion (typically painless):
- Up to 20% of posterior fossa tumors present with torticollis
- 50% of pediatric malignant brain tumors are located in the posterior fossa
- Clinical red flags: headache, vomiting, gait changes, ataxia, focal neuro deficits
Atlantoaxial Subluxation
Risk Factors for Atlantoaxial Subluxation
- Ligamentous injury (more common than fracture in children)
- Congenital hypermobility: Trisomy 21/Down syndrome, Marfan’s Syndrome, Juvenile Idiopathic Arthritis
- Grisel Syndrome: Post head/neck surgery with local inflammation → ligament laxity
Physical exam pearl to distinguish atlatoaxial subluxation from muscular torticollis
- Muscular torticollis: Head tilts toward spastic SCM
- Subluxation: Tilts away from affected side
Imaging for suspected atlantoaxial subluxation
-
XR: Odontoid and lateral views; assess Atlantodental Interval (≤5 mm if <8 years) – use as screening in low pretest probability patients; be aware than sensitivity is poor
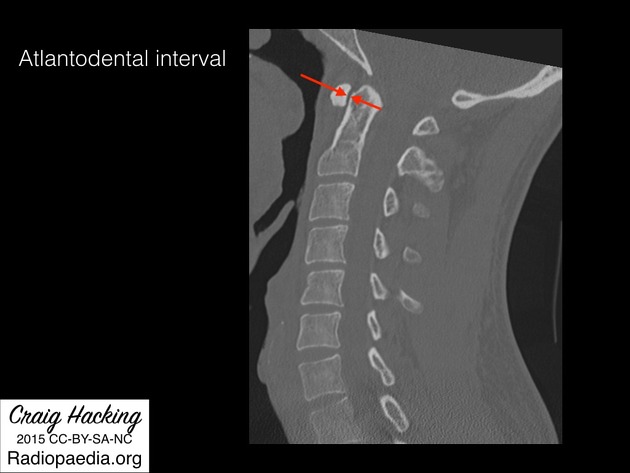
Source: Radiopaedia under the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported licence
-
CT: Gold standard when high suspicion or red flags present
Bottom Line
- Most cases of torticollis self-limiting, due to SCM muscle spasm
- Torticollis >1 week or with neurological findings → Image to rule out subluxation, infection, or CNS lesion
- McInerny, Thomas K, and American Academy of Pediatrics. American Academy of Pediatrics Textbook of Pediatric Care. Washington, D.C: American Academy of Pediatrics, 2009. Print.
Approach to Stable Wide-Complex Tachydysrhthmias
Regular, Wide, Fast Tachycardia? Assume VT.
Rhythms >120 bpm that are regular, wide, and fast are usually Ventricular Tachycardia (VT)—rarely SVT with aberrancy.
In unstable patients, decision making is typically straighforward with immediate electrical cardioversion.
When stable, we may be tempted to reach for diagnostic algorithms to distinguish VT vs. SVT—but:
- Algorithms are ≤80% accurate
- They waste precious time
- Patients may decompensate rapidly
Rapid approach:
Assume regular wide-complex tachycardia (>110–120 bpm) is VT.
- VT treatment works for SVT with aberrancy—not the reverse.
- Consider hyperkalemia if rate <110 bpm.
Management:
- Treat with electrical cardioversion in all cases unless contraindicated.
- ACLS suggests chemical cardioversion, but efficacy is variable.
- Procainamide is more effective than amiodarone (67% vs. 38% success, Ortiz et al. 2017).
- 200 J biphasic is safe and most effective.
- Use light sedation (e.g., propofol or etomidate) if patient is alert.
Bottom Line
In any hemodynamically stable patient with regular, wide, fast tachycardia, skip the guessing—electrical cardioversion is your safest and fastest option.
ECG Cases 19 – Tachycardias: Approach, WIDER mnemonic for Wide SVT DDx, VT vs SVT
Episode 112 Tachydysrhthmias with Amal Mattu & Paul Dorian
- Ortiz M, Martín A, Arribas F, Coll-Vinent B, Del Arco C, Peinado R, Almendral J; PROCAMIO Study Investigators. Randomized comparison of intravenous procainamide vs. intravenous amiodarone for the acute treatment of tolerated wide QRS tachycardia: the PROCAMIO study. Eur Heart J. 2017 May 1;38(17):1329-1335.
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline For The Management Of Adult Patients With Supraventricular Tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2016;133:e506-e574.
- Vereckei A. Current algorithms for the diagnosis of wide QRS complex tachycardias. Curr Cardiol Rev. 2014 Aug;10(3):262-76.
Post-intubation Neurocritical Care: 5 Non-pharmacologic and 4 pharmacologic best practices
Securing the airway in head-injured patients is only the beginning; meticulous post-intubation care optimizes neurologic outcomes.
Non-pharmacologic best practices:
- Head elevation (≈ 30°) or reverse Trendelenburg to lower ICP by ~ 5 mm Hg and reduce aspiration risk
- Loosen C-spine collar or switch to an aspen collar to prevent pressure sores and ICP elevation
- Gastric decompression using OG tube to reduce discomfort/pain
- Bladder decompression using foley catheter to reduce discomfort/pain
- Early arterial line placement for continuous BP monitoring (BP variability worsens outcomes)
Pharmacologic best practices:
- Propofol infusion is preferred over benzodiazepines (allows rapid on/off of sedation for neuro exams)
- Have boluses of sedatives (e.g. propofol) ready immediately post intubation, as infusion pumps are not always adequate
- Consider norepinephrine to maintain BP targets if propofol causes mild hypotension
- Alternatives include switching sedatives to ketamine or IV fluid boluses
- Use opioid boluses rather than continuous infusions for analgesia to avoid accumulation, delirium, hyperalgesia
- Fentanyl 25–50 µg, then hydromorphone 1–2 mg IV after obtaining CT
Bottom line => After securing the airway, focus on 5 pharmacologic and 4 non-pharmacologic best practices to deliver optimal post-intubation neurocritical care.
Hyponatremia correction rates: Has the slow correction rate dogma been debunked?
The Paper: Correction Rates and Clinical Outcomes in Hospitalized Adults With Severe Hyponatremia: A Systematic Review and Meta-Analysis by Ayus et al. JAMA Intern Med 2025.
Traditional caution against rapid sodium correction (due to osmotic demyelination syndrome, ODS) may inadvertently increase mortality.
- P: 16 studies, n = 11811 with severe hyponatremia (Na < 120 or < 125 + severe symptoms)
- I/C: hyponatremia correction at rates of rapid (> 8–10 mEq/L/24 h); slow (< 8); very slow (< 4–6)
- O: slow and very slow correction was associated with 32 (3.2% absolute increase) and 221 (22% absolute increase) additional in-hospital deaths per 1000 patients, respectively, compared to rapid correction. There were no statistically significant differences in risk of ODS between groups with different correction rates (< 1% across all correction speeds).
Additional considerations:
- The paper does not have access to underlying patient data that informs potential confounding factors (e.g. reason for hyponatremia, reason for treatment at different rates)
- Slower treatment groups may have higher rates of cirrhosis, heart failure, metastatic cancer, which may act as confounding factors, amongst many others
- Limited quality evidence warrants further data from studies including RCTs
- Other studies suggest that there is a strong correlation between baseline health conditions and demyelination
Bottom line => While awaiting RCTs, don’t let fear of ODS (rare) drive overly slow correction that may increase mortality; prioritize life-threatening symptoms and consider faster correction.
- Ayus JC, Moritz ML, Fuentes NA, Mejia JR, Alfonso JM, Shin S, Fralick M, Ciapponi A. Correction Rates and Clinical Outcomes in Hospitalized Adults With Severe Hyponatremia: A Systematic Review and Meta-Analysis. JAMA Intern Med. 2025 Jan 1;185(1):38-51. doi: 10.1001/jamainternmed.2024.5981.
- Verbalis JG, Goldsmith SR, Greenberg A, Korzelius C, Schrier RW, Sterns RH, Thompson CJ. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013 Oct;126(10 Suppl 1):S1-42.
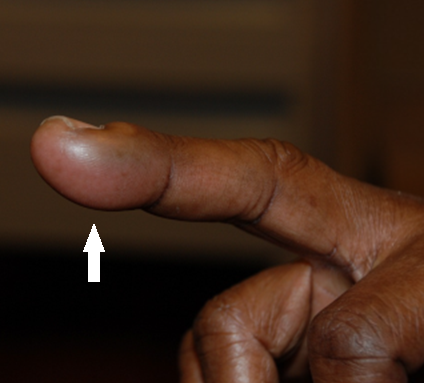
Paronychia Management
Acute or chronic nail-fold infections are common in children and often overtreated with antibiotics.
Acute paronychia:
- Usually bacterial (Staph aureus, Strep pyogenes) after minor trauma (nail biting, splinters)
- Presents as painful, red, swollen lateral nail fold ± fluctuant abscess
- Complications include cellulitis, osteomyelitis, chronic nail changes, and systemic infections (particularly if immunocompromised)
- Management: warm soaks × 10 min, then drain the pus by lifting the lateral nail fold with a fine needle
- Consider oral antibiotics (e.g., cephalexin, clindamycin) only if surrounding cellulitis, lymphangitis and/or immunocompromise
Chronic paronychia:
- From repeated moisture or irritant exposure (e.g. hand washing, eczema)
- Management: trigger avoidance (e.g. keep hands dry, barrier creams), manage underlying dermatological conditions, treat secondary infections.
- Refer to dermatology if persistent
Mimics of paronychia:
- Herpetic whitlow (HSV blister) → antivirals

Herpetic Whitlow. Source – Wikipedia
- Felon (deep fingertip abscess) → I&D
Felon. Source: Northwestern Medicine
- Acrodermatitis continua of Hallopeau (pustular psoriasis) → dermatology referral

Source: huidarts.com
Bottom line => Drain acute paronychia promptly and reserve antibiotics for cellulitis/secondary infections. Prevent chronic cases with trigger avoidance and education. Consider mimics of paronychia.
- . How I drain a paronychia: getting the pus out, Don’t Forget the Bubbles, 2021. Available at: https://doi.org/10.31440/DFTB.34608.
Women in EM Leaders Series: Dr Judith Tintinalli
Leadership pearls:
- Support your team through successes and failures
- Set an example for your team: e.g. clinical excellence, team dynamics, punctuality, preparedness
- Prioritize time management for yourself and for others
- Reinforce the importance of team dynamics and everyone’s equally important role in a team
- Active listening and invite others for their opinion
- Get things done: keep an agenda, track progress
Tips for practice expansion:
- Plan goals in 5-year blocks
- Pursue advanced training (e.g. fellowships, MPH, MBA)
- Stay clinically active: clinical practice can be a reliable source of income in case of changes to other career pathways; also helps to keep up with clinical updates and makes you better appreciate the problems and experiences faced in the ED.
- Work with individuals outside of Emergency Medicine: helps to learn to communicate in other professional “languages”
- Expand your practice (e.g. through telemedicine, ultrasound, public health, and cross-disciplinary collaborations)
Bottom line => Don’t be afraid to try and pursue the things you are interested in. Bold initiative, continuous learning, and genuine support for colleagues form the foundation of transformative EM leadership.
- Lin MP, Cooper RJ. Emergency Medicine: A Career or Just a Pit Stop? Ann Emerg Med. 2025 Jun;85(6):489-490. doi: 10.1016/j.annemergmed.2025.03.022. Epub 2025 Apr 24. PMID: 40272327.
None of the authors have any conflicts of interest to declare



Regarding the quick-hit on ventricular tachycardia: Always consider hypomagnesemia as an etiology. Of course, we should all think of hypomagnesemia in the setting of polymorphic VT, but it can accompany monomorphic VT and perhaps in particular, repetitive monomorphic VT https://onlinelibrary.wiley.com/doi/10.1111/j.1540-8159.2009.02527.x
So here’s a case from last week’s shift at a free-standing (U.S. based) critical access ED (one doc in the facility, 2 nurses). 70+ y.o. pt wheeled in by family feeling weak, sob; 2 weeks s/p pneumonectomy at center 1.5 hours away and hx CAD, former smoker. awake, conversant, SBP 110, sat OK; Monitor shows sustained regular wide complex tachycardia with occasional very short runs narrow complex, slightly slower rate. 12 lead wide complex @162/min w little variation in QRS, 4 beats sinus tach (p wave, narrow 140’s). She’s had diarrhea for several days and was just started on a thiazide diuretic. Mg 2 g IV administered as soon as the IV inserted/blood drawn. Runs of VT less frequent and shorter. Additional Mg administered and all VT extinguished. Serum Mg 1.2 (not terribly low, but low) and K was 3.3 (repleted as well.
Most VT should get “Edison” but cardioversion was not her problem; it was maintaining sinus.
Think magnesium
Great case. The presence of narrow complex beats and p waves should definitely make you consider alternate pathologies as you’ve pointed out!
As always, thank you for all your incredible work!!
About the stable wide-complex tachycardia, in case of cardioversion for all: one risk here that is common and not mentioned is potentially converting a non-anticoaguled atrial fibrillation or fludder with a background abbarency. As these at least in my practise are more common than stable VTs this is our main argument against cardioverting everyone (and also from our cardiologists). Instead when in doubt the practise here is to do a diagnostic oesophageal ECGs (don’t know any but studies in this though and it may not be better than other algorithms). Another is what the initial ERC 2021 (later changed in the current 2021 edition) and the ESC VT 2022 guideline figure 9, is giving adenosine as a test (main risk here is pre excited atrial fibrillation with WPW – but with pads on you can probably quickly terminate any potential malignant arytmia)
So despite your excellent talks from Anand and Amal Mattu earlier on the topic, saying the same thing , I don’t feel this issue (ie the non-anticoaguled patient), has been addressed and therefore I cannot applicate it in my practise. And as a result I always find these patients difficult as it’s a “damned if you do, damned if you don’t”-scenario . I might be missing something here ?
If it’s AF, you should see some irregularity which removes you from VT as a consideration.
AFlutter w/ abberancy can definitely mimic VT but, you should be able to see flutter waves. If in doubt, you can try speeding up the ECG tracing and see if flutter waves become more pronounced. I’m not a fan of adenosine or any AV nodal blocker because you run the risk of breaking certain types of VT and, if broken, the chance of someone discharging that patient instead of admitting for further workup is considerable. However, if your plan is, “I’m gonna give adenosine and whether this breaks or not, I’m admitting the patient to tele for cards evaluation and work up,” I’ve got less of a problem.
A few weeks out from listening to this podcast on minor treatment shift yesterday… guy came in because a box of avocados fell on his head at work GP had done cervical spine films which were normal, but the guy came in with torticollis… interestingly though he was favouring the right side, but had a lot of tenderness on his right side …
his CT showed right sided C5 C6 fractures…
…appreciate the pearl on the head turning towards the painful side being a red- flag, as it was very true in this case!